
Author: Sreeja Natesan, MD (@sreeja_natesan from @dukeemergency– EM Attending Physician / Assistant Program Director, Duke University Medical Center) // Edited by: Alex Koyfman, MD (@EMHighAK – EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Manpreet Singh, MD (@MPrizzleER – Assistant Professor of Emergency Medicine / Department of Emergency Medicine – Harbor-UCLA Medical Center)
Case: 60 year-old male PMH of Htn, DM, presents to the ED with complaints of generalized weakness and fatigue. His family states you are the third provider he has seen in the last week. He was seen by the primary care doctor for fever and cough 5 days prior and started on Azithromycin for bronchitis and was seen at the Urgent care for fatigue and weakness 1 day prior to presentation where he was treated with IVF. Despite antibiotics and IVF, he reports continued symptoms of generalized weakness. He denies focal weakness, headache or neck stiffness and has an otherwise negative ROS. Vital signs are within normal limits on arrival. PE reveals a normal exam except for the neurologic component which identifies decreased strength in bilateral LE with areflexia. What is your next step?
Background:
How common is GBS?
Guillain-Barré Syndrome (GBS) has an estimated incidence of 1 to 4 per 100,0001 making it the most common cause of acute generalize paralysis since the virtual elimination of poliomyelitis2,3. GBS is a commonly missed diagnosis in the ED which has the potential to progress to significant morbidity1.
How often is it missed?
Diagnosis of early acute GBS is often missed due to the failure to recognize key features essential in the diagnosis of the disease. This is often due to the minimizing the paresthesia, discounting the existence of the complaint, not being vigilant to check deep tendon reflexes, or misinterpreting the complaints of leg, back, or sciatic pain2. A retrospective case series revealed that only 25% of patients were accurately diagnosed with GBS during their first visit with an average of 2 visits need to make the correct diagnosis1.
Definition
Guillain-Barré Syndrome is an inflammatory peripheral neuropathy. Up to 88% of patients affected by GBS have a prodromal infection4. As an aberrant response to a precipitating infection, a primarily lymphocytic T cell mediated and macrophage mediated response results in demyelination, although the exact mechanism is still under investigation2. It is however become clearer that infection can induce antibodies that then cross react with neural antigens which leads to the resultant inflammatory neuropathy5.
It can present with paresthesia, ascending weakness, and areflexia one to six weeks after infectious prodrome4, although there are variable presentations within the 4 subtypes as seen in the box below. Miller-Fischer syndrome accounts for 5% of the cases and includes ataxia and ophthalmoplegia in addition to the areflexia1.

The most common infections are from cytomegalovirus and Campylobacter jejuni1,2. There are 4 main phases of the disease process including:
- Interval between the inciting infection illness and the onset of neuromuscular symptoms
- Progressive weakness lasting less than one month
- Plateau/nadir
- Recovery
The onset of symptoms may vary although there is a rapidly progressive form that can result in quadriplegia and respiratory failure within 48 hours1 and is associated with poorer outcomes5.
Important items in history and physical examination
History pearls
History is crucial in the diagnosis of GBS. The disease process is occur 5-7 days after an infection illness6. Two thirds of cases of GBS follow an infection, typically viral but can include such pathologic agents such as HIV, Epstein Barr virus, and Cytomegalovirus2. Enteritis from Campylobacter jejuni has been identified as an important etiology2, thus a history of fever, crampy abdominal pain with nausea/vomiting/watery-diarrhea or bloody diarrhea would be important to elicit from the patient. Infection with M pneumoniae precedes about 5% of cases of GBS5. In a small population, GBS can also occur in the presence of an underlying systemic disease process such as Hodgkin’s lymphoma, systemic lupus erythematosus, sarcoidosis, or a recently acquired HIV infection2.
Onset of symptoms of weakness within the last 24 hours should raise concerns for GBS, Myasthenia gravis, tick paralysis, stroke, or acute porphyric neuropathy6.
The chief complaint may center on complaints of pain or paresthesia/weakness3. The course can begin with fine paresthesia in the toes or fingertips that is followed within days by leg weakness2. Initially, the weakness may be proximal, distal, or both5 and typically ascends from the lower extremities upward symmetrically. Patients will often complain of weakness that makes it difficult to walk or climb stairs. Pain is a common complaint, described as aching in the large muscle of the upper legs, flanks or back or as bilateral sciatica pain2.
