Authors: Eriny Hanna, MD (@Eriny-Hanna-3, EM Resident Physician, Vanderbilt University Medical Center) and Aaron Lacy, MD (@AaronLacyMD, EM Attending Physician, Vanderbilt University Medical Center) // Reviewed by: Michael J. Yoo, MD (EM Attending Physician, San Antonio, TX), Alex Koyfman, MD (@EMHighAK), and Brit Long, MD (@long_brit)
Case
A 73-year-old female with a history of recurrent urinary tract infections (UTI), kidney stones, and type 2 diabetes mellitus presents with flank pain. The pain is left-sided, has been progressively worsening for 3 days, and now is constant. Her flank pain was associated with hematuria on the first day and now with urinary urgency. She denies dysuria, fevers, or chills. She has had multiple episodes of emesis and ongoing nausea. Her initial vitals are: T 36.7°C, HR 100, BP 146/72, RR 16, SpO2 98% on room air. On exam, she has left-sided costovertebral angle (CVA) tenderness. The patient’s urine is positive for leukocyte esterase and nitrites on dipstick. Urinalysis microscopy demonstrates 591 WBCs, 223 RBCs, and 2+ bacteria. Her creatinine is 1.05, close to her recent baseline values. Computed tomography (CT) of the abdomen/pelvis without contrast was obtained which demonstrated a left 4 mm stone at the ureteropelvic junction (UPJ) without hydronephrosis.
How do you determine if the patient needs hospitalization or can be discharged? When do you consult urology versus arrange follow-up? What treatments should you initiate?
Background
Urolithiasis is a common cause of emergency department (ED) visits worldwide, accounting for up to 9% of all visits, increased from 3% in the 1980s.1 There are approximately 1 million visits a year, resulting in a heavy economic burden.2 Similarly, the incidence of complications, including infection and obstruction, are increasing, necessitating prompt recognition and management of this disease process.3
Kidney stones become symptomatic as they travel down the ureter.4 Subsequently, ureterolithiasis is a more accurate term than nephrolithiasis, though often used interchangeably. Urolithiasis is a general term for all stones found anywhere along the urinary system. Pain in urolithiasis is secondary to ureteral muscle contraction and prostaglandin release.5 The pain is classically described as colicky, waxing and waning, and associated with dysuria and urinary urgency as the stone travels distally. Pain may become more constant if obstruction is present.5
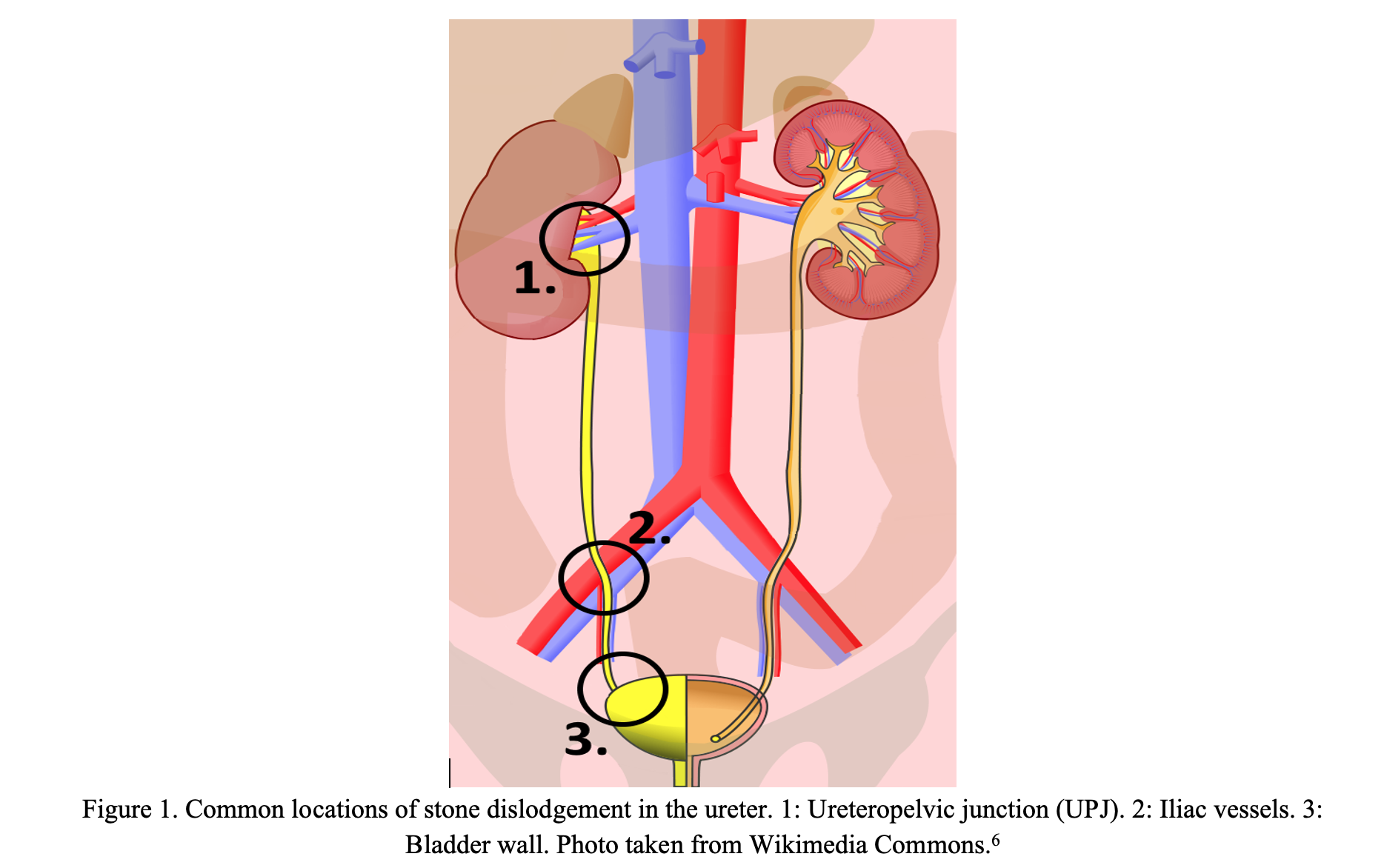
Stones typically get stuck at 3 common locations: the ureteropelvic junction (UPJ), the iliac vessels, and the bladder wall (Figure 1).4
The pain can be located anywhere between the flank and the groin depending on location, migration of the stone, and referred pain. Nausea and vomiting are secondary to vagal nerve and splanchnic nerve stimulation.4,5 Hematuria is another common symptom due to damage of the ureteral wall. Hematuria has the highest sensitivity, between 83% and 95%, within the first 24 hours of onset.7 However, its absence is not a reliable exclusion criterion.7,8
The ED visit should be focused on two things in patients with suspected renal colic: assessing for complicated urolithiasis and evaluating for other serious, life-threatening diagnoses. Figure 2 highlights stone-related emergencies as well as alternative diagnoses to consider.9 Further information on the differential diagnosis of renal colic can be found here and thoughts on diagnostic mistakes by ED legend, Dr. Peter Rosen, here.10,11

Evaluation
The presence of complications, size of stone, location, and patient risk factors guide management of urolithiasis, as discussed below.
