
Author: Daniel M. Good, MD, MPH (EM Resident, UTSW/Parkland Memorial, Dallas, TX) // Edited by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 32-year-old male presents to the ED with vomiting and abdominal cramping for the past 2 days. He reports a history of Crohn disease and has been poorly compliant with his maintenance regimen. He has been hospitalized 5 times in the past 2 years for Crohn flares. His current episode began as right lower abdominal pain 1 week ago with several episodes of watery diarrhea daily. He developed diffuse cramping, nausea, and vomiting 2 days ago and has been unable to tolerate any oral intake. He has not passed stool or flatus in 2 days. On exam, his pulse is 110/minute, blood pressure 112/83, respirations 18/minute, temperature 37.6ºC. His abdomen is distended with hyperactive, high-pitched bowel sounds, increased tympany to percussion, and diffuse mild tenderness to palpation without rebound or guarding. Upright abdominal x-ray shows multiple air-fluid levels in the small bowel with a paucity of colonic gas.
What is the most likely diagnosis?
Answer: Crohn’s disease exacerbation complicated by a small bowel obstruction
Epidemiology
- IBD is a chronic relapsing disease with unpredictable and highly variable relapsing rates.
- Initial presentation of IBD can occur at any age, but predominantly occurs in 2nd to 4th decade of life.1