Physical exam pearls
Focus should be aimed at the evaluation for weakness noted as symmetric limb weakness, greatly diminished or absent tendon reflexes, and minimal loss of sensation despite paresthesia2. It is imperative to do a careful neurologic exam including strength and evaluation of reflexes to avoid missing this diagnosis4. The facial nerves are often affected, although to a lesser extent, can also involve the bulbar and ocular motor nerves5. One third of patients may present with bilateral facial weakness2. Severe cases may present with respiratory depression, autonomic dysfunction, or eye movement weakness. Signs of autonomic involvement would include: urine retention, ileus, sinus tachycardia, hypertension, cardiac arrhythmia, and postural hypotension5.

Diagnostic Considerations:
Nerve conduction abnormalities occur earlier and more frequently than the elevation of protein in cerebrospinal fluid due to the reflecting demyelination and thus electrophysiology studies such as electromyography (EMG) are the most sensitive and specific diagnostic tool2 . However, this is usually not feasible to attain in the ED1 raising use of a thorough history, physical exam, and lumbar puncture as the tools to help a clinician correctly make this diagnosis.
Cerebrospinal fluid Studies
Confirmatory workup involves a lumbar puncture (LP) in which the CSF is evaluated for albuminocytologic dissociation without an elevated cell count (high protein (>45) and low WBC count (<10))1. The LP results that is consistent with GBS includes normal opening pressure, few or no cells, and a protein concentration that is elevated2. A raised CSF protein concentration is found in up to 80% of patients although it is important to know that in the first few days of the illness it may be normal5.
Guillain Barré Syndrome (GBS) Diagnostic Criteria

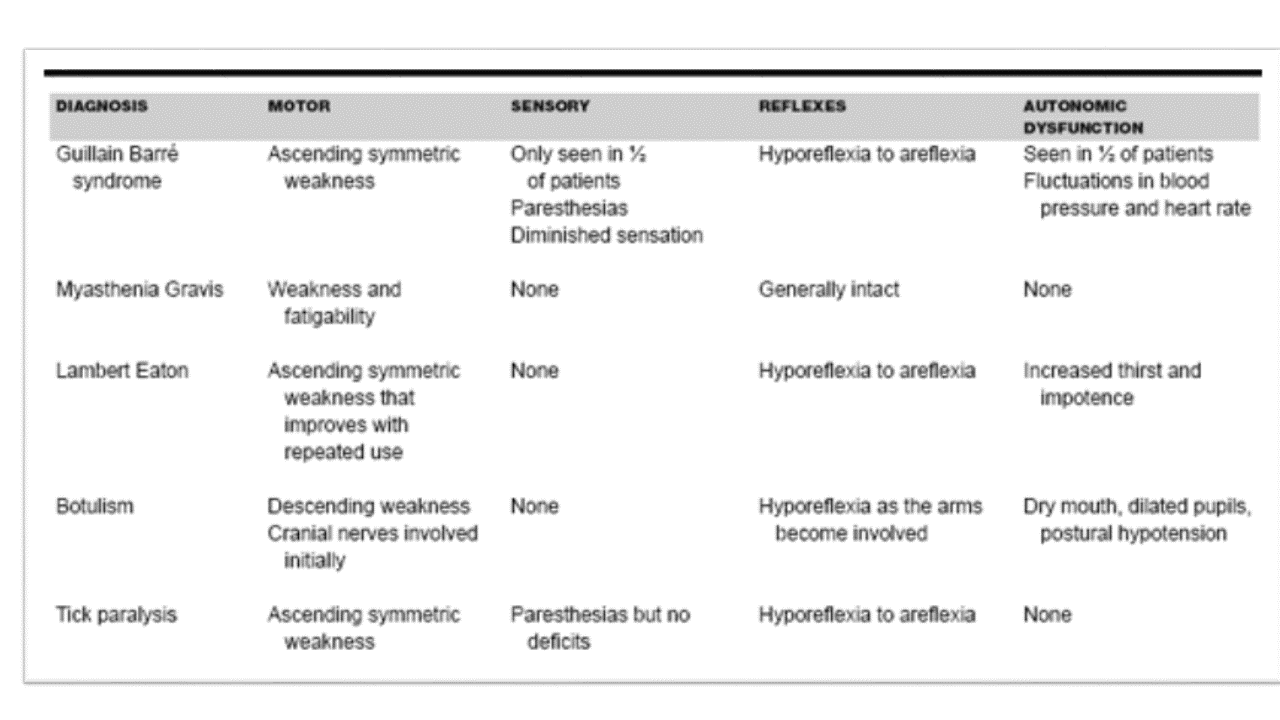
Differential diagnosis of acute flaccid paralysis5

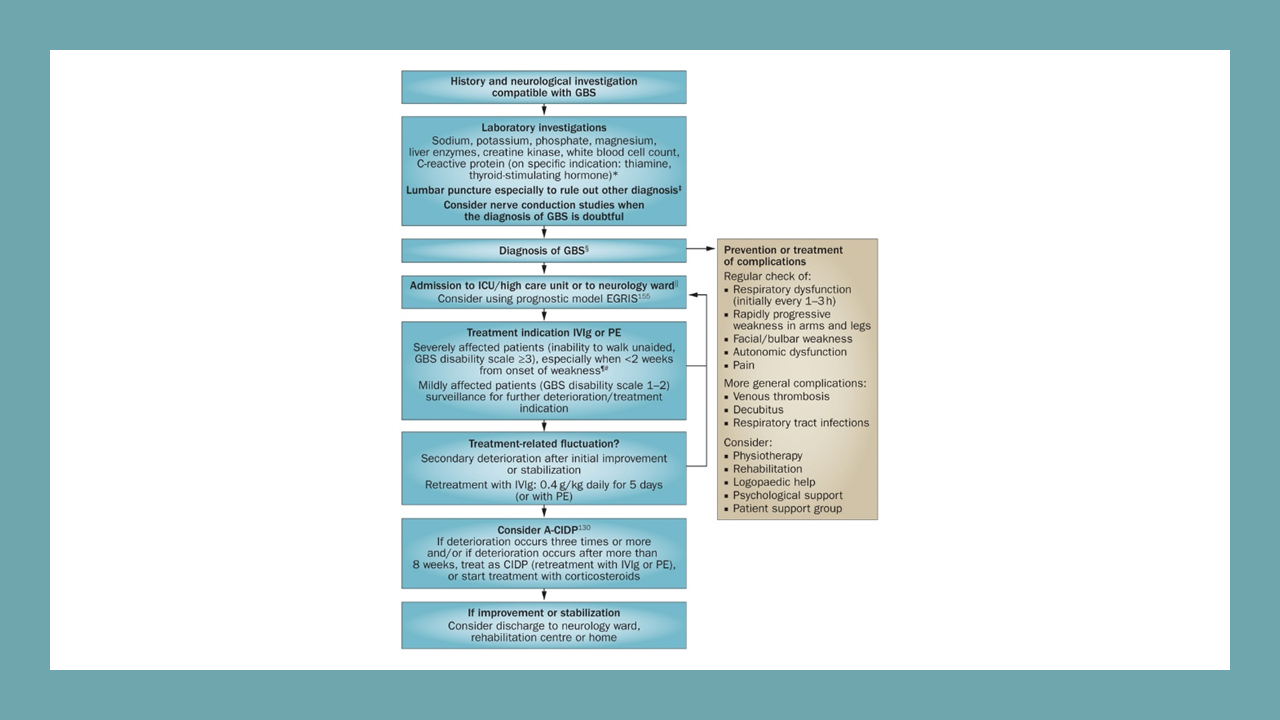
Management