1. Evaluating for Infection
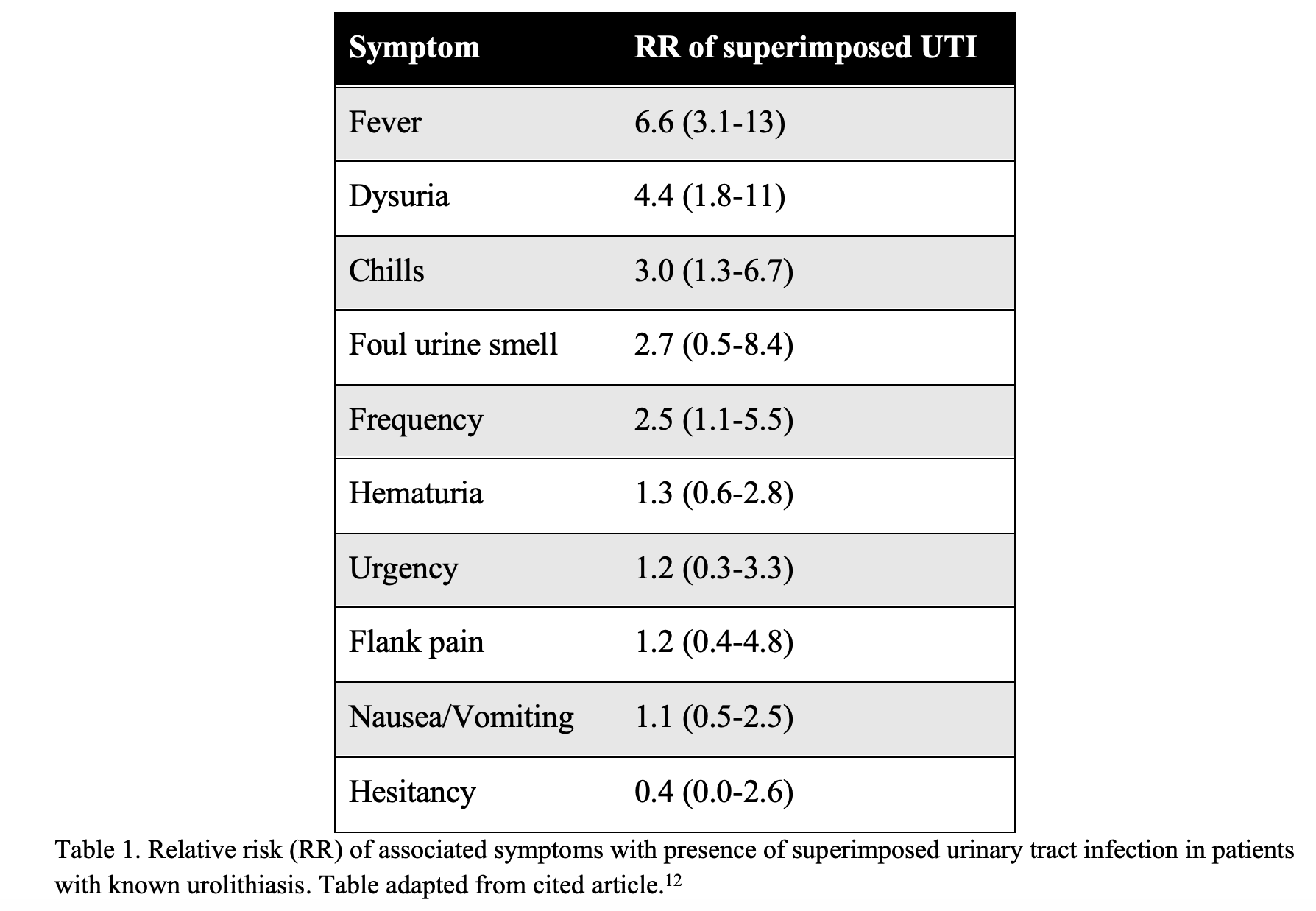
Obtain a urinalysis (UA) with microscopy and urine culture on every patient with suspected ureteral stones. This includes patients with low clinical concern for a concomitant infection. Specifically, several studies determined that up to 10% of patients with urolithiasis will have positive urine cultures.12,13 One study showed that 37% of patients who were found to have untreated positive urine cultures in urolithiasis developed systemic inflammatory response syndrome (SIRS), and 5% progressed to septic shock.14 Pyuria, female sex, dysuria, urinary frequency, chills, and fever were the greatest predictors of superimposed UTI (Table 1).12 Of note, in this study, 26 of 28 (93%) of study patients who had UTI were female.12
In patients with known urolithiasis, a UA with >5 WBCs was 86% sensitive and 79% specific for an associated infection.12 Furthermore, UA with >20 WBC was 57% sensitive and 93% specific for infected stone.12 This study is described in more detail here.15 Presence of bacteria, nitrites, and leukocyte esterase are also predictive.12,13 While ureteral inflammation itself can cause pyuria, the degree of pyuria is significantly associated with an increased chance of a positive urine culture, with >50 WBC associated with a 60% risk of positive culture and large volume leukocyte esterase having a 78% risk.13 An additional study determined infectious UA, CRP (≥1.5) and patient age (≥ 54 years) were significant UTI predictors, but neither serum WBCs nor typical UTI symptoms were associated with superimposed UTI.16 Subsequently, obtaining a UA and culture are essential in ruling out infection.
A urinalysis and culture must be obtained on every patient in which ureteral stone is suspected or confirmed.
2. Interpreting Elevated Creatinine
Obtain a basic metabolic panel on every patient with suspected urolithiasis. Although of uncertain clinical significance, stone formers have a lower creatinine clearance than the general population, even when adjusted for age, sex, and body weight.17 An increase in creatinine does not necessarily indicate an obstruction and should be compared with the patient’s baseline, if available. A pediatric/young adult study found that those with acute kidney injury (AKI) were more likely to have vomiting and dehydration, rather than actual obstruction or infection, and fluid resuscitation should be considered.18Another cause of loss of kidney function is intra-renal crystal nephropathy changes and damage secondary to stone formation.19
The diagnosis of ureteral obstruction cannot be made with labs alone, but an elevated creatinine compared to baseline should raise suspicion for urolithiasis in patients with renal colic.