- Ulcerative colitis
- Incidence in North America is 19.2 per 100,000 person-years1
- Prevalence in North America is 249 per 100,000 persons1
- Crohn’s disease
- Incidence in North American is 20.2 per 100,000 person-years1
- Prevalence in North American is 319 per 100,000 persons1
- Highest prevalence among Caucasians and those of Jewish descent, but increasing prevalence among those of African and Asian descent.2
- Inconsistent reports of gender bias.2
- Those with an affected first-degree relative have a 10-fold increased risk of developing the same subtype of IBD, but no significant risk of developing the other subtype.3
Pathophysiology4
- The pathogenesis of IBD complex, not fully known, and multifactorial. IBD has been linked to different environmental, genetic, microbial, and immune factors. There is likely an interaction between the gastrointestinal (GI) flora and immune system, in a susceptible individual, that leads to inflammation of a portion of the GI tract.
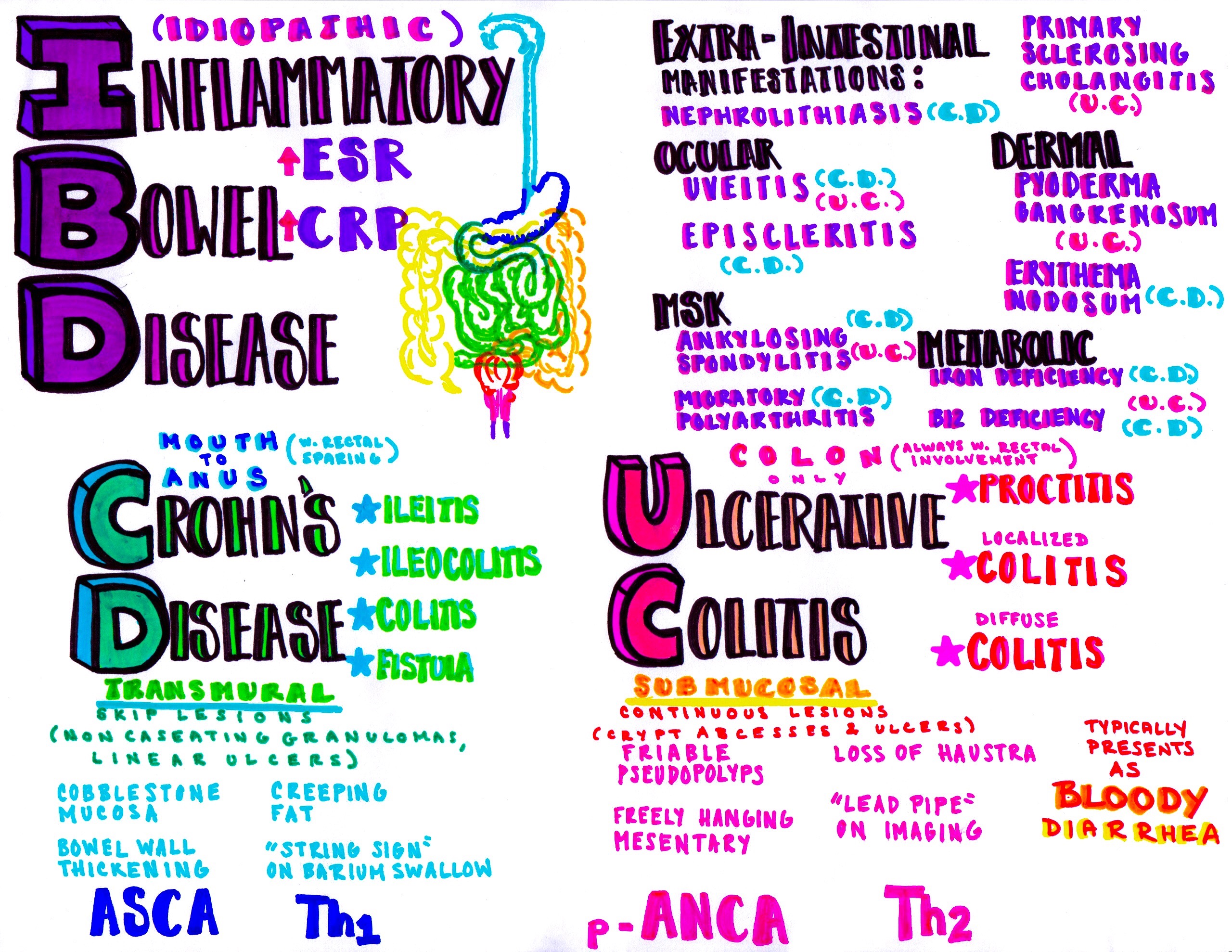
- Location of depth of GI tract involvement differs between IBD subtype
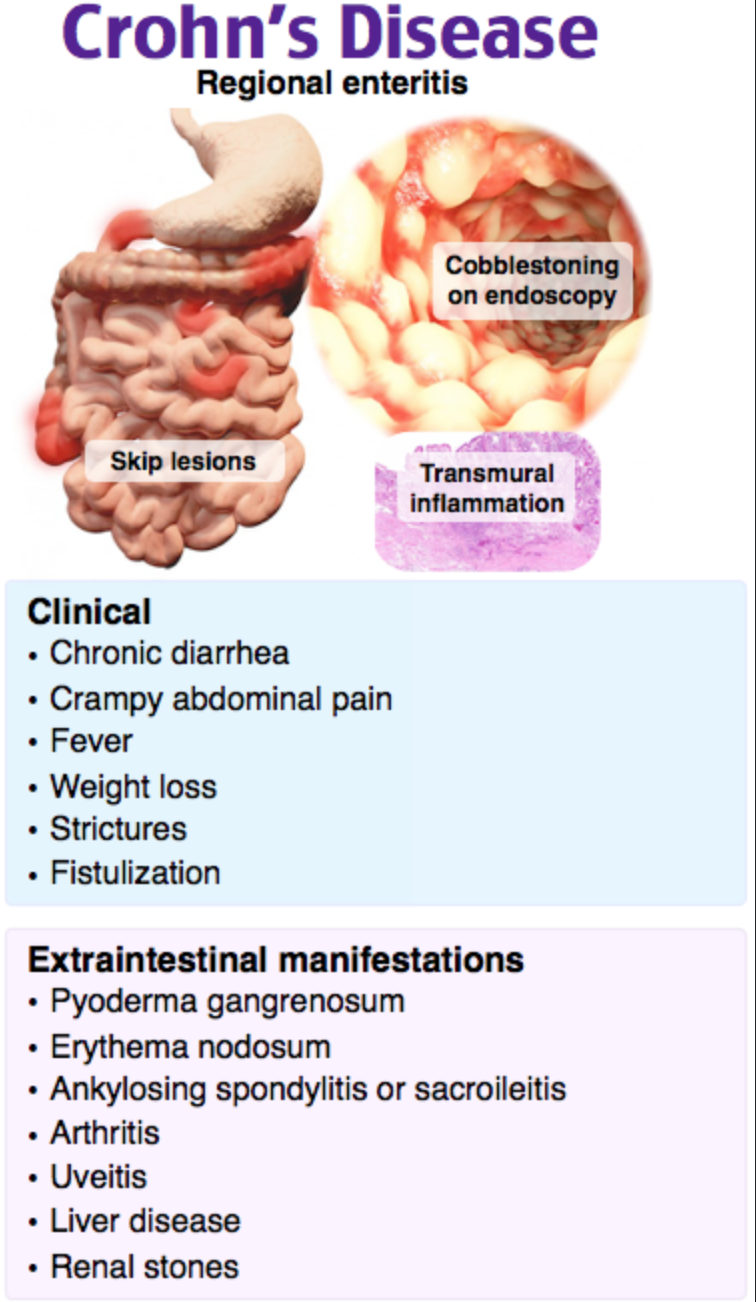
- Crohn’s Disease
- Affects any portion of the GI tract, except the rectum, which is typically spared. The terminal ileum is the most common location involved.
