Today on the emDOCs cast, Brit Long, MD (@long_brit) covers Part 1 in a series on complications of CAR T-cell therapy, specifically cytokine release syndrome (CRS).
Episode 77: CAR T-cell Therapy and Cytokine Release Syndrome
Background
- Vast array of new cancer therapies, including chimeric antigen receptor (CAR) T-cell therapy, antibodies, cytokines, oncolytic viruses, and vaccines.
- CAR T-cell therapy is a type of immunomodulation which uses genetically modified T-cells to attack malignant cells.
- Primarily used for ALL, CLL, Non-Hodgkin’s, multiple myeloma. Currently under study for Hodgkin’s lymphoma and solid tumors.
Mechanism:
- CAR T cell therapy involves T cells attacking cancer cells.
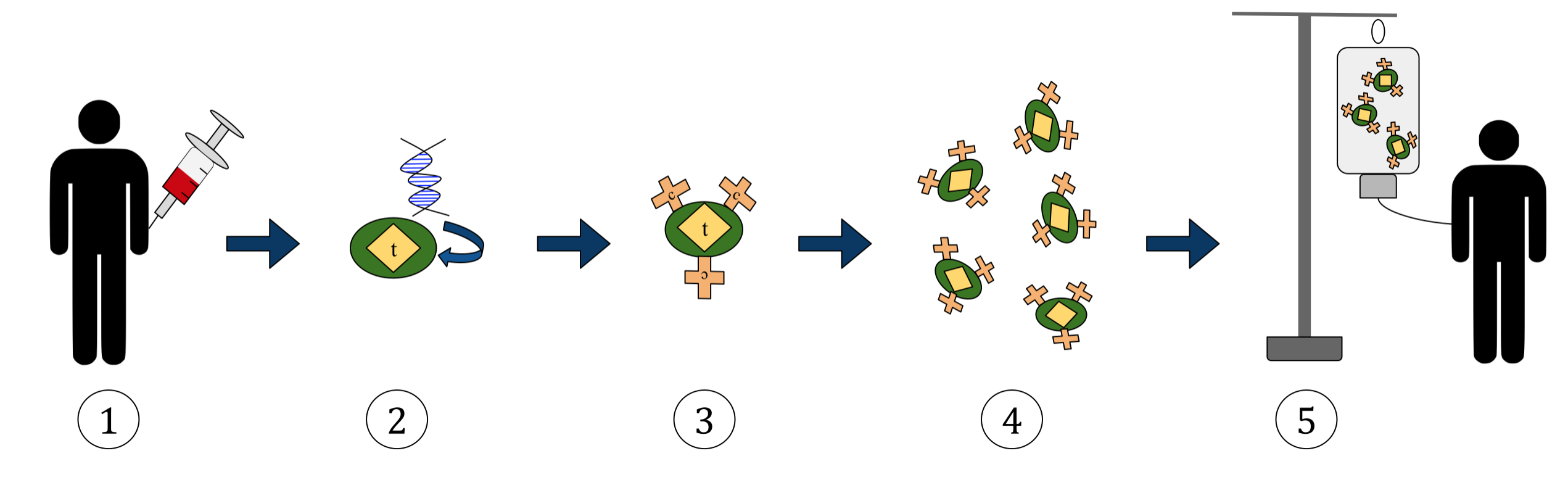
- Process:
- 1. T-cells present in the blood are removed from the patient or from a donor (less common).
- 2. T-cells are incorporated with the gene encoding specific antigen receptors.
- 3. This results in CAR receptors on the surface of T-cells.
- 4. The modified T-cells are harvested and grown in a laboratory setting.
- 5. The patient undergoes chemotherapy for lymphocyte depletion, and then the engineered T-cells are finally administered to the original patient.
Complications
- Infusion usually occurs in the outpatient setting.
- The two major complications of CAR T-cell therapy include cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS), or CAR T-cell-related encephalopathy syndrome (CRES).
- Others are infusion reaction, hypogammaglobulinemia, tumor lysis syndrome (TLS), cytopenias, cardiac toxicity, and graft-versus-host disease (GVHD).
Cytokine Release Syndrome
- CRS is a serious complication with fever and multiorgan dysfunction (Figure 2).
- CRS is a supraphysiologic response to CAR T-cell therapy that leads to elevated cytokine activity (interleukin (IL) 6, interferon (IFN), and tumor necrosis factor (TNF) alpha) and activation of endothelial cells, macrophages, and T-cells.