3. Imaging – Obstruction, Size, and Location
The main goal of imaging should be to determine if obstruction is present. Determining stone size is also beneficial depending on the patient’s risk factors for complications. Patients at particularly high risk include those with fever, hemodynamic abnormalities, solitary kidney, transplant kidney, and those with prior urologic procedures.20 Kidney, ureter, and bladder (KUB) X-rays have limited utility in diagnosing renal stones, as they do not provide information regarding the presence of hydronephrosis; furthermore, the sensitivity (53%) and specificity (79%) of KUBs are lower than other modalities.20 A non-contrast CT of the abdomen and pelvis is the gold standard for diagnosis of ureterolithiasis due to its high sensitivity (98%) and specificity (100%) for diagnosis of stones, ability to identify the presence and degree of obstruction, and pre-operative planning with urology if necessary.20 Low dose and ultra-low dose CT are comparable to standard dose in terms of sensitivity and specificity for renal stones but do not as accurately detect <3mm stones or stones in patients with BMI >30.21,22 Ultra-low dose CT has radiation dosing close to a KUB X-ray.20 Ultra-low dose CT sensitivity and specificity are better than X-ray, but may not be as good as higher-dose CT in detecting other abdominal pathologies.23,24 If considering other intra-abdominal pathologies, regular dose CT scan should be ordered (Figure 2).
Detection of stones in CT with contrast has been long debated, but the data supports that CT with contrast has the same negative predictive value for obstructive ureterolithiasis than CT without contrast.25 Obstructive urolithiasis can safely be ruled out with a contrasted study.25 There are additional benefits of contrast for ureterolithiasis, such as demonstrating secondary signs of obstruction, determining level of obstruction, and identifying pelvic phleboliths. Also, the stone itself can be detected with similar sensitivity on contrasted CT.26
CT scans with contrast have the same negative predictive value for obstructive stones than a CT without contrast and can be used to identify other intra-abdominal pathologies or signs of stone complication.
Per the American College of Emergency Physicians (ACEP) ‘Choosing Wisely’ guidelines, CT should be avoided in healthy, young patients (<50-years-old) with known history of kidney or ureteral stones presenting with classic, uncomplicated renal colic.27 A CT in this case usually does not change treatment decisions. Renal point of care ultrasound (POCUS) may be useful in this case to rule out obstruction. However, obtain a CT if you are considering other intra-abdominal etiologies of renal colic or a complicated stone.
A 2014 multi-center study determined that an initial POCUS, rather than CT, leads to less radiation exposure without any significant difference in high-risk diagnoses, serious adverse events, pain, or ED repeat visits at 30 days.28,29 The goal of POCUS is to determine the presence and grade of hydronephrosis to guide management, as presence of hydronephrosis suggests a large (>5mm) stone. 30,31 For children and pregnant patients, POCUS should be the first-line imaging modality. MRI is the follow-up option in pregnant patients with an equivocal ultrasound, and low dose CT or KUB is second line in children.32
POCUS should be the first line imaging modality in children, pregnant patients, and healthy, young (<50) patients presenting with classic signs of renal colic. Otherwise, CT is the imaging modality of choice in the diagnosis of ureterolithiasis. CT scans or other imaging modalities as the clinical situation dictates should be performed in all other cases.
4. Prediction Tools
Several prediction tools have been created to determine higher likelihood of urolithiasis and lower likelihood of serious alternative diagnoses. The most common one is the STONE score, which determined that male sex, short duration of pain (<24 hours), nausea and vomiting, microscopic hematuria, and non-black race were top predictors of ureteral stone in patients presenting with flank pain.33 Patients are stratified into low, intermediate, and high risk. Combining STONE with evaluation of hydronephrosis by ultrasound increased the likelihood of urolithiasis as the diagnosis.34 Subsequent studies showed the STONE score still performs similarly without inclusion of race as a variable and has been widely validated.34-38
A newer predictive tool, CHOKAI, originally created in Japan, uses 7 factors: age <60 years, male sex, duration of pain of <6 hours, nausea/vomiting, hydronephrosis (on ultrasound), hematuria, and history of ureteral stones. 39 Though additional external validation is needed, the CHOKAI score appears promising and diagnostically superior to the STONE score, especially in international sites.40,41
A newer predictive tool called CLAD aims to rule out patients who are at risk of alternative diagnoses or need early urologic intervention (within 7 days).42 The investigators determined high risk factors were: age >45 years, history of urologic surgery, pulse >100 bpm, temperature >37.8 °C, and urine dipstick negative for blood.42 This tool isn’t validated yet and should be used with caution. Just remember to think critically about disposition in patients who meet any of the CLAD criteria.
STONE, CHOKAI, and CLAD are predictive tools that can be used to help with work-up in ureteral stone workups. However, no predictive tool or scoring system should replace clinical judgement.
Treatment and Disposition
There are key guidelines from national and international urology associations on the management of urolithiasis based on a wide appraisal of the literature. The European Association of Urology (EAU) published guidelines in 2021, while the latest American Urological Association (AUA) recommendations are from 2016.32,43 Each society scored the level of evidence differently but still largely came to the same conclusions regarding management.
There are two hard indications for urgent urological intervention: infection and obstruction with known or impending kidney injury. Once either is suspected, start broad-spectrum antibiotics, and obtain CT imaging emergently to guide operative planning. Which antibiotics to use should be based on the local antibiogram, resistance patterns, and patient risk factors for resistance. Gram negative bacteria are more common, with E. coli being the most common, but gram-positive bacteria are also possible, mainly Enterococcus.44 Only a small percentage are related to fungal pathogens, mainly Candida.44 One study found that 25% of urine cultures distal to obstruction were different from the cultures obtained intraoperatively after drainage, so broad spectrum coverage should be highly considered, even if past culture data is known.44 The IDSA does recognize the importance of periprocedural antibiotics in infected urolithiasis but does not have firm guidelines on recommending a specific regimen.45 There is increasing antibacterial resistance in patients with infected urolithiasis, particularly at academic medical centers.44 Given this concern, certain urological groups suggest cefepime as a plausible first line, especially in patients at risk of developing sepsis secondary to UTI, with aztreonam being an alternative if there is an allergy.44 A reasonable start in patients without high risk factors for bacterial resistance patterns would be a third-generation cephalosporin, such as ceftriaxone. 44 Amikacin or gentamicin can be added if signs of sepsis are present, and polymyxin should be considered for patients who are high risk for resistance, such as those presenting from nursing homes, have indwelling catheters, have history of resistance, recurrent UTIs, or recent antibiotics.44 If all else fails, carbapenems are the ‘big guns’ that have the lowest amount of resistance.44 Penicillin, amoxicillin/clavulanate, lower generation cephalosporins, TMP/SMX, and fluoroquinolones have relatively high rates of resistance in infected stones and should generally be avoided. 46,47 This emDOCs review provides some suggested dosing of antibiotics.48 Just keep in mind resistance patterns and patient risk factors when deciding on an antibiotic regimen.