- Typified by areas of inflamed bowel with intervening unaffected bowel, referred to as skip lesions.
- Transmural inflammation causes a predilection for many of the complications seen in Crohn disease.
- Ulcerative Colitis
- Involves the rectum. The area of inflammation can progress proximally in a step-wise fashion to involve other areas of the colon. Can range from isolated rectal involvement to pancolitis.
- Inflammation is limited to mucosa and submucosa layers and thus does not typically cause the obstructive complications seen in Crohn’s disease.
- Crohn’s Disease
Presentation
- The presentation of an IBD flare can range from a stable patient with worsening of typical symptoms to a patient in extremis with severe hypovolemic or septic shock.5
- Systemic symptoms such as fever, malaise, and weight loss are common.5
- Some features are classically attributed each IBD subtype, however overlap is common.
- Ulcerative colitis
- Bloody diarrhea that may contain mucus, fecal urgency, proctalgia, left-sided or diffuse abdominal pain, occasionally severe constipation.5
- Severity of disease clinical disease activity indices (ACG, ECCO, JSG) have been proposed and are based on number of bloody stools daily, as well as presence or absence of fever, anemia, elevated ESR/CRP, and tachycardia. These indices appear to have a moderately good correlation to severity of endoscopic findings.6
- Crohn’s disease
- Watery diarrhea, nausea, weight loss, and colicky abdominal pain.5
- May present with hematochezia if colonic involvement.5
- The Crohn Disease Activity Index and Harvey-Bradshaw Index have been proposed for grading disease severity, however they appear to have poor correlation with the degree of mucosal inflammation.6
Extra-intestinal Disease Manifestations7
- Extra-intestinal manifestations are typically concurrent with intestinal disease and improve with treatment of the IBD flare, with the exception of renal and biliary calculus disease, fatty liver, and primary sclerosing cholangitis.
- Ocular: Anterior uveitis, episcleritis
- Dermatologic: Pyoderma gangrenosum or erythema nodosum
- Musculoskeletal: Sacroilitis or migratory polyarthritis
- Renal: Calcium oxalate stones
- Hepatobiliary: Cholelithiasis/cholecystitis, autoimmune hepatitis, primary sclerosis cholangitis, fatty liver disease
- Hematologic: Iron deficiency anemia, anemia of chronic disease, reactive thrombocytosis
Complications5,7
- Ileus or bowel obstruction:
- Presents at nausea and vomiting with abdominal distention and obstipation. More commonly seen in long-standing Crohn’s disease.
- Abscess formation:
- Presents as fever, abdominal pain with tenderness +/- palpable mass. More commonly seen in Crohn’s disease.
- Perforation:
- Presents as fever and abdominal pain with peritoneal signs. Seen in Crohn’s disease or as a complication of toxic megacolon or fulminant colitis in patients with ulcerative colitis.
- Toxic megacolon:
- Can be the initial presentation of Crohn’s disease or ulcerative colitis. Diagnostic criteria include colonic dilation (>6 cm) PLUS ≥ 3:
- Fever >38ºC
- Leukocytosis
- Anemia
- Pulse >120/minute
- Can be the initial presentation of Crohn’s disease or ulcerative colitis. Diagnostic criteria include colonic dilation (>6 cm) PLUS ≥ 3:
-
-
- PLUS ≥ 1: hypotension, electrolyte disturbances, altered mental status, dehydration
-
- Fulminant colitis:
- Presents as fever, anorexia, abdominal distention, persistent rectal bleeding, and >10 stools per day. Seen in patients with ulcerative colitis.
- Sepsis
- Venous thromboembolism:
- 3-fold increased risk compared to general population.9
Evaluation
Laboratory5,7
- Complete blood count to evaluate for anemia and reactive thrombocytosis.
- Metabolic panel and liver panel to evaluate for acid-base disturbance, diarrhea-induced hypokalemia, concurrent biliary disease, hepatic or renal injury.
- Lipase to evaluate for concurrent pancreatitis.