- CRS occurs in 25%-50% of patients treated with CAR T-cell therapy for ALL, but the incidence is lower in patients with NHL, CLL, and multiple myeloma.
- Severity is associated with the disease burden of the malignancy, molecular design, level of T-cell activation in response to CAR T-cell infusion, lymphodepletion prior to infusion, and dose of CAR T-cells
- Onset of symptoms is 1-14 days after therapy, but severe CRS usually occurs shortly after CAR T cell therapy. Duration can be days to weeks.
- Signs/symptoms range from mild, flu-like symptoms to severe, life-threatening inflammation and end organ injury. Fever has to be present for the diagnostic criteria.
- Mild symptoms include rash, headache, myalgias, and fatigue.
- Gastrointestinal symptoms, including nausea, vomiting, and diarrhea, are common.
- Severe, uncontrolled CRS may include circulatory collapse, vascular leakage, edema, renal failure, cardiac dysfunction, and multiorgan failure.
- Neurologic symptoms can occur several days after the onset of CRS and include aphasia, altered mental status, weakness, seizures, and cerebral edema.
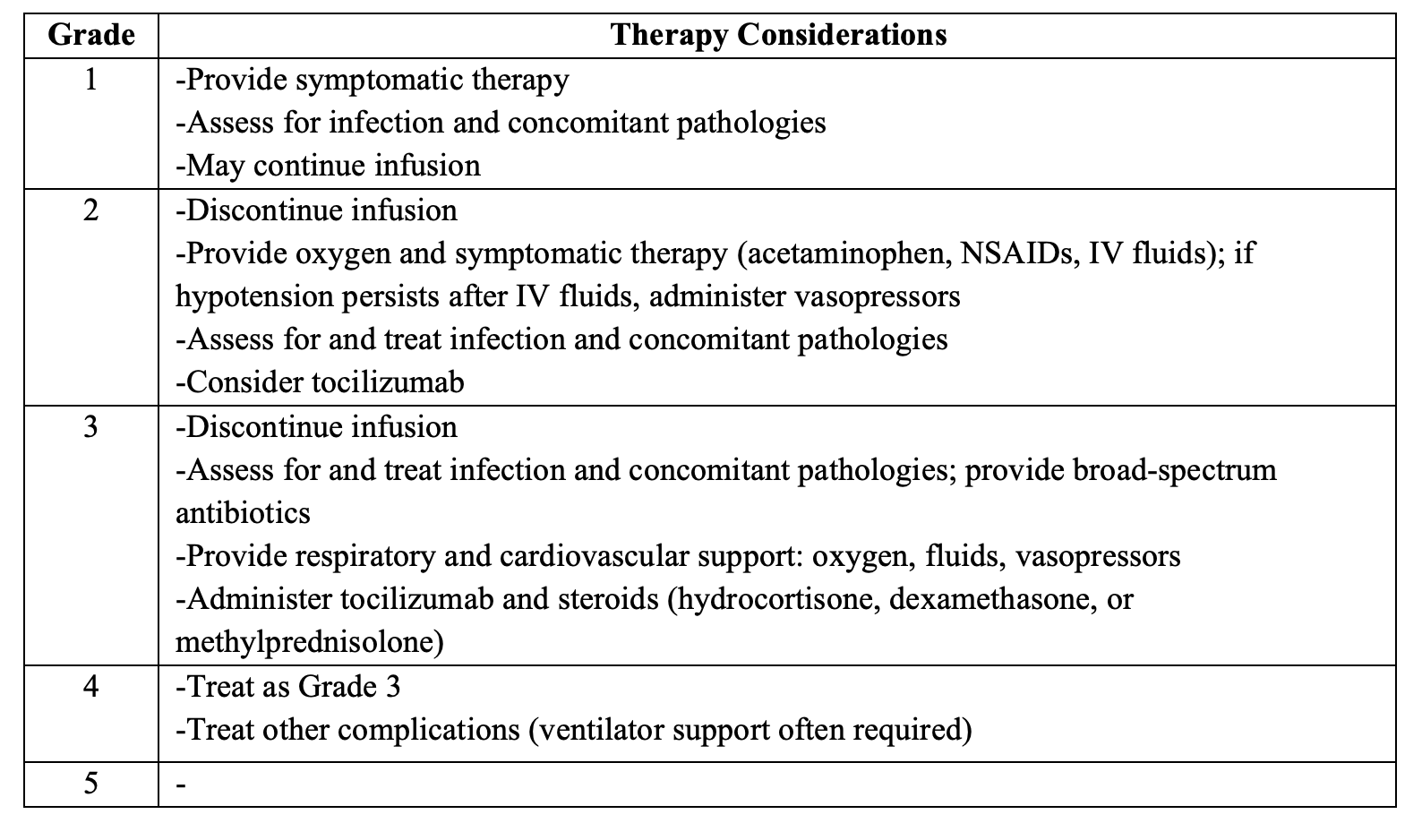
- Grading is based on cardiopulmonary dysfunction and related treatment intervention; the most severe event noted is used to define the grade

- Consider CRS following CAR T-cell therapy in patients with fever, hypotension, hypoxia, tachypnea, tachycardia, dyspnea, myalgias, fatigue, nausea, vomiting, and diarrhea.
