Originally published on Ultrasound G.E.L. on 8/20/18 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from Ultrasound G.E.L. team!
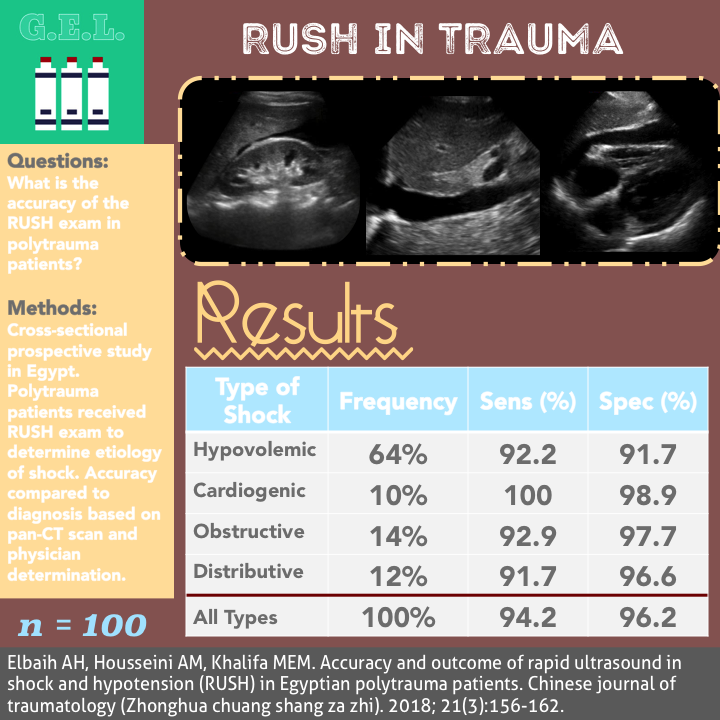
Accuracy and outcome of rapid ultrasound in shock and hypotension (RUSH) in Egyptian polytrauma patients
Chinese Journal of Traumatology – Pubmed Link
Take Home Points
1. This study does not prove that the RUSH exam is useful in polytrauma patients.
2. The RUSH exam may be able to accurately categorize the type of shock in polytrauma patients, but unclear how that can help management. This is not evidence to use ultrasound in place of other diagnostics.
Background
We know that focused ultrasound can be helpful in trauma. We also know that ultrasound can be helpful in critically ill and hypotensive patients. So….what about critically ill trauma patients?! That is the idea behind this article. Generally, patients with severe trauma go either to CT (computed tomography) to determine the extent of their injuries or straight to the operating room to repair their injuries. Ultrasound’s most useful role here is to identify an injury that would require the operating room in an unstable patient, thus allowing the patient to bypass CT. The question posed in this article is whether there is further role for ultrasound in identifying significant injuries, earlier in the course of management. The RUSH exam (Rapid Ultrasound in Shock and Hypotension) is one of several hypotensive protocols that examines various parts of the body in search of an etiology for shock. This paper applies this exam to the patient with significant trauma including multiple body systems (“polytrauma”). The authors’ goal seems to ultimately try to reduce the need for pan-CT of all of these patients.
Questions
What is the accuracy of the RUSH exam in polytrauma patients?
What are the outcomes in polytrauma patients who receive a RUSH exam?
Population
Single University Hospital in Egypt
Inclusion:
- Polytrauma patients (see below for definition)
- Patients receiving advanced trauma life support (ATLS) guidelines
- Treated for all life-threatening conditions
- Had 28 day follow up
- Consented to study (could be obtained from relative)
Exclusion:
- Shock from source other than trauma
Polytrauma patient =
A. Two major system injuries* + one major limb injury
B. One major system injury* + two major limb injuries
C. One major system injury* + one grade 3 open skeletal injury
D. Unstable pelvic fracture + visceral injury
*Major system injury = death within 24 hrs, injury severity score ≥16, ICU stay ≥1 day, or blood transfused ≥ 2 units
Design
Cross-sectional prospective study
All patients underwent primary survey by ATLS guidelines.
Life threatening conditions treated as they were encountered.
Then secondary survey and more in depth history, labs drawn.
Then RUSH protocol – heart, IVC, FAST, Aorta, Lung, DVT
Portable chest xray
Portable pelvis xray
For 28 days patients were followed to determine:
- Surgical interventions
- Admission to floor
- ICU admission
- Transfer to another center
- Discharge
- Death
Initial diagnosis was determined based on the notes by the emergency physicians or surgical attending. Additional diagnoses gathered from subsequent documentation. It seems that CT was the main standard but if subsequent diagnoses occurred, those could supercede the CT diagnosis.
In the abstract, it states that all patients received pan-CT (usually brain, cervical spine, chest, abdomen, pelvis, ± thoracic and lumbosacral spine. This was not mentioned in the methods, but the results and discussion seem to confirm this occurred.
Who did the ultrasounds?
The authors – from departments of Emergency Medicine, Radiology, and Anesthesia and Critical Care
The Scan
Curvilinear transducer (may also use Phased Array)

Cardiac views (originally parasternal long and apical four chamber – in this study they added parasternal short axis and subxiphoid as well)
IVC
FAST – RUQ, LUQ, Bladder views
Aorta
Bilateral anterior lungs
Then you can consider additional views for ectopic pregnancy (examining adnexa) and DVT (examining common femoral veins)
Here is how they determined the shock type in the present study:
Hypovolemic: hyperdynamic heart with low filling, flat IVC, peritoneal or pleural fluid, AAA or aortic dissection
Cardiogenic: hypodynamic heart, dilated heart, distended IVC, B-lines, pleural effusions, ascites, normal aorta
Obstructive: pericardial effusion, Right heart strain, hyperdynamic heart, distended IVC, absent lung sliding, +DVT
Distributive: hyperdynamic or hypodynamic heart, normal or small IVC, pleural or peritoneal fluid, normal aorta
**Note – unclear how they differentiated hypovolemic from distributive since there is a lot of overlap in the ultrasound findings.


