
Author: Cameron Jones, MD, MPH (EM Resident Physician, Northwestern Memorial Hospital, Chicago, IL) // Reviewed by: Bryant Allen, MD (EM Attending Physician, Carolinas Medical Center, Charlotte, NC); Alex Koyfman, MD (@EMHighAK); Marina Boushra, MD; Brit Long, MD (@long_brit)
Case
A 43-year-old male arrives as a level 1 trauma activation after a motor vehicle collision. The patient is secured to a backboard and in a c-collar, with the following vitals: HR 107, BP 165/89, O2 saturation 95% on non-rebreather, RR 25. Primary survey reveals significant face and head trauma with moderate blood in the airway requiring repeated suctioning, bilateral breath sounds, intact extremity pulses, GCS 6. The patient clearly needs to be intubated for airway protection, and, as you and your team prepare for the procedure, you glance over at the different laryngoscopes you have available: a traditional non-video blade, a standard-geometry (Macintosh/Miller) video laryngoscope (VL), and a hyper-angulated video laryngoscope. Given the complicating factors, including the need for c-spine stabilization, a soiled airway, and possible traumatic brain injury, what device should you choose? How will your positioning and technique differ depending on your choice?
What are the options for video laryngoscopes?
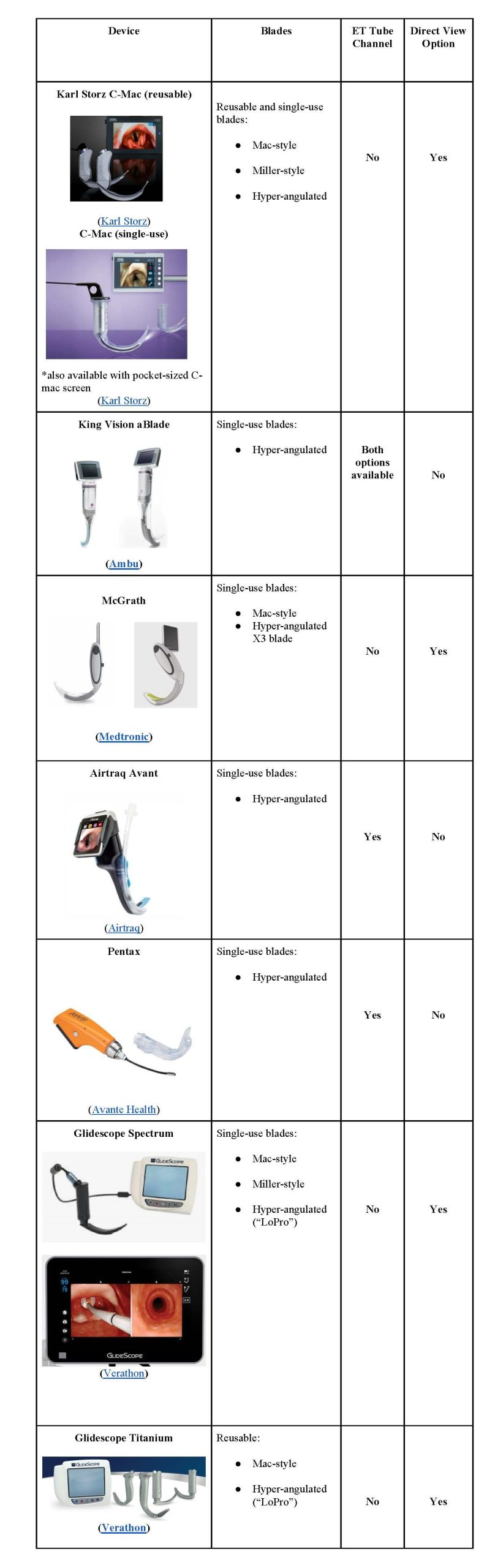
To answer this question, we must be careful about the terminology used when describing devices. Simply referring to a device as a video laryngoscope or VL blade, or using brand names such as “C-Mac” or “Glidescope,” can lead to confusion, as these terms encompass multiple different devices with different advantages/disadvantages and accompanying techniques. There are several broad categories of video laryngoscopes (see the below table for specific brands/devices):
- VLs (Video Laryngoscopes) with standard geometry blades allow for both indirect (video) and direct views
- VLs with hyper-angulated blades are designed to improve your indirect view but do not allow for direct views
- VLs with hyper-angulated blades with a dedicated channel to facilitate ET tube passage
What are the differences in technique between video and direct laryngoscopy?
