Originally published on Ultrasound G.E.L. on 11/23/20 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from Ultrasound G.E.L. team!

Screening of Embolic Sources by Point-of-Care Ultrasound in the Acute Phase of Ischemic Stroke
Ultrasound Med Biol Sept 2020 – Pubmed Link
Take Home Points
1. A focused echo can be sensitive and specific for sources of embolism in ischemic stroke.
2. It is unclear if this practice could lead to improvements in meaningful patient centered outcomes.
Background
We know that strokes are a large cause of morbidity. A good portion of them are caused by an embolism that originates in the heart. This can be due to atrial fibrillation, ventricular dysfunction, or valvular pathologies. Obtaining a comprehensive echocardiogram is part of the standard stroke work up in many centers. This study takes a look at doing this echo a little bit earlier in the course of stroke, at the point-of-care. Are there certain patients that this could benefit?
Questions
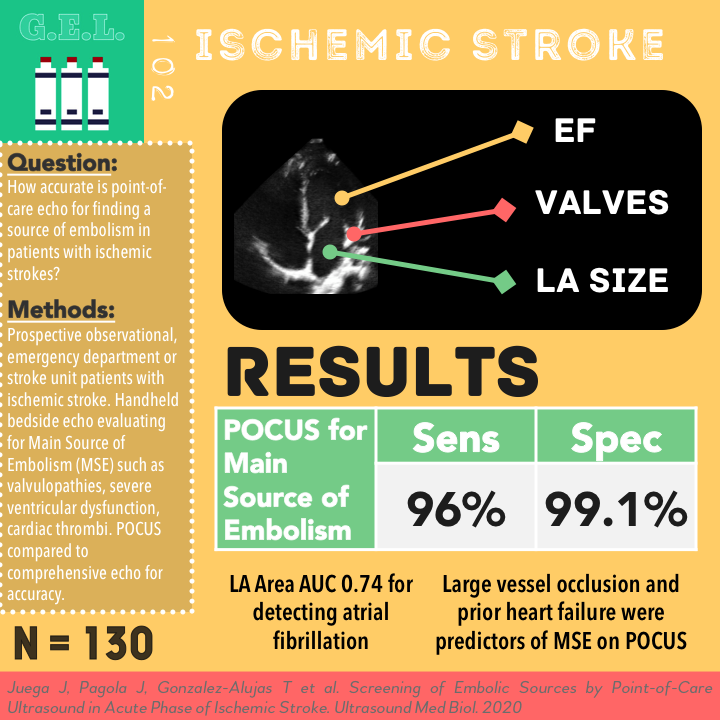
How accurate is a point-of-care echo for finding a source of embolism in patients with ischemic strokes?
What subset of patients with acute stroke would benefit from a screening point-of-care echocardiography?
Population
Single center (presumably a stroke center, but not specified)
Does not specify geographic location. Most authors work in Spain, one in Chile.
Inclusion:
- Non-lacunar Ischemic stroke patients admitted to emergency department or stroke unit
Exclusion:
- Poor echocardiographic windows
- Clinical instability
- Any condition that did not allow an echo
- Lost in follow up
- Stroke mimics
- Brain hemorrhage or tumor
Design
Prospective observational
Patients with stroke identified. Evaluated within first 24 hours of stroke onset
All patients underwent CT, CT angiography (or actual arteriography)
They categorized patients into two groups after this: those with a determined etiology and those with undetermined etiology. Determined etiology was decided based on those in whom the initial imaging work up revealed a cardioembolic stroke or large arterial atherosclerosis stroke defined as symptomatic >50% stenosis or occlusion. This seemed to include those that had a history of atrial fibrillation, prosthetic valves.
In both groups, they performed a bedside echo looking for a predictor of a Main Source of Embolism (MSE) or an enlarged left atrium. Later they obtained cardiac monitoring for atrial fibrillation detection as well.
The physician performing the echo was blinded to the medical record. This physician assessed for MSEs- defined as embolic valvulopathies (EVs) or severe ventricular dysfunction (SVD). EVs included masses, endocarditis, fibroelastoma, prosthetic valves, rheumatic mitral valve stenosis. SVD defined as severe LV systolic dysfunction (estimated <30%) and intracardiac masses or thrombi. LV systolic dysfunction, mitral stenosis, and left atrial dilation.
All patients underwent a transthoracic echo (TTE) examination within 72 hours.
The POCUS was compared to the TTE for accuracy of detecting MSEs. In a few cases they did TEE (suspected complex aortic atheromatosis or patent foramen ovale).
Their detection of atrial fibrillation was compared to hospital telemetry for up to 1 year from hospital discharge.
In looking at their patient flow chart, it seemed their diagnostic thought process was thus:
- First exclude those with clear causes (known embolic source or a large atherosclerotic stroke)
- Look at subgroups of those with LVO and those without
- Identify those who had an MSE
- If they did not have MSE, then it was more important to assess the left atrial area and look for atrial fibrillation
Who did the ultrasounds?
A single stroke neurologist who had been trained for 1 year in focused echocardiography (>350 echos supervised by an expert)
The Scan
Phased Array (technically a hand-held though)

They used a hand-held ultrasound (GE Vscan) → could perform exam in ED, stroke unit, CT suite, angiography suite
It appears they obtained the four standards focused echo views (parasternal long, parasternal short, subcostal, apical four chamber) but also added an apical 2 chamber.
Focused Echo for Stroke Sources (the study ultrasound protocol)
- LV Function – assessed ejection fraction (EF) qualitatively on apical 4 and 2 chamber views. Classified as normal EF (>50%), moderately reduced (30-50%), severely reduced (<30%)
- Valves – mitral stenosis suspected based on visualized reduced mobility of mitral valve + color aliasing (looked for turbulent flow on B-mode and color doppler)
- Left Atrium – diameter measured in parasternal long axis. Left atrial area – measured in apical four chamber view (>20cm2 considered enlarged)
Learn how to do Cardiac Ultrasounds from 5 Minute Sono!