Either ureteral stenting by urology or a percutaneous nephrostomy (PCN) tube, usually by interventional radiology (IR), is required for emergent drainage of urine in patients with infected urolithiasis.49 There are minimal differences in outcomes between these two methods.49 Stone removal prior to antibiotic therapy increases chances of progressing to bacteremia. PCN may be a better option for patients who are hemodynamically unstable since stenting usually requires general anesthesia.43 There is a two-fold increase in mortality when there is delayed decompression in septic patients, so the preferred treatment modality should be whichever is most readily available.43 Of note, struvite stones are mainly caused by underlying infection, usually Klebsiella or Proteus, and their definitive management is removal.43 Predictors of mortality include the presence of AKI upon presentation, vital sign abnormalities such as hypothermia and tachycardia, altered mental status, and need for intubation.50 These patients require ICU admission after urologic intervention.50
One cross-sectional study determined that female sex, age >60, multiple stone sites, presence of obstruction, and staghorn/struvite calculi were risk factors for superimposed infection.51 Females are twice as likely to develop infected urolithiasis than males.3 If UA or clinical presentation is equivocal in these populations, err on the side of caution in management.
When a patient with urolithiasis has either an obstructed or infected stone, urgent intervention is indicated. Percutaneous nephrostomy by an interventional radiologist or urethral stenting by a urologist have similar outcomes, and whichever can be done quicker should be the intervention of choice.
Your patient does not have infection or obstruction: Now what?
1. Stone Size and Location
Management of uncomplicated stones is usually less pressing. The AUA recommends observation if a stone is <10mm.43 The EAU recommends observation if the stone is 6mm.32 If the stone is distal (lower border of sacrum to the bladder) and >5mm, then medical expulsion therapy (MET) is recommended by both associations.32,43 Short periods of observation are recommended (no more than 4-6 weeks).43,52 If there are risk factors for complications, recurrent stones, or if the stone is 6mm or greater, urology follow-up is recommended. 32
Unlike obstruction and infected stones, the guidelines on size and location are not as clear-cut. Both urologic societies stress shared decision making with the patient and statistics may help with this dialogue. Certain stone characteristics on CT are associated with likelihood of spontaneous passage.52 Stones <5mm have greater than 75% chance of passing spontaneously, stones between 5mm and 10mm, 50%, and >10mm less than 25%.52 A distal stone (past sacroiliac joint) has >75% chance of passage while a proximal stone (above sacroiliac joint) 50% with midureteral falling between those.52 Another recent, smaller prospective study showed similar results.53 Stones ≥6.5mm had a 29% (2/7) rate of spontaneous passage within 28 days but only 9% (2/23) by 20 weeks.53 Think about involving urology in the ED or having urgent follow-up when the chances of spontaneous passage are relatively low and when the patient re-presents with renal colic, especially if not passed within the first 30 days of symptoms.
Stone size and location on CT are critical components to the likelihood of spontaneous passage. Stones <5mm and distal are the most likely to pass spontaneously, while those proximal and >10 are the most likely to require intervention. Shared decision making based on stone size in combination with symptoms is recommended.
Asymptomatic stones in the kidney (as opposed to in the ureter) are often found incidentally. Unless causing obstruction, patients can be reassured as they rarely require surgical intervention.54 Risk factors to stones in the kidney becoming symptomatic include stones >5 mm, non-inferior pole stones, diabetes, or high serum uric acid; subsequently, patients should have non-urgent urology referral for long-term monitoring or early intervention if high risk.54 Active surveillance is recommended by AUA if asymptomatic, but surgical intervention can be offered if a patient is symptomatic and there is no other explanation for the pain.43
2. Medical Expulsive Therapy (MET)
There has been conflicting data on the efficacy of MET. Despite this the AUA and EAU recommend the use tamsulosin for distal stones between 5 and 10 mm to aid in stone expulsion.32,43
A meta-analysis performed by ED providers supports this recommendation, with a number needed to treat of five.55 Tamsulosin works by aiding ureteral smooth muscle relaxation. Adverse reactions to alpha receptor blocking medications such as tamsulosin include orthostatic hypotension and retrograde ejaculation. It’s typically dosed as 0.4mg daily until resolution of symptoms or up to 4 weeks. Tamsulosin can still be offered with smaller and more proximal stones, but there is likely no statistically significant benefit in these cases, and the decision for MET should be patient driven.56 There have been other alpha blockers studied, such as silodosin 8 mg once daily. Meta-analysis suggests that it may be superior to tamsulosin in terms of success rate for <10 mm distal stones.57 Agents such as calcium channel blockers and phosphodiesterase inhibitors have also been studied but are not nearly as effective as alpha receptor blockade and not recommended for MET.32
3. Pain Management in Symptomatic Urolithiasis
Pain management is one of the main pillars of managing urolithiasis in the ED. Time and again, non-steroidal anti-inflammatory drugs (NSAID) have proven to be the recommended mainstay of pain control.58,59 A meta-analysis determined that NSAIDs, opioids, and acetaminophen have the same rates of pain control at 30 minutes after administration; however, NSAIDs required less redosing and were associated with less vomiting than opioids.58 While in most conditions oral NSAIDS provide comparable pain relief to IV NSAIDS, in renal colic, IV ketorolac provides faster clinical relief than oral ibuprofen. 60 Recommendations are to start with 15mg of ketorolac IV or IM in the acute phase, with combination oral NSAIDs and short course of narcotics if indicated in the outpatient setting.32 However, the EAU warns that diclofenac and ibuprofen increase major adverse coronary events and should be used with caution in patients with specific risk factors, and NSAIDs should be avoided in patients with a glomerular filtration rate (GFR) <30.32 Patients should also be treated for dehydration with fluid bolus(es) and nausea/vomiting with ondansetron or metoclopramide.
The use of lidocaine as an adjunct in renal colic is discussed here and here.61,62 Multiple studies have demonstrated that IV lidocaine helped to reduce the use of opioids and is recommended for patients who have severe or refractory pain.63 The regimen suggested by ACEP is: cardiac lidocaine 1.5 mg/kg (maximum 200 mg) IV over 10 minutes in addition to ketorolac 15 mg IV, 1L 0.9% normal saline, and acetaminophen 1,000 mg PO or IV.64 Contraindications to using lidocaine include history of seizures, cardiac disease, pregnancy, and hepatic/renal failure.62,64
There has recently been interest in using ketamine as an adjunct for renal colic. A double-blind RCT in Iran compared morphine 0.1 mg/kg + ketamine 0.2 mg/kg versus morphine + saline placebo.65 The ketamine group had significantly lower pain ratings at 20 and 40 minutes, but the differences were only 0.5 on a 10-point pain scale.65 Fewer participants needed re-dosing of analgesia in the ketamine group [OR 0.43 (0.22–0.83)].65 There was less vomiting with ketamine, but the risk of dizziness was twice as high in the ketamine group.65 Other small studies have evaluated the efficacy of ketamine in the setting of urolithiasis but external validation is needed before becoming mainstream.