For standard-geometry video laryngoscopes (SGVL) that allow both indirect and direct viewing, the operator can choose to ignore the video screen entirely and use the blade as they would a DL Mac or Miller blade. These devices have been used in many training environments to augment teaching by letting the learner utilize the blade in DL function while the instructor and/or other learners view the video screen to better understand and describe the relevant anatomy.1 Allowing other members of the team to view laryngoscopy may also facilitate better team dynamics and permit improved head or cricoid manipulation by assistants if necessary.2 When used as an indirect VL device, the operator benefits from the camera view to aid in visualizing the glottis. However, placement of the blade, suctioning of the airway, elevation of the epiglottis, and passage of the ET tube can be performed similarly to DL.3
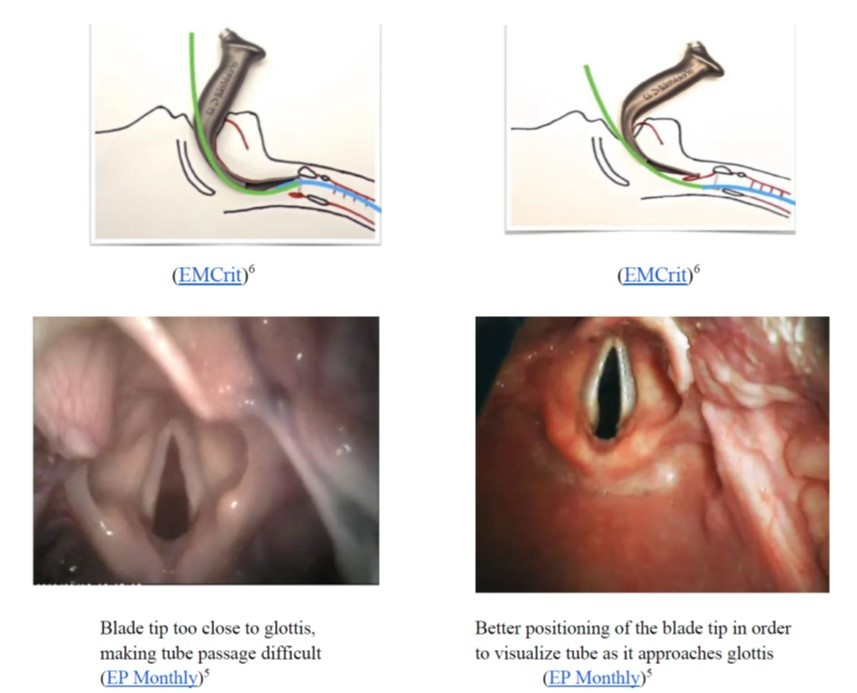
For hyper-angulated video laryngoscopes (HAVL) that only allow indirect viewing, operators must utilize the device’s video screen and cannot use the hyper-angulated blade to obtain a direct view. Operators typically use a rigid stylet that molds the ET tube to a curvature designed to facilitate passage along the hyper-angulated blade (though, if unavailable, a traditional stylet can be molded to a similar angle). In addition, placement of the blade’s tip and maneuvering of the blade in order to view the glottic opening is notably different from DL technique. While obtaining a sufficient view of the cords is often the most challenging step of DL, conversely, obtaining a Grade 1 view with HAVL is often the easiest step, while passing the ET tube around this angle and through the cords can prove to be surprisingly challenging.1,4,5,6
Key points for using HAVL devices
- Most experts recommend slowly advancing the hyper-angulated blade along the middle of the tongue rather than sweeping the tongue to the left as is traditionally done in DL1,4,5,6
- It is important to advance slowly as it is easy to overshoot with these devices and end up in a pool of fluid or a wall of tissue, requiring the operator to back out and re-orient
- Operators should resist obtaining a perfect view by bringing the blade tip too near the glottis or angling the blade up to bring the glottis to the center of the screen:4,5,6,7
- Tube insertion should also be performed with slow movements, advancing the tube under direct visualization until the tip is in view on camera, then adjusting its trajectory with micro-movements
- Certain devices (see above) have a channel incorporated into the blade through which the ET tube is passed
- Because operators are only using an indirect (video) view, the tube can be passed more centrally, following the curve of the blade, rather than inserting from the side
- The rigid stylet used with HAVL can sometimes get caught near the tracheal opening, requiring rotation of the tube & stylet or partial removal of the stylet before fully passing the tube through the cords (airway instructor Dr. Richard Levitan coined this maneuver “Stop, Pop, and Drop”)5
What is the evidence for use of video laryngoscopy in the emergency department?
