
Authors: Bryan Anderson1; Anthony Scoccimarro MD2; Muhammad Waseem, MD, MS1,2 (St. George’s University Grenada West Indies1, Lincoln Medical & Mental Health Center Bronx New York2) // Edited by: Jamie Santistevan, MD (@Jamie_Rae_EMdoc), Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital), and Brit Long, MD (@long_brit, SAUSHEC, USAF)
Skin and soft tissue infections encompass a wide array of clinical presentations and are common presenting conditions in the Emergency Department. In this post we will review the current treatment considerations of skin abscesses.
What is an abscess?
An abscess is a localized infection characterized by a collection of pus surrounded by inflamed tissue. Abscesses are fluctuant, tender and erythematous. Most cutaneous abscesses are appropriate for incision and drainage when they are larger than 5 mm in diameter and are in an accessible location [1].
Incision and drainage involves providing appropriate anesthesia followed by making a skin incision with a No. 11 or 15 surgical blade into the most prominent or fluctuant portion of the abscess. Ideally, the direction of the incision should be in line with the natural skin crease, along the natural lines of collagen of the dermis (Langer’s lines) [2]. Percutaneous drainage is defined as the placement of a catheter using imaging guidance, to provide continuous drainage of a fluid collection.
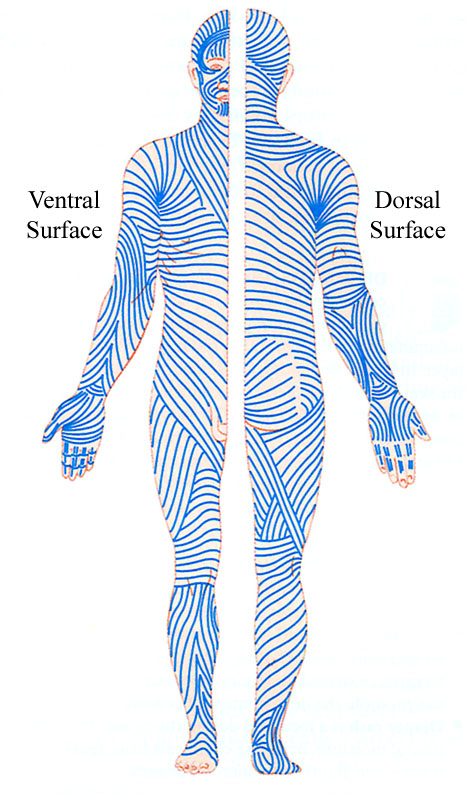
Figure 1: Langer’s lines of the skin
However, premature incision, before the localization of pus, may not be curative. Theoretically it may result in extension of the infectious process and may result in bacteremia [2].
Which abscesses require surgical consultation?
Often, an abscess is simple and can be drained in the emergency department. Occasionally, abscesses are complicated and require surgical consultation. In some cases, complicated abscesses may be better drained in the operating room. If an abscess meets the following criteria, surgical consultation should be obtained [1, 6]:
- Difficult to provide adequate anesthesia due to lack of patient cooperation, location or extent of abscess.
- Difficult or limited access, for example on the neck or perineum.
- Large, extensive, and complex abscesses, both size and depth, especially if deeper tissues are involved, such as bone (osteomyelitis) or muscles.
- Risk of neurovascular damage such as adjacent to major blood vessels and nerves.
- Anal, perirectal abscess, and pilonidal abscess due to risk for development of fistulas.
- Anatomically complex regions such as the hand.
- Cosmetic concerns, due to scarring, such as on the face, breast, and nasolabial folds.
- Vulvovaginal abscess or Bartholin gland cyst with abscess
- Multiple abscesses
- Abscess following recent surgery
What is the utility of obtaining labs?
In general, the utility of obtaining basic labs and blood cultures for patients presenting with uncomplicated soft tissue abscesses is of little clinical benefit. Most physicians agree that blood cultures in particular are not necessary because of the extremely low likelihood of a true positive result and the potential cost of a false positive is high including the need for repeated blood culture, unnecessary intravenous antibiotics, and the return to the ED for re-evaluation [3].
However for patients with symptoms and signs of systemic toxicity, such as fever, tachycardia and hypotension, laboratory studies may be helpful for determining if the patient is suffering from severe sepsis. Laboratory studies may include CBC, BMP, lactate and inflammatory markers [3].