The latest approach in EM has been performing plane blocks for providers who are ultrasound trained. A study of 40 patients found significantly different lower pain scores using erector spinae plane blocks compared to NSAIDs and also reduced opioid use.66 Transversus abdominis plane block is also described as effective in case reports.67 It is yet to be determined if this will be widely adopted by ED providers. If pain cannot be well controlled in the ED or if vomiting is intractable, patients can be admitted to the hospital for further symptom management. If there is persistent intolerable pain, this alone may be an indication for urological intervention. 67
NSAIDs are the mainstay of pain management in the patient with symptomatic urolithiasis, but other adjuncts should be considered, especially in those with refractory pain.
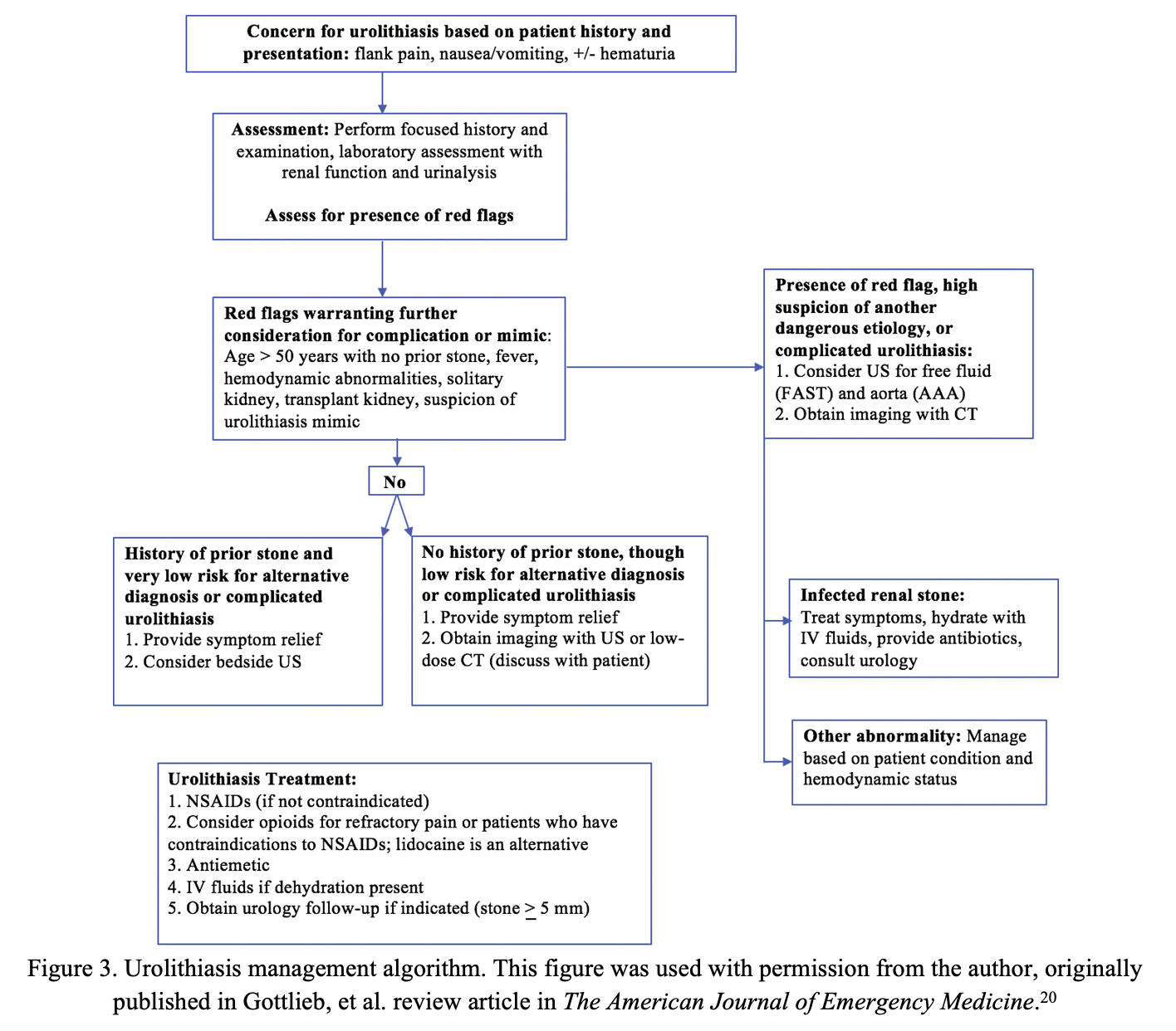
Figure 3 below offers a summary of urolithiasis management that we have discussed thus far.20 A bullet point summary is found here.68
Final Disposition Determination
About 20% of patients with urolithiasis are admitted.69 Patients with evidence of infection, AKI, hydronephrosis on ultrasound, history of prior urologic procedure, and need for opiates were more likely to get admitted, and approximately 75% of admitted patients underwent an in-hospital urologic procedure.69 Patients who were discharged and required urologic intervention within 90 days were those with larger stones, presenting after a longer period of symptoms, and had a history of prior procedures.69 Stone size (>5mm) was the strongest predictor of intervention.69
When considering discharge, reassess vitals and laboratory findings. Reassess the patient’s pain, and make sure the patient can urinate and is PO tolerant. Consider their risk factors and comorbidities and ensure follow up is established.
Prevention and Recurrence Counseling
The recurrence rate of stones is approximately 50% within 10 years.20 Patients should be counseled to intake water with a goal urine output of 2.5L per day.70 Those with calcium or cysteine stones would benefit from limiting sodium to no more than 2,300 mg per day and increasing calcium intake with a goal of 1-2 g, respectively.71 Limiting animal protein is more useful with those who have uric acid or cysteine related stones.71 In refractory cases, patients may benefit from oral therapies such as thiazide diuretics, potassium citrate, or allopurinol, but these pharmacologic therapies are made in conjunction with urology and the primary care physician.70,71
Case Resolution
Given a diagnosis of ureteral stone with infection, the patient was given 1L LR bolus, 15 mg of IV ketorolac, 4 mg of IV ondansetron, and 2 g of ceftriaxone. She was admitted to a medical service, and urology was consulted who proceeded with stent placement. The patient required PO opioids, acetaminophen, and IV ketorolac for pain while admitted. Her urine culture grew E. coli sensitive to cefdinir, and she was transitioned, to complete a 10-day treatment course. She had outpatient follow-up for definitive removal of the stone 2 weeks later. She follows regularly with urology for further medical management of her stones.
Pearls
- Do not forget to consider complications (infection, AKI, obstruction) as well as serious alternative diagnosesin every patient with flank pain.