- Urinalysis to evaluate for concurrent infection.
- Erythrocyte sedimentation rate and C-reactive protein to evaluate to disease activity.
- Several studies have shown poor correlation between endoscopic disease activity and ESR and CRP levels. One study revealed 28% of patients with active Crohn’s disease and 42% of patients with active ulcerative colitis had normal ESR and CRP levels.8
- Lactate and blood cultures in acutely ill-appearing patients to guide resuscitation and direct future antibiotic therapy.
- Stool studies in those with diarrhea to evaluate for concurrent viral, bacterial, and/or parasitic infection, including C. difficile.10
Imaging
- CT abdomen/pelvis with intravenous contrast to evaluate for complications such as obstruction, perforation, fistula formation, fulminant colitis, abscess formation, or toxic megacolon.11
- CT does not accurately characterize disease severity of ulcerative colitis. Admission for endoscopy may be appropriate.
- Sensitivity of 67% and specificity of 90% for diagnosing IBD.12
- Sensitivity of 85% and specificity of 95% for abscess formation.12
- Sensitivity of 85% and specificity of 100% for obstruction.12
- Sensitivity of 70% and specificity of 97% for fistula formation.12
- MR enterography or CT enterography may be appropriate in a stable patient if study is readily available from the ED.
- Enterography approaches 100% sensitivity and 100% specificity for detecting stenotic lesions in Crohn’s disease.11
*Consider evaluation for venous thromboembolic disease in the appropriate clinical setting, as patients are at increased risk.
ED Management5,7
- Initial ED management is dependent on whether or not the patient is acutely ill-appearing.
- Unstable or acutely ill-appearing:
- ABCs, IV access, and IV crystalloid resuscitation.
- Empiric IV antibiotics with enteric coverage (ciprofloxacin and metronidazole OR piperacillin-tazobactam).
- High-dose IV steroids.
- Laboratory and imaging evaluation as above.
- Stable:
- IV analgesia and anti-emetics.
- IV crystalloid if reported vomiting or diarrhea.
- Laboratory studies as above.
- May not require ED imaging if suspicion for complicated disease is sufficiently low.
- Unstable or acutely ill-appearing:
Disposition
- Ultimate disposition is dependent on the stability of the patient and the presence or absence of disease complications.
- Complicated IBD flare with toxic megacolon, fulminant colitis, perforation, significant hemorrhage:
- All are indications for emergent surgery – emergent surgical consultation.7,13
- Admission with gastroenterology consultation.
- Complicated IBD flare with abscess, ileus, small bowel obstruction:
- May require urgent surgical intervention.7,13
- Obstruction may resolve with steroids or newer biologic agents and obviate need for surgery.5
- Abscess may be amenable to percutaneous drainage by interventional radiology.7
- Admission with surgical and gastroenterology consultation.
- Complicated IBD flare with sepsis or venous thromboembolism:7
- Admission with gastroenterology consult.
- Uncomplicated IBD flare with persistent symptoms:7
- Admission with gastroenterology consult for symptom control, IV steroids, and possible inpatient endoscopy.
- Uncomplicated IBD with improved symptoms, tolerating oral intake and hemodynamically stable:7
- Discharge with outpatient gastroenterology follow up.
- Consider PO steroids.
- Complicated IBD flare with toxic megacolon, fulminant colitis, perforation, significant hemorrhage:
From Dr. Katy Hanson at Hanson’s Anatomy:

Which of the following complications is most common in patients with Crohn’s disease?
A) Bloody diarrhea
B) Malignancy
C) Perianal disease
D) Toxic megacolon
Answer: C
Crohn’s disease is a chronic granulomatous inflammatory disease involving any part of the GI tract from mouth to anus, most commonly the ileum and the anus. It is also called regional enteritis due to “skip areas” between involved segments of bowel. Patients present with episodes of abdominal pain, diarrhea, fever, and weight loss. They may look like appendicitis with right lower quadrant pain due to terminal ileitis. A very common complication affecting 90% of patients is perianal disease, such as abscess, fissure, fistula, or rectal prolapse. Fistulas and abscesses can also occur elsewhere in the bowel, along with obstruction, perforation, and peritonitis. Most patients will require surgery at some point. Extraintestinal manifestations affect about one-third of patients and may include arthritis, vasculitis, thromboembolic disease, hepatobiliary disease, erythema nodosum, pyoderma gangrenosum, uveitis, and renal calculi. Peak incidence is bimodal around ages 20 and 60. Initial diagnosis is confirmed by colonoscopy. Management includes evaluation for complications, therapy with antibiotics, mesalamine for mild disease or steroids for severe disease, and supportive care with analgesics, antidiarrheal agents, fluids, electrolyte replacement, and gradual resumption of lactose-free diet.