- 2016 Cochrane review10 found:
- Significantly fewer failed intubations using VL in both straightforward and anticipated difficult airways
- No differences in first-pass success rate, hypoxic time, or mortality.
- Only 3 of the 64 studies were in ED settings.
- 2017 prospective, observational study11 comparing VL and DL in soiled (blood- or vomitus-stained) airways found:
- Higher first-pass success rate with VL in both soiled and clean airways
- Similar reduction in first-pass success rate in soiled airways compared to clean airways with both DL and VL
- 2018 meta-analysis12 found:
- No difference in first-pass or overall intubation success rate and no difference in mortality
- Fewer esophageal intubations using VL
- All patients in included studies were adult ED patients
- 2020 Best Evidence Topic review (BET 2)13 found:
- Significantly higher first-pass success rate, fewer esophageal intubations using VL.
- No mortality difference, no difference in any outcomes among senior/experienced operators.
- 2020 retrospective National Emergency Airway Registry (NEAR) study14 comparing SGVL and HAVL in ED intubations found:
- Slightly higher first-pass success-rate with SGVL, but no difference after covariate adjustment with regression model
- No difference in peri-intubation adverse events
- HAVL was used more frequently in trauma and in anticipated and confirmed difficult airways
Unfortunately, some of these studies also fail to delineate the specific devices used, making it difficult to fully compare first-pass success rates between the various categories of VL, or obtain sub-group analyses to better understand which devices may be more successful for specific patients.
Where do we go from here?
Given the variety of devices and blades that have emerged in the past few years, it is important for researchers to be specific about exactly which VL is being studied. The available evidence shows there is still a gap between the excellent laryngeal views typically obtained with VL and the first-pass success rate of intubations. This data emphasizes the need for specific instruction and development of the distinct hands-on skills of video laryngoscopy, especially when it comes to using HAVL. Operators must also ensure they are familiar with all of the different VL devices, blades, and stylets that are stocked at their institution.
The widespread availability of SGVL, which allows both direct and video-augmented laryngoscopy, makes the debate between video and direct a moot point. Instead, the choice facing many emergency physicians (EPs) when approaching an intubation is between SGVL and HAVL. The question of exactly how these devices should fit into a difficult airway algorithm remains unsettled. However, trainees should become familiar with all of these options and receive training specific to each device. Planning for intubation may also require a more nuanced understanding of the predicted difficult airway (c-collar precautions vs obesity vs contaminated airway) in order to choose the ideal device for intubation.
Some have suggested that SGVL should be the go-to device for the majority of ED intubations, as it allows use of familiar airway manipulation techniques and adjuncts (e.g. Bougie), facilitates easier suctioning or foreign-body retrieval, and allows seamless transition between direct and video-augmented laryngoscopy.6,15 In this model, HAVL would be reserved for patients in which it is important to minimize force or head manipulation (e.g. c-spine precautions) or those in whom a glottic view is likely to be difficult to obtain (e.g. airway mass or morbid obesity). It may also make sense for trainees to learn airway anatomy and master the initial skills of SGVL, which translate easily to traditional DL, before building in the specific skill set for HAVL.16 Ideally, when formulating an airway plan, EM providers should become accustomed to incorporating all options into their primary and backup plans (e.g. first attempt with SGVL, using video as needed, and second attempt with HAVL if views are more difficult to obtain than anticipated).
Take-Home Points
- Video laryngoscopes include standard-geometry blades (SGVL), hyper-angulated blades (HAVL), and hyper-angulated blades with an ET tube channel.
- While SGVL involves similar technique to classic DL blades, HAVL requires a specific skill set, particularly when it comes to tube insertion.
- There is some evidence that VL may increase first-pass and overall intubation-success rate, but the data in ED-based studies is still mixed.
- The availability of SGVL also makes the “VL vs DL” debate obsolete, and EPs should instead focus on building both HAVL and SGVL into their airway algorithms.