- When needing to evaluate for other etiologies of flank pain, a contrasted CT has adequate sensitivity for obstructive stones. Otherwise, low dose and even ultra-low dose non-contrast CT will detect clinically significant (>3mm) stones. Do start with renal ultrasound first if there is low suspicion of complication or serious alternative
- Disposition bottom line:
- Infection or AKI due to obstruction: urgent urology consult for drainage + broad spectrum antibiotics + admission (floor vs ICU depending on hemodynamics).
- Moderate/severe hydronephrosis or >10mm stone: urology consult (or very urgent outpatient urology follow up if young, healthy, uncomplicated). Disposition can vary depending on urology’s plan for intervention.
- Intractable pain/vomiting/dehydration/revisit for worsening symptoms: admit to floor for symptom control.
- Presence of risk factors for developing complications/needing intervention: arrange a very urgent urology clinic follow up if discharging. Admit any patient with concerns for loss to follow up or clinical deterioration.
- Uncomplicated, small, distal stone: Discharge with pain control +/- MET, close PCP follow up and non-urgent urology clinic follow up.
References
- Raheem, O., Khandwala, Y, Sur, R., Ghani, K., & Denstedt, J. Burden of urolithiasis: Trends in prevalence, treatments, and costs. European Urology Focus. 2017. 3:18-26.
- Ghani, K., Roghmann, F., Sammon, J., Trudeau, V., Sukumar, S., Rahbar, H., & Trinh, Q. Emergency department visits in the United States for upper urinary tract stones: Trends in hospitalization and charges. The Journal of Urology. 2014. 191:90-96.
- Sammon, J., Ghani, K., Karakiewicz, P., Bhojani, N., Ravi, P., Sun, M., & Trinh, Q. Temporal trends, practice patterns, and treatment outcomes for infected upper urinary tract stones in the United States. European Urology. 2013. 64:85-92.
- Ingimarsson, J., Krambeck, A., & Pais, V. Diagnosis and management of nephrolithiasis. Surgical Clinics. 2016. 96:517-532.
- Shokeir, A. Renal colic: New concepts related to pathophysiology, diagnosis and treatment. Current Opinion in Urology. 12:263–9.
- Ureter stones. WikiMedia Commons. https://commons.wikimedia.org/wiki/Category:Ureter_stones#/media/File:Ureter_Engstellen.png
- Kobayashi, T., Nishizawa, K., Mitsumori, K., Ogura, K. Impact of date of onset on the absence of hematuria in patients with acute renal colic. Journal of Urology. 2003. 170:1093.
- Safriel, Y., Malhotra A., Sclafani, S., et al. Hematuria as an indicator for the presence or absence of urinary calculi. American Journal of Emergency Medicine. 2003. 21: 492–3.
- Wang, R. Managing urolithiasis. Annals of Emergency Medicine. 2016. 67:449-454.
- Crain, N. Renal colic: Differential diagnosis and approach to management. emDocs. 2017. http://www.emdocs.net/renal-colic-mimics-differential-diagnosis-approach-management.
- Rosen, P. EM decision making: Thoughts on mistakes in renal colic. emDocs. 2016. http://www.emdocs.net/em-decision-making-thoughts-on-mistakes-in-renal-colic.
- Abrahamian, F., Krishnadasan, A., Mower, W., Moran, G., & Talan, D. Association of pyuria and clinical characteristics with the presence of urinary tract infection among patients with acute nephrolithiasis. Annals of Emergency Medicine. 2013. 62:526-533.
- Dorfman, M., Chan, S., Hayek, K., & Hill, C. Pyuria and urine cultures in patients with acute renal colic. The Journal of Emergency Medicine. 2016. 51:358-364.
- Mariappan, P., Smith, G., Bariol, S., Moussa, S., & Tolley, M. Stone and pelvis urine culture and sensitivity are better than bladder urine as predictors of urosepsis following percutaneous nephrolithotomy: a prospective clinical study.Journal of Urology. 2005. 173: 1610-1614.
- Schmitz, G, & Hockstein, M. emDocs Cases: The sick kidney stone patient. emDocs. 2018. http://www.emdocs.net/emdocs-cases-the-sick-kidney-stone-patient.
- Rosenhammer, B., Spachmann, P., Burger, M., Fritsche, H., & Schnabel, M. Prospective evaluation of predictive parameters for urinary tract infection in patients with acute renal colic. The Journal of Emergency Medicine. 2018. 55:319-326.
- Worcester, E., Parks, J., Evan, A., & Coe, F. Renal function in patients with nephrolithiasis. The Journal of Urology. 2006. 176:600-603.
- Farris, N., Raina, R., Brown, M., Colvis, M., Schwaderer, A. L., & Kusumi, K. Acute kidney injury associated with urinary stone disease in children and young adults presenting to a pediatric emergency department. Frontiers in Pediatrics. 2020. 8:784.
- Keddis, M., & Rule, A. Nephrolithiasis and loss of kidney function. Current Opinion in Nephrology and Hypertension. 2013. 22:390.
- Gottlieb, M., Long, B., & Koyfman, A. The evaluation and management of urolithiasis in the ED: A review of the literature. The American Journal of Emergency Medicine. 2018. 36:699-706.
- Rob, S., Bryant, T., Wilson, I., & Somani, B. K. Ultra-low-dose, low-dose, and standard-dose CT of the kidney, ureters, and bladder: is there a difference? Results from a systematic review of the literature. Clinical Radiology. 2017. 72:11-15.
- Moore, C., Daniels, B., Ghita, M., Gunabushanam, G., Luty, S., Molinaro, A. M., et al. Accuracy of reduced-dose computed tomography for ureteral stones in emergency department patients. Annals of Emergency Medicine. 2015. 65:189-198.
- Nicolan, B., Greffier, J., Dabli, D., de Forges, H., Arcis, E., Al Zouabi, N., et al. Diagnostic performance of ultra-low dose versus standard dose CT for non-traumatic abdominal emergencies. Diagnostic and Interventional Imaging. 2021. 102: 379-387.
- Gavrielli, S., Yan, C., Rogalla, P., Anconina, R., & Metser, U. Ultra-low dose CT abdomen and pelvis for the detection of acute abdominal pathology in the emergency room: Initial experience from an academic hospital. Emergency Radiology. 2021. 28:15-21.
- Lei, B., Harfouch, N., Scheiner, J., Demissie, S., & Hayim, M. Can obstructive urolithiasis be safely excluded on contrast CT? A retrospective analysis of contrast-enhanced and noncontrast CT. The American Journal of Emergency Medicine. 2021. 47:70-73.
- Corwin, M., Lee, J., Fananapazir, G., Wilson, M., & Lamba, R. Detection of renal stones on portal venous phase CT: Comparison of thin axial and coronal maximum-intensity-projection images. American Journal of Roentgenology. 2016. 207:1200-1204.
- Choosing Wisely. 2014. https://www.choosingwisely.org/clinician-lists/acep-ct-of-abdomen-and-pelvis-for-ed-patients-under-50.