The first priority in any patient arriving to the Emergency department should focus on ABCs and a quick review of life threatening causes of weakness as seen in the following box6.
| Acute Life-threatening Causes of Weakness6 |
| Myasthenia gravis |
| Guillain-Barre Syndrome |
| Botulism |
| Adrenal insufficiency/hypermagnesemia |
| Organophosphate poisoning |
| Carbon monoxide poisoning |
| Hypokalemia |
| Cerebrovascular accident |
| Seizure |
| Spinal cord compression |
| Encephalopathy |
| Sepsis |
Intubation/RSI pearls
Weakness of the respiratory muscles can cause patients with GBS to require artificial ventilation in up to 25% of patients1,5. Regular monitor of vital capacity can be useful in determining if prophylactic intubation is necessary5. Early intubation is recommended for patients for airway protection with guidance using the 20-30-40 rule (given in the following box)6. Other potential indications would be inability to lift head or shoulders, inability cough, rapid onset of symptoms6.
| 20-30-40 Rule for Intubation in GBS |
| Forced vital capacity < 20ml/kg |
| Max inspiratory pressure <30cm H20 |
| Max expiratory pressure <40cm H20 |
Regarding RSI: succinylcholine should be avoided due to significant risk of hyperkalemia, which results due to the upregulation of muscle acetylcholine receptors6,7.
Medication Considerations
Plasma exchange versus immunoglobulin (IVIG) therapy are the mainstay therapy1,4 and are more efficacious when started during the first 2 weeks of symptoms6. However since continued research including randomized controlled trials have showed similar efficacy to plasma exchange, IVIG has replaced plasma exchange in treatment of severe GBS due to convenience5. CSF analysis should be done before initiating IVIG as the implementation of IVIG may cause an aseptic meningitis5. The American Academy of Neurology practice parameter does recommend either plasma exchange or IVIG for treatment of GBS patients who have lost the ability to walk, although best practice is still undecided5. Corticosteroids are no longer considered useful in the therapy for GBS2.