Following incision and drainage of simple abscesses culture and susceptibility testing of the purulent material should be considered [1]. Culture results may guide antimicrobial therapy especially for patients with recurrent skin infections.
What is the utility of packing and irrigation?
For simple uncomplicated abscess requiring I & D, there is no benefit to packing or irrigation. No difference in recurrence rates or the need for further intervention has been demonstrated with packing [4, 5]. Abscesses with packing have higher pain scores and increased need for analgesia [6]. Despite this evidence, the majority of ED physicians surveyed report routinely using packing [7]. Packing may be useful for achieving hemostasis following drainage of a large and/or complicated abscess, and to facilitate the healing of deeper tissues before skin closure.
What are the indications for antibiotics?
In healthy patients with simple abscesses without surrounding cellulitis who undergo successful I & D, antibiotics are generally not indicated [1]. Systemic antibiotics do not significantly improve complete resolution of abscesses [8] although the practice of forgoing antibiotics for uncomplicated abscess recently has been called into question [9].
However, in the following circumstances antibiotics should be strongly considered [2]:
- Complex or multiple abscesses
- Systemic symptoms including fever, rigors, chills
- Extensive cellulitis
- Drug-resistant organisms including a history of MRSA or VRSA
- Immunocompromised state or other co-morbidities such as diabetes, HIV/AIDS, chronic steroid use, or actively receiving chemotherapy
- Extremes of age
- Failed response to I&D
- Incomplete drainage due to location
MRSA Considerations
Community Acquired- methicillin Resistant Staph. Aureus (CA-MRSA) has been reported to be responsible for many abscesses. Its prevalence in emergency department patients has been found to be as high as 56% in purulent skin and soft tissue infection [10]. Simple needle aspiration of abscesses is not adequate to treat abscesses caused by CA-MRSA [11].
What are some advanced and alternative techniques for abscess drainage?
Bedside ultrasound (US) is a useful adjunct in the evaluation of a potential abscess. Physical examination alone has been shown to have poor inter-rater agreement and has been found to be less sensitive and specific than US [12, 13]. Ultrasound has been shown to change management in half of all cases, both in eliminating the need for drainage and in identifying those in need of advanced diagnostics and/or consultation [11]. Therefore, bedside US is a non-invasive diagnostic test that may allow the avoidance of invasive therapeutic procedures. Additionally, US may distinguish abscess from cellulitis, identify a foreign body with an abscess and can delineate the extent and depth of an abscess.
Loop drainage is an improved skin abscess drainage procedure. For significantly large or continuously draining abscesses, bipolar small incisions are made at the abscess borders and a drain may be left in place as needed and for up to several days, to facilitate complete resolution [14]. This technique has significantly decreased the failure rate for appropriate treatment (1.4%, compared with 10.5% in the standard group) [14].

Figure 2: Loop drainage of axillary abscess
What are some considerations in the pediatric population?
Unlike most adults, young children may not be able to cooperate with the procedure without procedural sedation to ensure a successful and safe outcome. Compared to adults, pediatric patients are more likely to have a neck infection that necessitates surgical drainage [13]. Similar to adults, loop drainage has been found to eliminate the need for repetitive wound packing and simplified postoperative wound care and has been found to be safe and effective in children [14, 15, 16].
What are some other general considerations?
Beware of the Herpetic whitlow, a painful infection of the tip of the finger caused by herpes simplex virus. Herpetic whitlow may be difficult to differentiate from a paronychia, an infection at the edge of the fingernail, which can form into an abscess. It is important not to incise herpetic whitlow due to the risk of superinfection and delayed resolution.
It is also important to consider immune deficiency if a patient presenting with recurrent abscesses or with unusual organisms present.