- Smith-Bindman, R., Aubin, C., Bailitz, J., Bengiamin, R. N., Camargo Jr, C. A., Corbo, J., et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. New England Journal of Medicine. 2014. 371:1100-1110.
- Alerhand, S. CT versus ultrasound for kidney stones. emDocs. 2014. http://www.emdocs.net/ct-vs-ultrasound-kidney-stones.
- Gottlieb, M., Hill, E. D., & Arno, K. Is Point-of-Care Ultrasonography Effective for the Diagnosis of Urolithiasis? Annals of Emergency Medicine. 2019. 73:517-519.
- Wong, C., Teitge, B., Ross, M., Young, P., Robertson, H., & Lang, E. The accuracy and prognostic value of point‐of‐care ultrasound for nephrolithiasis in the emergency department: A systematic review and meta‐Academic Emergency Medicine. 2018. 25:684-698.
- Türk, C., Neisius, A., Petrik, A., Seitz, C. Skolarikos, A., et al. EAU Guidelines on Urolithiasis. European Association of Urology. 2021. https://uroweb.org/guideline/urolithiasis.
- Moore, C., Bomann, S., Daniels, B., Luty, S., Molinaro, A., Singh, D., & Gross, C. Derivation and validation of a clinical prediction rule for uncomplicated ureteral stone—the STONE score: retrospective and prospective observational cohort studies. Bmj. 2014. 348.
- Daniels, B., Gross, C., Molinaro, A., Singh, D., Luty, S., Jessey, R., & Moore, C. L. (2016). STONE PLUS: evaluation of emergency department patients with suspected renal colic, using a clinical prediction tool combined with point-of-care limited ultrasonography. Annals of Emergency Medicine. 2016. 67:439-448.
- Wang, R., Rodriguez, R., Moghadassi, M., Noble, V., Bailitz, J., Mallin, M., et al. External validation of the STONE score, a clinical prediction rule for ureteral stone: An observational multi-institutional study. Annals of Emergency Medicine. 2016. 67:423-432.
- Hernandez, N., Song, Y., Noble, V., & Eisner, B. Predicting ureteral stones in emergency department patients with flank pain: An external validation of the STONE score. World Journal of Urology. 2016. 34:1443-1446.
- Schoenfeld, E. Poronsky, K., Elia, T., Budhram, G., Garb, J., & Mader, T. Validity of STONE scores in younger patients presenting with suspected uncomplicated renal colic. The American Journal of Emergency Medicine. 2016. 34:230-234.
- Kim, B., Kim, K., Kim, J., Jo, Y. H., Lee, J. H., Hwang, J. E., & Park, J. External validation of the STONE score and derivation of the modified STONE score. The American Journal of Emergency Medicine. 2016. 34:1567-1572.
- Fukuhara, H., Ichiyanagi, O., Midorikawa, S., Kakizaki, H., Kaneko, H., & Tsuchiya, N. Internal validation of a scoring system to evaluate the probability of ureteral stones: The CHOKAI score. The American Journal of Emergency Medicine. 2017. 35:1859-1866.
- Fukuhara, H., Kobayashi, T., Takai, S., Tawara, T., Kikuta, M., Sugiura, A., et al. External validation of the CHOKAI score for the prediction of ureteral stones: A multicenter prospective observational study. The American Journal of Emergency Medicine. 2020. 38:920-924.
- Eraybar, S., & Yuksel, M. The prospective evaluation of the effectiveness of scoring systems in the emergency department in cases with suspected ureteral stones: STONE? CHOKAI? The American Journal of Emergency Medicine. 2021.
- Balen, F., Bastouil, M., Charpentier, S., Game, X., Houze-Cerfon, C., & Lauque, D. Derivation of a clinical predicting rule for obstructive urolithiasis and alternative diagnosis requiring urgent intervention: the CLAD score. Urolithiasis. 2021. 49:145-152.
- Assimos, D., Krambeck, A., Miller, N., Monga, M., Murad, M., Nelson, C. et al. Surgical management of stones: American urological association/endourological society guideline, Part I. The Journal of Urology. 2016. 196:1153-1160.
- Marien, T., Mass, A., & Shah, O. Antimicrobial resistance patterns in cases of obstructive pyelonephritis secondary to stones. Urology. 2015. 85:64-68.
- Nicolle, L., Gupta, K., Bradley, S., et al. Clinical practice guidelines for the management of asymptomatic bacteriuria: 2019 update by the Infectious Disease Society of America. Clinical Infectious Disease. 68:10 e83-e110.
- De Lorenzis, E., Alba, A., Cepeda, M., Galan, J., Geavlete, P., Giannakopoulos, S., et al. Bacterial spectrum and antibiotic resistance of urinary tract infections in patients treated for upper urinary tract calculi: A multicenter analysis. European Journal of Clinical Microbiology & Infectious Diseases. 2020. 39:1971-1981.
- Wang, S., Zhang, Y., Zhang, X., & Li, J. An evaluation of multidrug-resistant bacteria in patients with urinary stone disease: Data from a high-volume stone management center. World Journal of Urology. 2020. 38: 425-432.
- Tauber, D. EM@3AM: Urolithiasis. emDocs. 2019. http://www.emdocs.net/em3am-urolithiasis.
- Hinojosa-Gonzalez, D., Torres-Martinez, M., Villegas-De Leon, S., Galindo-Garza, C., Roblesgil-Medrano, A., Alanis-Garza, C., et al. Emergent urinary decompression in acute stone-related urinary obstruction: A systematic review and meta-analysis. Journal of Clinical Urology. 2021.
- Mann, U., Jain, K., Wong, R., Li, Z., Eng, A., Blachman-Braun, R., & Patel, P. (2021). Predictors of mortality for patients admitted to the intensive care unit with obstructing septic stones. Canadian Urological Association Journal. 2021. 15.
- Yongzhi, L., Shi, Y., Jia, L., Yili, L., Xingwang, Z., & Xue, G. Risk factors for urinary tract infection in patients with urolithiasis—primary report of a single center cohort. BMC Urology. 2018. 18(1), 1-6.
- Coll, D., Varanelli, M., & Smith, R. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. American Journal of Roentgenology. 2002. 178:101-103.
- Jendeberg, J., Geijer, H., Alshamari, M., Cierzniak, B., & Lidén, M. (2017). Size matters: The width and location of a ureteral stone accurately predict the chance of spontaneous passage. European Radiology. 2017. 27:4775-4785.
- Li, X., Zhu, W., Lam, W., Yue, Y., Duan, H., & Zeng, G. Outcomes of long‐term follow‐up of asymptomatic renal stones and prediction of stone‐related events. BJU International. 2019. 123:485-492.