- Nonspecific presentation. Patients look like sepsis or septic shock. Must keep sepsis, heart failure, pulmonary embolism (PE), hemophagocytic lymphohistiocytosis, tumor lysis syndrome, and tumor progression on the differential.
ED Evaluation
- History: symptoms (fever, dyspnea, pain, rash), baseline patient function, disease status, burden of illness, immunotherapy type, dose, and schedule.
- Physical examination should focus on the skin, hearts, lungs, abdomen, and neurologic system.
- Testing: Labs and imaging are nonspecific; diagnosis needs to be based on history and end organ injury.
- CBC, electrolytes, magnesium/phos/Ca, renal/liver function, uric acid, coags, blood cultures, CRP.
- ECG, BNP, troponin if cardiopulmonary symptoms present.
- Significant risk of cardiac ischemia and arrhythmia.
- May see leukocytosis, leukopenia, neutropenia, and/or thrombocytopenia may be present due to chemotherapy, the malignancy, or other isues
- Elevated creatinine and liver enzymes are common, as are electrolyte abnormalities, including hypophosphatemia (75%), hypokalemia (56%), and hyponatremia (51%).
- Coagulation panel abnormalities may occur.
- Confirmatory tests are interferon gamma, IL-6, IL-10, and soluble IL-2R alpha levels, but not available in the ED.
- CXR for cardiopulmonary symptoms.
Management:
- Stabilization, evaluation for concomitant pathologies (e.g., sepsis, PE), and providing targeted therapy based upon the CRS grade.
- Involve hematology/oncology early.
- If the patient is critically ill, start with IV fluids, vasopressors, and broad-spectrum antibiotics. These patients will look like sepsis. Respiratory support will be needed for severe cases.
- Targeted therapy is based on CRS severity
- Mild CRS can typically be treated with antipyretics, intravenous fluids, antihistamines, and monitoring.
- Other grades may need steroids plus tocilizumab, but this is best left to the heme/onc and critical care specialist.
- Patients with severe CRS (consisting of some patients with grade 2 CRS and all patients with grades 3-4 CRS) may receive tocilizumab, an IL-6 antagonist, plus a steroid. This combination provides more rapid and complete control compared with either agent alone
- For those with less severe manifestations meeting criteria for grade 2 CRS, tocilizumab may be used alone.
- Options for steroids include hydrocortisone 100 mg every 8 hours, dexamethasone 10 mg up to four times per day, or methylprednisolone 1 mg/kg/day.
- Steroids should be used alone in patients with neurologic findings.
- Other monoclonal antibodies may be used if tocilizumab is not effective.
- All patients should be admitted.
Stay tuned for Part 2, where we cover neurotoxicity, infusion reactions, cytopenias, and cardiac toxicity!
References:
- Long B, Yoo MJ, Brady WJ, Holian A, Sudhir A, Gottlieb M. Chimeric antigen receptor T-cell therapy: An emergency medicine focused review. Am J Emerg Med. 2021 Dec;50:369-375.
- Shimabukuro-Vornhagen A, Gödel P, Subklewe M, et al. Cytokine release syndrome. J Immunother Cancer. 2018 Jun 15;6(1):56.
- Neelapu SS, Tummala S, Kebriaei P, et al. Chimeric antigen receptor Tcell therapy-assessment and management of toxicities. Nat Rev Clin Oncol. 2018;15:47–62.
- Liu D, Zhao J. Cytokine release syndrome: grading, modeling, and new therapy. J Hematol Oncol. 2018 Sep 24;11(1):121.
- Lee DW, Santomasso BD, Locke FL, et al. ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune Effector Cells. Biol Blood Marrow Transplant. 2019 Apr;25(4):625-638.





1 thought on “emDOCs Podcast – Episode 77: CAR T-cell and Cytokine Release Syndrome”
Pingback: LITFL Update 009 • LITFL • Newsletter