- There is limited evidence comparing HAVL and SGVL, and future prospective trials may inform selection of specific devices for certain clinical scenarios.
References
- Phelan MP, Dhimar J. Techniques for Improving Video Laryngoscopy With a Hyperangulated Blade. Acad Emerg Med. 2016;23(8):e15-e15. doi:10.1111/ACEM.13011
- Kelly FE, Cook TM, Boniface N, Hughes J, Seller C, Simpson T. Videolaryngoscopes confer benefits in human factors in addition to technical skills. Br J Anaesth. 2015;115(1):132-133. doi:10.1093/BJA/AEV188
- Paolini JB, Donati F, Drolet P. Review article: Video-laryngoscopy: Another tool for difficult intubation or a new paradigm in airway management? Can J Anesth. 2013;60(2):184-191. doi:10.1007/S12630-012-9859-5/FIGURES/2
- Levitan, Richard M. “Tips for Using a Hyperangulated Video Laryngoscope.” [online] ACEP Now. Available at: https://www.acepnow.com/article/tips-for-using-a-hyperangulated-video-laryngoscope/?singlepage=1.[Accessed 11 February 2022]
- Levitan, R., 2013. “Four Secrets To Video Laryngoscopy.” [online] EP Monthly. Available at: https://epmonthly.com/article/four-secrets-to-video-laryngoscopy-/ [Accessed 11 February 2022]
- Kovacs, G., 2020. Lights Camera Action: Redirecting Videolaryngoscopy. [Blog] EMCrit, Available at: https://emcrit.org/emcrit/redirecting-videolaryngoscopy/ [Accessed 13 October 2020].
- Gu Y, Robert J, Kovacs G, et al. A deliberately restricted laryngeal view with the GlideScope® video laryngoscope is associated with faster and easier tracheal intubation when compared with a full glottic view: a randomized clinical trial. Can J Anesth. 2016;63(8):928-937. doi:10.1007/S12630-016-0654-6/FIGURES/4
- AIME Airway, 2015. VL Pearl: Not So Close. Available at: https://youtu.be/9DuSzt41dBo?t=117 [Accessed 20 October 2020].
- Levitan, Richard. “Hyperangulated Glidescope Titanium blade in super obese man with omega shaped epiglottis.” Available at https://vimeo.com/123057240
- Lewis, S., Butler, A., Parker, J., Cook, T. and Smith, A., 2016. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database of Systematic Reviews, Available at: https://doi.org/10.1002/14651858.CD011136.pub2
- Sakles, J., Corn, G., Hollinger, P., Arcaris, B., Patanwala, A. and Mosier, J., 2017. The Impact of a Soiled Airway on Intubation Success in the Emergency Department When Using the GlideScope or the Direct Laryngoscope. Academic Emergency Medicine, 24(5), pp.628-636. Available at: https://doi-org.ezproxy.galter.northwestern.edu/10.1111/acem.13160
- Bhattacharjee, S., Maitra, S. and Baidya, D., 2018. A comparison between video laryngoscopy and direct laryngoscopy for endotracheal intubation in the emergency department: A meta-analysis of randomized controlled trials. Journal of Clinical Anesthesia, 47, pp.21-26. Available at: https://doi.org/10.1016/j.jclinane.2018.03.006
- Howson, A., Goodliff, A. and Horner, D., 2020. BET 2: Video laryngoscopy for patients requiring endotracheal intubation in the emergency department. Emergency Medicine Journal, 37(6), pp.381-383. Available at: https://10.1136/emermed-2020-209962.3
- Driver BE, Prekker ME, Reardon RF, Fantegrossi A, Walls RM, Brown CA. Comparing Emergency Department First-Attempt Intubation Success With Standard-Geometry and Hyperangulated Video Laryngoscopes. Ann Emerg Med. 2020;76(3):332-338. doi:10.1016/J.ANNEMERGMED.2020.03.011
- Farkas J.: 10 Pearls from the Levitan Airway Course. EMCrit. Available at https://emcrit.org/pulmcrit/10-pearls-from-the-levitan-airway-course/ [accessed 25 February 2022]
- Strayer R. Strayerism: Video Laryngoscopy Nomenclature. EM:RAP. Available at https://www.emrap.org/episode/emrap202113/strayerismvideo. [accessed 27 February 2022]