Disposition
Hospitalization for observation for at least several days should occur for almost all patients with Guillain-Barré Syndrome2. Mild cases that include only mildly distal paresthesia or mild limb weakness may not warrant therapy, although it is suggested to wait approximately two weeks before concluding that there will be no further progression2. Intensive Care admission should be considered in patient with cardiovascular dysautonomia or those patient with a vital capacity that is <18ml/kg body weight or is rapidly declining2.
Prognosis
Weakness typically stops advancing in one to four weeks, with a nadir by 2 weeks, eventually reaching a plateau phase by 4 weeks in nearly all cases2,5. A typical patient during this process will become bedridden due to the weakness with distal paresthesia, incomplete bilateral weakness of facial muscles, difficulty swallowing and half of the predicted vital capacity2. There are varying degrees of the severity and identification of this is crucial to ensure the best outcomes. In both adult and children, the severity of the disease at the nadir has been identified as an adverse prognostic factor (expressed as being bed bound or requiring artificial ventilation)5.
Prompt treatment has been associated with good long-term outcomes including an 85% full recovery6. Between 4-15% of patients die despite medical therapy, from largely avoidable complications such as sepsis, adult respiratory distress syndrome, pulmonary embolism, and dysautonomia leading to cardiac arrest2 with some references stating up to 20% being permanently disabled5. Minor residual deficits can be seen in up to 65 percent such as distal numbness or foot drop although this does not impair daily life2. Disabling weakness, imbalance or sensory loss occur in 5 to 10 percent2. Poorer outcomes are seen in patients who had rapid onset of symptoms5. Patients who at the nadir of 2 weeks are still able to walk, are likely to improve with or without treatment with no residual deficit5. Multi-disciplinary rehabilitation is essential in the recovery of GBS patients.
The illness tends to be less severe in children than adult2 with recovery being more rapid and complete5. Also, if this occurs during pregnancy, it typically occurs during the third trimester or post-partum and does not affect the fetus suggesting that the maternal IgG does not cause nerve inflammation or demyelination2.
Pearls and Pitfalls:
- Guillain-Barre Syndrome is a difficult diagnosis to make and an accurate history and physical examination including reflexes and ambulation of the patient can help to identify this life-threatening diagnosis
- LP results will reveal a normal opening pressure, elevated protein level with no cells
- Intubation consideration: remember the 20-30-40 rule and avoid succinylcholine for RSI
- Management options: IVIG or plasmapheresis should be considered in patients with GBS. They should be monitored closely in the hospital for progression.
- Steroids have no role in treatment of GBS.
Case Resolution
The patient was admitted to neurology step down and had progression of his disease resulting in intubation the next morning due to respiratory depression. IVIG was started in the intensive care unit and the patient’s symptoms stabilized. He was eventually extubated and transferred to the floor. He was transitioned to a rehabilitation facility to help with physical therapy and strength training.
References/Further Reading
- Noto, A., & Marcolini, E. (2014). Select Topics in Neurocritical Care. Emergency Medicine Clinics of North America, 32(4), 927-938.
- Ropper A.H.: The Guillain-Barre syndrome. N Engl J Med 1992; 326: pp1130-1136.
- McGillicuddy D.C., Walker O., Shapiro N.I., et al: Guillain-Barre syndrome in the emergency department. Ann Emerg Med 2006; 47: 390-393.
- Sheridan, J. (2010). Atypical Guillain-Barre in the emergency department. West J of Emerg Med, 11(1), 80-82.
- Ganti, L., & Rastogi, V. (2016). Acute Generalized Weakness. Emergency Medicine Clinics of North America, 34(4), 794-809.
- Hughes RAC, Cornblath DR. Guillain-Barre Syndrome. Lancet 2005; 366: 1653-66.
- Roppolo L.P., and Walters K.: Airway management in neurological emergencies. Neurocrit Care 2004; 1: 405-414.





4 thoughts on “Guillain-Barré Syndrome – Third time’s the charm”
Pingback: Guillain-Barré Syndrome – Third time’s the charm – Verpleegkundig specialisten SEH
Pingback: Week 1: Neuro – SAMMC ER Residency Website
Pingback: Weekly Update – 29 March 2021 – NewYork-Presbyterian Emergency Medicine
Pingback: Neuromuscular Disease in Emergency Medicine | EM Cases