The POCUS Atlas – Trauma Pathology
The POCUS Atlas – Echo Pathology
The POCUS Atlas – Pulmonary Pathology
The POCUS Atlas – Aorta Pathology
The POCUS Atlas – Evidence Atlas for Trauma
Results
The Patients
N = 100 patients
- 75% male
- Age range 7-65 (mean 27.5 yo) – 31% less than 18, 10% > 60 yo
- Most common mode of injury was RTA (road traffic accident) -86%. 8% GSW, 6% Falls
Types of Injuries
- Extremity injuries 34.2% (most common injury, remembering that each patient had multiple injuries)
- Head injuries – 32.4%
- Chest 16.4%
- Face 11%
- Abdominal/pelvis injuries – 3.7% (only 8 in entire cohort)
- Spine 2.4%
As far as how sick the patients were, that is unclear. Table 1 lists “Clinical predictors for hypovolemia”, but it is unclear what these data represent.
- Mean HR 107.6
- SBP 74, MAP 53.9
- GCS 13.1
- RR 28.4
Primary Outcome
The Accuracy of the RUSH Exam to diagnose the type of shock in unstable polytrauma patients
Overall accuracy 95.2%
Sensitivity 94.2%
Specificity 96.2%
Hypovolemic (64%)
Sensitivity 92.2%
Specificity 91.7%
Cardiogenic (10%)
Sensitivity 100%
Specificity 98.9%
Obstructive (14%)
Sensitivity 92.9%
Specificity 97.7%
Distributive (12%)
Sensitivity 91.7%
Specificity 96.6%
Types of Shock Based on RUSH exam
- 64% hypovolemic
- 14% obstructive
- 12% distributive
- 10% Cardiogenic
Note: Cardiogenic seems high for a trauma patients – assuming that cardiac tamponade was counted as obstructive, then this must mean a blunt cardiac injury leading to shock or shock from prior cardiac dysfunction.
Other Findings
28 day outcomes:
- 42% surgical intervention + ICU
- 23% Surgical intervention + floor
- 19% ICU without surgery
- 12% floor admission
- 4% transfer
43% mortality
53% discharge after complete recovery
4% transfer (with unknown outcome)
Limitations
Do you need an ultrasound to tell you that your polytrauma patient is in hypovolemic shock? Probably not. There were no AAAs, aortic dissections, PEs, or ectopic pregnancies picked up in this study so do we need to do the extra views of the RUSH beyond what we normally do in the EFAST exam? My take is no.
External validity – Egyptian population, different trauma management, different injuries. The distribution of types of shock would likely change in different population.
Mostly head and extremity injuries. However, there was still high mortality rate (43%) and high percentage of surgical intervention (65%). Unclear what counted as a surgical intervention. They mention that traumatic brain injury was most common cause for surgery. Therefore, ultrasound, although it could have ruled out other concurrent injuries, probably did not help with diagnoses in many of these patients.
Poorly explained methods. Really unclear how they made the comparisons. Did they make a diagnosis with ultrasound, then categorize, then compare to the category of shock based on injuries seen on the CT? Was there any blinding? – we don’t even know exactly who was performing the ultrasound and how well trained they were.
Limited sample size so not many patients in each category.
No patient centered outcomes. Would have been great to have a control group to compare the patient outcomes. If not a control group – would have been nice to assess if ultrasound changed decision making by leading to further testing or treatments.
Discussion
Does this matter? Are you not going to CT the patient? Determining which category of shock is not the same as identifying an injury. There are likely few cases where ultrasound alone would suffice.
On the other hand, however they may have derived them, the accuracies of the study were impressive. Is there some small population of trauma patient’s where this might be helpful? Perhaps the fake trauma that is secretly just an old person in shock who incidentally fell out of bed? Maybe, but I’m not even sure it is appropriate there.
These authors recommend, among other things, that the RUSH exam be used in polytrauma patients. I disagree. I would summarize the study more accurately with a quote from the article:
“Little studie[s] have been done for the accuracy of RUSH in polytrauma, so this study is kind of innovative.” Innovative indeed; however, innovation does not always translate into utility.
Take Home Points
1. This study does not prove that the RUSH exam is useful in polytrauma patients.
2. The RUSH exam may be able to accurately categorize the type of shock in polytrauma patients, but unclear how that can help management. This is not evidence to use ultrasound in place of other diagnostics.
Our score

Cite this post as
Michael Prats, MD. The RUSH Exam in Polytrauma. Ultrasound G.E.L. Podcast Blog. Published on August 20, 2018. Accessed on November 13, 2020. Available at https://www.ultrasoundgel.org/51.