Check out Cardiac Pathology on the POCUS Atlas!

Results
N = 130
- 14 exclude for poor windows (this was 54% of total excluded), 8 lost to follow up, 3 stroke mimics
- 18.5% (n = 24) of these had a known cause after initial work up (prior to POCUS)
- 19.23% of these patients had an Main Source of Embolism discovered ultimately (7 had EV, 17 had SVT, 1 had both)
- For those with unknown etiology, median age 74, 50% female, plenty of risk factors, 17.3% had prior stroke, median NIHSS 8, 53.8% had LVO, 49% got alteplase, 34.6% endovascular treatment
Primary Outcome – Test characteristics of point of care (hand held) echo compared to comprehensive TTE
MSEs (SVDs + EVs) n = 25
Sensitivity 96% (CI 77.68-99.79)
Specificity 99.05% (CI 94.04-99.95)
K 0.95 (0.88-1)
SVDs n = 18
Sensitivity 94.44% (CI 70.62-99.71)
Specificity 99.11 (CI 94.40-99.95)
K 0.93 (0.84-1)
EVs n = 8
Sensitivity 87.50% (CICI 47.35-99.68)
Specificity 100% (CI 97.02-100)
K 0.92 (0.79-1)
Overall – really sensitive and specific. More specific with better confident intervals. The sensitivity for EVs was hurt because they had a false negative and there were only 8 total.
Secondary Outcomes
LA Area to Detect AF – AUC 0.74 (CI 0.64-0.85)
LA area > 20 cm2
Sensitivity 83.3%
Specificity 62.7%
Other Findings
There were only 2 misdiagnoses with POCUS
- False negative: 1 patient had a papillary fibroelastoma that was missed (EV)
- False positive: 1 mild dysfunction was called a severe ventricular dysfunction
57% of POCUS was within first 6 hours from stroke onset
Average duration of POCUS was 9.2 minutes (SD 5.3 min)
22% of SVD was classified as “transient” embolic source
LA diameter and area was larger in patient in whom AF was detected (4.5 vs 4 cm, and 22.3 vs 18.6 cm2)
On multivariate analysis, LVO and previous Heart failure were independent predictors of MSEs
- LVO – OR 4.24 (CI 10.01-17.85)
- CHF – OR 13.25 (CI 3.54-49.50)
Strengths
Prospective
Novel protocol
Extensive follow-up (up to 1 year after stroke to assess for atrial fibrillation)
Clever use of hand-held ultrasound
Limitations
This is a single center study. Their population had a relatively high percentage of MSEs. These findings might not apply to the population of stroke patients seen by everyone.
This was a study of one, fairly well trained neurologist. Many of the findings they studied are outside of what is generally considered the scope of a “focused” echo. Many point-of-care ultrasound practitioners are likely not trained in finding cardiac thrombi, subtle valvular abnormalities, or measuring cardiac chambers.
Discussion
A few other things it would have been nice to know. They excluded patients with poor echocardiographic windows – did cardiology have limited windows on those patients or are we seeing a different subset of patients in this study? They did not discuss using contrast (to assist with visualization of endocardial border for EF or assessment of thrombus). They also did not mention doing a shunt test with bubbles. Why was NIH of ≥8 considered moderate but ≥9 was severe? So only NIH 8 was actually moderate? They do site a reference but this would affect how they analyzed the different severities (although they do group moderate and severe often). Also – it would have been nice to have a second POCUS investigator review the scans for accuracy or agreement. This is helpful information when it is a novel application.
What is the point? What is the advantage of doing an ultrasound to discover a source of the stroke earlier? The authors state that delayed echo can miss some transient causes of the stroke, so a POCUS in the acute phase might be more sensitive. They wanted to find causes that would benefit from anticoagulation. Their second point is with regard to atrial fibrillation. Their reasoning here is that since an enlarged left atrium is associated with higher risk of atrial fibrillation, these patients might warrant longer electrocardiographic monitoring if no other cause for the stroke is found. Despite all this – I am not sold that this time savings will lead to a meaningful patient centered outcome. A benefit would hinge on finding that earlier anticoagulation in these patients (on the scale of 1-2 days earlier) reduces negative outcomes. Keep in mind that 76.5% of their patients with MSE received thrombolytics. Also, there is no reason that comprehensive echoes can’t be done soon in some centers. All that to say, I think a significant benefit is theoretically possible, but somewhat far-fetched.
Summary
Prospective observational study of 130 patients with non-lacunar ischemic strokes. They found that a point-of-care echo done by a skilled operator was 96% sensitive and 99% specific for finding a main source of embolism. Patients with LVO and pre-existing heart failure are more likely to have a source of embolism discovered. A large atrium was associated with having atrial fibrillation.
Take Home Points
1. A focused echo can be sensitive and specific for sources of embolism in ischemic stroke.
2. It is unclear if this practice could lead to improvements in meaningful patient centered outcomes.
Our score

Expert Reviewer for this Post

Joseph Pare, MD MHS @jrpare29
Dr. Pare is an attending physician at Boston Medical Center and Director of Ultrasound Research in the Department of Emergency Medicine at Boston University School of Medicine.
Cite this post as
Michael Prats. Ischemic Stroke – Focused Echo for Embolic Source. Ultrasound G.E.L. Podcast Blog. Published on November 23, 2020. Accessed on October 29, 2021. Available at https://www.ultrasoundgel.org/102.