- Wang, R., Smith-Bindman, R., Whitaker, E., Neilson, J., Allen, I., Stoller, M., & Fahimi, J. Effect of tamsulosin on stone passage for ureteral stones: A systematic review and meta-analysis. Annals of Emergency Medicine. 2017. 69:353-361.
- Vermandere, M., Kuijpers, T., Burgers, J., Kunnamo, I., van Lieshout, J., Wallace, E., et al. (2018). Alpha-blockers for uncomplicated ureteral stones: a clinical practice guideline. BJU International. 2018. 122:924-931.
- Liu, X., Wen, J., Wan, Y., Hu, B., Wang, Q., & Wang, Y. Role of silodosin as medical expulsive therapy in ureteral calculi: A meta-analysis of randomized controlled trials. Urolithiasis. 2018. 46:211-218.
- Pathan, S., Mitra, B., & Cameron, P. A systematic review and meta-analysis comparing the efficacy of nonsteroidal anti-inflammatory drugs, opioids, and paracetamol in the treatment of acute renal colic. European Urology (2018). 73:583-595.
- Forouzanfar, M., Mohammadi, K., Hashemi, B., & Safari, S. Comparison of intravenous ibuprofen with intravenous ketorolac in renal colic pain management: A clinical trial. Anesthesiology and Pain Medicine. 2019. 9.
- Tramèr, M., Williams, J., Carroll, D., Wiffen, P., Moore, R., & McQuay, H. Comparing analgesic efficacy of non-steroidal anti-inflammatory drugs given by different routes in acute and chronic pain: A qualitative systematic review. Acta Anaesthesiologica Scandinavica. 1998. 42:71-9.
- Cisewski, D. Pain profiles: Intravenous lidocaine for intractable renal colic unresponsive to standard therapy. emDocs. 2018. http://www.emdocs.net/pain-profiles-intravenous-lidocaine-for-intractable-renal-colic-unresponsive-to-standard-therapy.
- LaPietra, A. Intravenous lidocaine for renal colic. ALiEM. 2018. https://www.aliem.com/intravenous-lidocaine-for-renal-colic.
- Makhoul, T., Kelly, G., Schult, R., & Acquisto, N. Intravenous lidocaine for renal colic in the emergency department. The American Journal of Emergency Medicine. 2019. 37:775.
- Managing Acute Pain in the ED: Intravenous lidocaine for renal colic. ACEP. https://www.acep.org/patient-care/map/map-intravenous-lidocaine-for-renal-colic-tool.
- Hosseininejad, S., Jahanian, F., Irankar, S., Moosazadeh, M., Hosseini, S., Shahbakhti, N., & Bozorgi, F. Comparing the analgesic efficacy of morphine plus ketamine versus morphine plus placebo in patients with acute renal colic: A double-blinded randomized controlled trial. The American Journal of Emergency Medicine. 2019. 37:1118-1123.
- Aydin, M., Tekin, E., Ahiskalioglu, E., Ates, I., Karagoz, S., Aydin, O. et al. (2021). Erector spinae plane block vs non‐steroidal anti‐inflammatory drugs for severe renal colic pain: A pilot clinical feasibility study. International Journal of Clinical Practice. 2021. 75:e13789.
- Kadioglu, E., Kaya, M., & Yildirim, H. Transversus abdominis plane block: A new method in renal colic pain management. The American Journal of Emergency Medicine. 2020. 38:2116-2118.
- Chitinis, S., Kabba D., Kulkarni, M. Nephrolithiasis: Diagnosis and management in the ED. emDocs. 2015. http://www.emdocs.net/nephrolithiasis-diagnosis-management-ed.
- Daniels, B., Schoenfeld, E., Taylor, A., Weisenthal, K., Singh, D., & Moore, C. Predictors of hospital admission and urological intervention in adult emergency department patients with computerized tomography confirmed ureteral stones. The Journal of Urology. 2017. 198:1359-1366.
- Pearle, M., Goldfarb, D., Assimos, D., Curhan, G., Denu-Ciocca, C., Matlaga, B., et al. Medical management of kidney stones: AUA guideline. The Journal of Urology. 2014. 192:316-324.
- Lin, B., Lin, M., Huang, R., Hong, Y., Lin, B., & He, X. Dietary and lifestyle factors for primary prevention of nephrolithiasis: A systematic review and meta-analysis. BMC Nephrology. 2020. 21:1-13.





1 thought on “Urolithiasis: ED Presentations, Evaluation, Management, and Disposition”
Regarding the ID issues, it was very nice that the authors referred to our work looking at occult infection among ED patients with typical KS presentations that found that while 1/2 of those infected had symptoms of fever to suggest that infection was present, the other 1/2 did not and infection risk factors were female sex, dysuria, past UTI, and the usual UA findings that connote infection. Women, who much more rarely get KS than men, have frequent entry of bacteria into their bladder b/o of the different anatomy, and the etiology of their stones is often r/t frequent past infections, so it is not surprising that women are at greater risk of infection when they get a KS.
While I like the rec – “A urinalysis and culture must be obtained on every patient in which ureteral stone is suspected or confirmed” – based on our findings, I also recommend empiric abx for females, and any patient with dysuria, past UTI, and those with abnl UAs c/w infection. This does not mean these patients require hospitalization, but they all require good education on when to return, a dose of abx before leaving, and careful C & S f/u. Of course, I cannot prove this practice (I have considered how a trial might be done, you know me) since infection complications are still very rare, although may be catastrophic. I would also be relatively more careful with patients larger, more proximal stones and any suggestion of infection risk.
Regarding empirical abx, I agree that fluoroquinolones are dicey in many areas b/o high resistance prevalences, and the big concern now is ESBLs. See our Jan 2021 Annals of EM article. So with regard to the authors’ antibiotic section, I’d amend to recommend this – for women, an advanced generation cephalosporin – like cefixime or cefepime (1st dose in ED, or following a dose of ceftriaxone), and for men, a shot of ertapenem and then a fluoroquinolone. men rarely get infected but, unfortunately, the prostate is assumed to be seeded and beta-lactams are no bueno in terms of prostate penetration. Carbapenems and fluoroquinolones do get into the prostate. Ertapenem is long-acting and will likely cover the patient long enough until the C&S is resulted, with still the majority of isolates will be susceptible to FQs. For those “high risk for resistance,” we are really talking about ESBLs, and a carbapenem is best, and for oral regimens, combination amox/clav and cefepime has an evidence base to treat ESBL infections (and clavulante may protect cefepime). Next IV choice might be a daily dose of amikacin. For those with past infections, the previous micro results should also be checked to guide abx selection.
Since stones take some time to pass, I give a 10 day Rx, which I stop in men if the C &S is [-], but continue in women “prophylactically” if the initial C &S is [-] b/o of their continued risk to develop infection while the stone foreign body is hanging around and bugs continuous wash up into the bladder. Anyone with a [+] C & S, I call back for clinical reeval asap.