Ultrasound for Pediatric Skull Fractures
By Stephen Alerhand, MD
EM Resident Physician
Icahn School of Medicine at Mount Sinai
Edited by Alex Koyfman, MD
Case History
5 y/o boy BIBEMS s/p MVC. Per EMS report, the T-bone collision occurred at 30 mph, patient sitting in behind passenger seat wearing seatbelt. Airbags not deployed, no LOC, ambulated at scene. Entire left side of vehicle found jutted inwards.
Exam
GEN: Alert, crying, responding to basic questions intermittently, visibly shaken
HEAD: 2×2 cm round, L-sided parietal-occipital hematoma; minimal bleeding/drainage, moderate ttp
NEURO: No focal deficits, though somewhat limited 2/2 currently distressed state

You have mild-to-moderate concern for a skull fracture, but are hesitant to expose the child to the ionizing radiation of a CT scan, not to mention the likely necessary sedation. The PECARN Pediatric Head Injury algorithm for CT use is questionably positive for “signs of altered mental status” (agitation, slow response to verbal communication.).
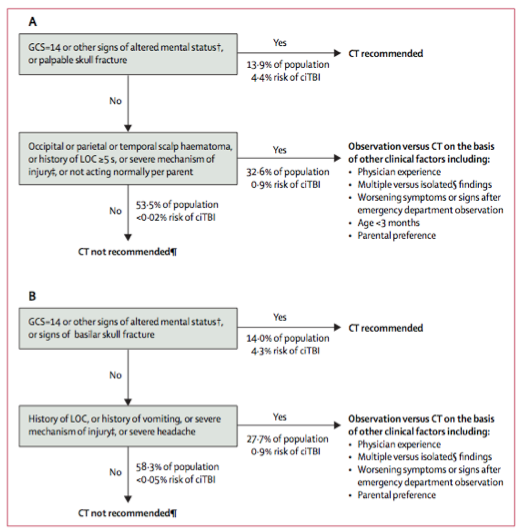
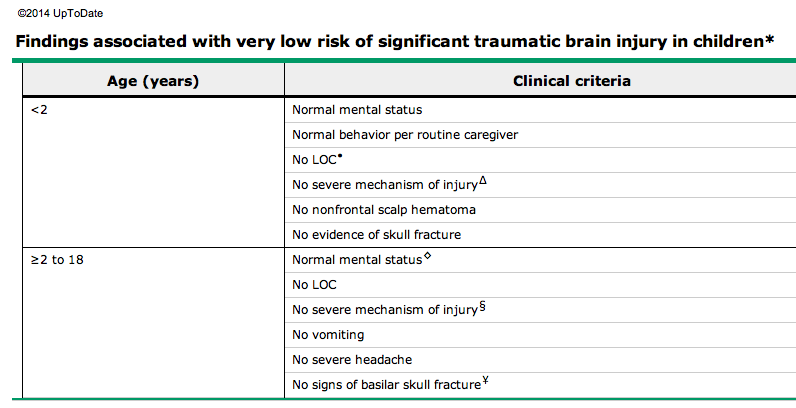
Kuppermann N, et al; Pediatric Emergency Care Applied Research Network (PECARN). Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009 Oct 3;374(9696):1160-70. Epub 2009 Sep 14. PubMed PMID: 19758692.
You are discussing the possible skull fracture with your team when the friendly neighboring ultrasound guru strolls right up and raises one piece of paper in each hand.
Piece of Paper #1
Rabiner, Joni E. et al. Accuracy of point-of-care ultrasound for diagnosis of skull fractures in children. Pediatrics 2013;131;e1757.
Type of Study:
— Prospective, n=69
Methods:
— Patients less than or equal to 21 y/o presenting with head injuries or suspected skull fractures that required head CT
— 1-hour focused ultrasound training session for clinicians
— CT scan as reference standard
Results:
— 8 of 69 with fracture (21%)
— Sensitivity 88% (53-98% CI)
— Specificity 97% (89-99% CI)
— Positive likelihood ratio 27 (7-107 CI)
— Negative likelihood ratio 0.13 (0.02-0.81 CI)
Conclusions:
— Focused US training session led to high specificity of diagnosis.
— Clinical assessment shown not to be entirely reliable.
Piece of Paper #2
Parry, Niccolo. et al. Ability of emergency ultrasonography to detect pediatric skull fractures: a prospective, observational study. Journal of Emergency Medicine 2013; 135-141.
Type of Study:
— Prospective, n=58
Methods:
— Patients less than 18 y/o with minor head trauma (normal mental status and neuro exam; no hemotympanum, Battle’s sign, or palpable bone depression)
— CT as reference standard
Results:
— Sensitivity 100% (82.2-100% CI)
— Specificity 95% (75.0-99.9% CI)
— Positive predictive value 97.2% (84.6-99.9% CI)
— Negative predictive value 100% (80.2-100% CI)
Conclusions:
— US provided accurate diagnosis.
— Consider incorporating into minor head injury prediction rules.
ED Pearls
- Advantages of US:
— Rapid, accurate, specific, lower cost, easy to learn; can “show” and thus reassure parents - Disadvantages of CT:
— Radiation exposure, sedation risk, higher cost, transport away from ED physicians/nurses - Skull fracture more predictive than scalp swelling or vomiting for traumatic brain injury.1-4 Increases likelihood by 4-fold to 20-fold.4-6
- Intracranial injury may still occur w/o skull fracture. Use caution in using US to rule this out.
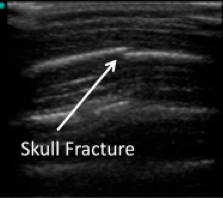
Performing the US 7
- Use linear probe.
- Scan the location of pain or hematoma in two planes.
- Visualize hyperechoic bone cortex beneath hypoechoic soft tissue and periosteum.
- Suture appears symmetric and regular, and leads to a fontanelle. Follow it there. Conversely, a fracture is jagged and may be displaced.
- That’s it. Pretty simple to learn.

Additional References
- Kuppermann N, Holmes JF, Dayan PS, et al. Pediatric Emergency Care Applied Research Network (PECARN) identification of children at very low risk of clinically important brain injuries after head trauma: a prospective cohort study. Lancet 2009;374:1160–70.
- Osmond MH, Klassen TP, Wells GA, et al., Pediatric Emergency Research Canada (PERC) Head Injury Study Group. CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury. CMAJ 2010;182:341–8.
- Schutzman SA, Barnes P, Duhaime AC, et al. Evaluation and management of children younger than two years old with apparently mi- nor head trauma: proposed guidelines. Pediatrics 2001;107:983–93.
- Schutzman SA, Greenes DS. Pediatric minor head trauma. Ann Emerg Med 2001;37:65–74.
- Quayle KS, Jaffe DM, Kuppermann N, et al. Diagnostic testing for acute head injury in children: when are head computed tomography and skull radiographs indicated? Pediatrics 1997;99:E11.
- Dunning J, Batchelor J, Stratford-Smith P, et al. A meta-analysis of variables that predict significant intracranial injury in minor head trauma. Arch Dis Child 2004;89:653–9.
- Dawson, Matt. Mallin, Mike. Introduction to Bedside Ultrasound: Volumes 1 and 2, 1st