References / Further Reading
[1] Fitch MT, Manthey DE, McGinnis HD, Nicks BA, Pariyadath M. Videos in clinical medicine. Abscess incision and drainage. N Engl J Med. 2007 Nov 8;357(19):e20
[2] Holtzman L, Hitti E, Harrow J. Incision and Drainage. 2014 Roberts and Hedges’ Clinical Procedures in Emergency Medicine, Chapter 37, 719-757.e3 Saunders Philadelphia
[3] Sauer MW, Hirsh DA, Simon HK, Kharazmi SA, Sturm JJ. Pediatric abscess characteristics associated with hospital admission from the ED. Am J Emerg Med. 2011 Nov;29(9):1013-1018
[4] Kessler DO, Krantz A, Mojica M. Randomized trial comparing wound packing to no wound packing following incision and drainage of superficial skin abscesses in the pediatric emergency department. Pediatr Emerg Care. 2012 Jun;28(6):514-517
[5] Leinwand M, Downing M, Slater D, Beck M, Burton K, Moyer D. Incision and drainage of subcutaneous abscesses without the use of packing. J Pediatr Surg. 2013 Sep;48(9):1962-1965
[6] O’Malley GF, Dominici P, Giraldo P, Aguilera E, Verma M, Lares C, Burger P, Williams E Routine packing of simple cutaneous abscesses is painful and probably unnecessary. Acad Emerg Med. 2009 May;16(5):470-473
[7] Schmitz G, Goodwin T, Singer A, Kessler CS, Bruner D, Larrabee H, May L, Luber SD, Williams J, Bhat R. The treatment of cutaneous abscesses: comparison of emergency medicine providers’ practice patterns. West J Emerg Med. 2013 Feb;14(1):23-28
[8] Singer AJ, Thode HC. Systemic Antibiotics After Incision and Drainage of Simple Abscesses. A Meta-analysis. Emerg Med J. 2014;31(7):576-578
[9] Talan DA, Mower WR, Krishnadasan A, Abrahamian FM, Lovecchio F, Karras DJ, Steele MT, Rothman RE, Hoagland R,Moran GJ. Trimethoprim-Sulfamethoxazole versus placebo for uncomplicated skin abscess. N Engl J Med.. 2016 Mar 3;374(9):823-832
[10] Moran G J, Krishnadasan A, and Gorwitz R J et al.: Methicillin-resistant Staphylococcus aureus infections among patients in the emergency department. N Engl J Med. 2006; 355: 666–674
[11] Gaspari RJ, Resop D, Mendoza M, Kang T, Blehar D: A randomized controlled trial of incision and drainage versus ultrasonographically guided needle aspiration for skin abscesses and the effect of methicillin-resistant Staphylococcus aureus. Ann Emerg Med 2011; 57: 483-491
[12] Tayal VS, Hasan N, Norton HJ, Tomaszewski CA. The effect of soft-tissue ultrasound on the management of cellulitis in the emergency department. Acad Emerg Med. 2006 Apr;13(4):384-388
[13] Ramirez-Schrempp D, Dorfman DH, Baker WE, Liteplo AS. Ultrasound soft-tissue applications in the pediatric emergency department: to drain or not to drain? Pediatr Emerg Care. 2009 Jan;25(1):44-48
[14] Wendling, Patrice. ACEP News: Novel Technique Improved Skin Abscess Drainage. January 2009. Elsevier Global Medical News. Retrieved on March 31, 2016 from https://www.acep.org/Clinical—Practice-Management/Novel-Technique-Improved-Skin-Abscess-Drainage/?__taxonomyid=118007
[15] Tsoraides SS, Pearl RH, Stanfill AB, Wallace LJ, Vegunta RK. Incision and loop drainage: a minimally invasive technique for subcutaneous abscess management in children. J Pediatr Surg. 2010 Mar;45(3) 606-609
[16] Ladd AP, Levy MS, Quilty J. Minimally invasive technique in treatment of complex, subcutaneous abscesses in children. J Pediatr Surg. 2010 Jul;45(7):1562-1566
[17] Skin and the Integumentary System. Jan 7, 2007. Retrieved on May 31, 2016 from: http://www.freethought-forum.com/forum/showthread.php?t=11578&garpg=2
[18] Roberts, JR, Roberts, M. Emergency Medicine News. Pilonidal Abscess: The Very Bare (Back) Basics.. Feb 3, 2015. Retrieved on May 31, 2016 from: http://mobile.journals.lww.com/em-news/_layouts/15/oaks.journals.mobile/post.aspx?blogId=8&postId=25





2 thoughts on “Update on the management of skin abscesses in the emergency department”
Pingback: CanadiEM Frontline Primer - MSK - Extremity Soft Tissue Abnormalities - CanadiEM
Pingback: CanadiEM Frontline Primer - Skin and Soft Tissue Infections - CanadiEM