Patients with Crohn’s disease tend to have occult blood in their stool but do not often have grossly bloody diarrhea (A). In contrast, ulcerative colitis presents with bloody diarrhea, crampy abdominal pain, and tenesmus. Ulcerative colitis always begins at and spreads proximally from the rectum. Malignancy (B) is not nearly as common as perianal complications in Crohn’s disease. Compared with the general population, malignancy is about three times more common in patients with Crohn’s disease, and about 15 times more common in patients with ulcerative colitis. Toxic megacolon (D) is rare in Crohn’s disease. It is more common in ulcerative colitis, indicating avoidance of antidiarrheal agents and antibiotics in patients with ulcerative colitis.
Further Reading:
More FOAMed:
- Carter MJ, Lobo AJ, Travis SPL. Guidelines for the management of inflammatory bowel disease in adults. Gut 2004;53:v1-v16. http://dx.doi.org/10.1136/gut.2004.043372
- Crohn Disease. https://radiopaedia.org/articles/crohn-disease-1
- Ulcerative Colitis. https://radiopaedia.org/articles/ulcerative-colitis?lang=us
References:
- Molodecky, NA, Soon IS, Rabi DM, et al. Increasing Incidence and Prevalence of Inflammatory Bowel Diseases with Time, Based on Systematic Review. Gastroenterology. 2011. 142 (1): 46-52.
- Hou JK, El-Serag H, and Thirumurthi S: Distribution and manifestations of inflammatory bowel disease in Asians, Hispanics, and African Americans: a systematic review. Am J Gastroenterol. 2009. 104: 2100-2109.
- Orholm, M, Munkholm P, Langholz E, et al. Familial Occurrence of Inflammatory Bowel Disease. N Engl J Med. Jan, 1991. 324(2): 84-88.
- Zhyang, YZ and Li, YY. Inflammatory bowel disease: Pathogenesis. World J Gastroenerol. Jan, 2014. 20(1). 91-99.
- Walls, R, et al. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 9th ed., Elsevier, 2017.
- Peyrin-Biroulet L, Panes J, Sandborn WJ, et al. Defining Disease Severity in Inflammatory Bowel Disease: Current and Future Directions. Clin Gastroenterol Hepatol. Mar, 2016. 14(3):348-354.
- Burg MD, Riccoboni ST, Nusbam J, et al. Management of Inflammatory Bowel Disease in the Emergency Department. Emerg Med Pract. Nov, 2017. 19(11): 1-20.
- Alper A, Zhang L, Pashanker DS. Correlation of Erythrocyte Sedimentaiton Rate and C-Reactive Protein With Pediatric Inflammatory Bowel Disease Activity. J Pediatr Gastroenterol Nutr. Aug, 2017. 65(2): e25-27.
- Bernstein, CN, Blanchard, JF, Houston, DS, et al. The Incidence of Deep Vein Thrombosis and Pulmonary Embolism Among Patients With Inflammatory Bowel Disease: A Population-based Cohort Study. Thromb Haemost. March, 2001. 85(3): 430-434.
- Khanna S, Shin A, Kelly CP. Management of Clostridium difficile Infection in Inflammatory Bowel Disease: Expert Review from the Clinical Practice Updates Committee of the AGA Institute. Clin Gastroenterol Hepatol. Feb, 2017. 15(2): 166-174.
- Griffey RT, Fowler KJ, Thielen A, et al. Considerations in Imaging Among Emergency Department Patients With Inflammatory Bowel Disease. Ann Emerg Med. May, 2017. 69(5): 587-599.
- Panes J, Bouhnik Y, Reinisch W, et al. Imaging techniques for assessment of inflammatory bowel disease: Joint ECCO and ESGAR evidence-based consensus guidelines. J Crohns Colitis. Sept, 2010. 25(5): 349-354.
- Grucela A, Steinhagen RM. Current Surgical Management of Ulcerative Colitis. Mt Sinai J Med. Dec, 2009. 76(6): 606-612.





1 thought on “EM@3AM: Inflammatory Bowel Disease”
Pingback: IBD – översikt – Mind palace of an ER doc