
We always work hard, but we may not have time to read through a bunch of journals. It’s time to learn smarter.
Originally published at JournalFeed, a site that provides daily or weekly literature updates.
Follow Dr. Clay Smith at @spoonfedEM, and sign up for email updates here.
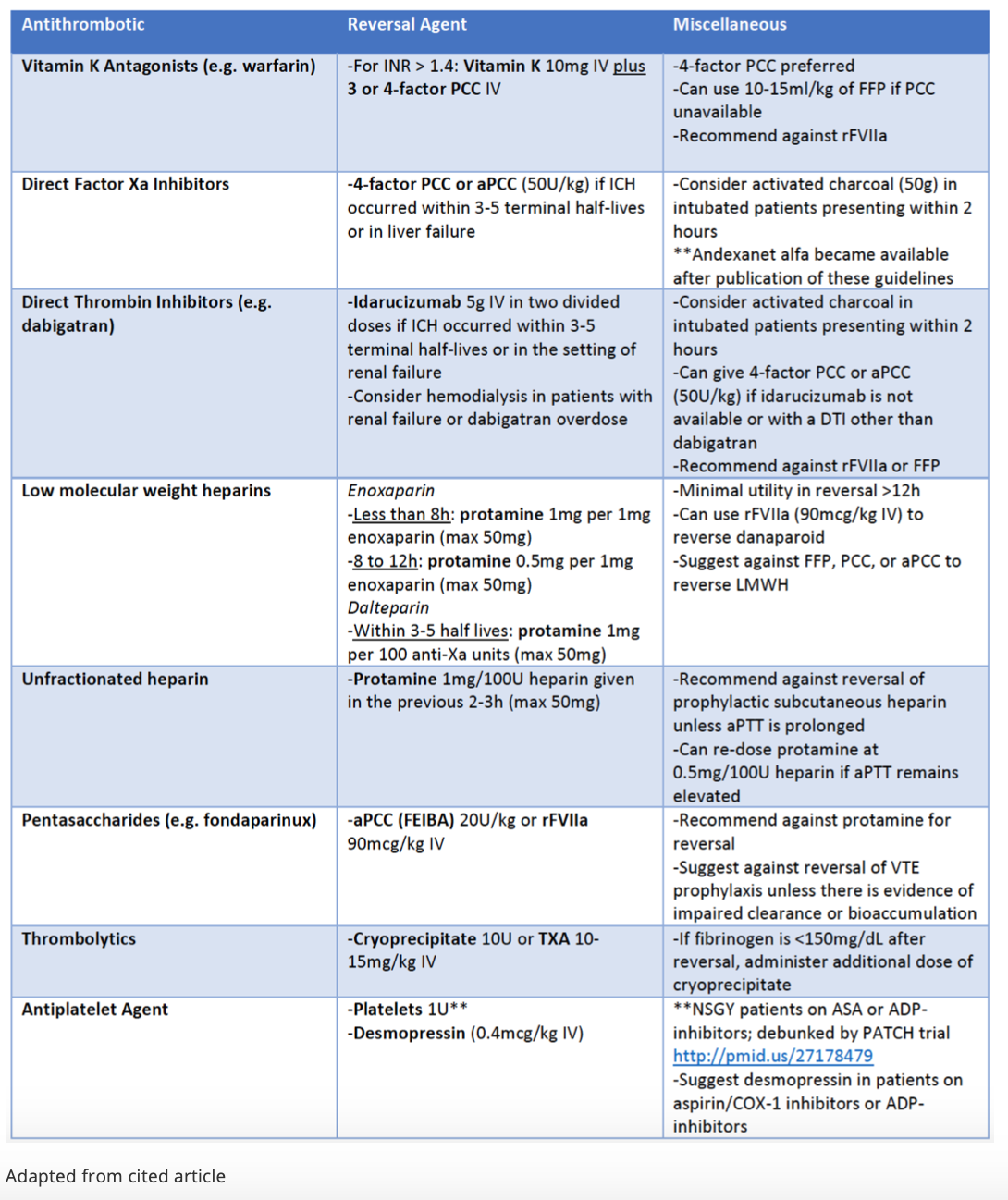
#1: Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage
Spoon Feed
The table below summarizes the recommendations for adult patients on anti-thrombotic agents with intracranial hemorrhage (both spontaneous and traumatic). This will be focused on ED management.
Why does this matter?
Ummm…it’s an anticoagulated head bleed.
Here is your go to reference to stop bleeding in patients with intracranial hemorrhage
Download a PDF copy of this table.
Open in Read by QxMD
#2: HEART – Can We Agree on the Score?
Spoon Feed
Interoperator reliability was high among various paired users of the HEART score. This means people with different levels and types of training were likely to score it the same.
Why does this matter?
The HEART score and HEART Pathway are helpful tools to identify patients with very low risk of acute coronary syndrome (ACS) who may be safely discharged home. But if your HEART score is a 4 and mine is a 3, then that makes a difference in disposition – more testing vs discharge home. Interoperator reliability has been assessed retrospectively in the past. This is a prospective look.
HEARTs beating together
This was a prospective study of paired scorers of patients in the ED with possible ACS: senior doctor/junior doctor or senior nurse/junior nurse. All had a pocket score card guide as a memory aid. They found that in 88 patient/scoring pairs that the intraclass correlation coefficient (ICC) was high overall, 0.91 (that’s excellent, very high agreement). This suggests that the, “HEART Score is reproducible when used by different professional groups and grade of clinician.”
For the individual components, the ICC for troponin and age were 1, which means 100% agreement. ICC for history was 0.41; ECG, 0.64; and risk factors, 0.84. They initially planned to enroll 120 patients but were unable to do so. However, the result was still significant, as reliability was higher than expected. They also used high-sensitivity troponin, which may differ from place to place. History had the lowest interoperator reliability. As this study shows, deciding what is or is not “suspicious” for ACS in the history is tough.
Another Spoonful
Using the HEART Pathway App has helped me, especially when scoring the “History” portion of the HEART score.
This emDocs post looks at potential pitfalls to be aware of when using the HEART pathway.
Source
Do all HEART Scores beat the same: evaluating the interoperator reliability of the HEART Score. Emerg Med J. 2018 Sep 14. pii: emermed-2018-207540. doi: 10.1136/emermed-2018-207540. [Epub ahead of print]
Open in Read by QxMD
#3: Really Scary? Predicting Bad Outcomes in Bronchiolitis
Spoon Feed
Specific emergency department variables are strongly predictive of infants with bronchiolitis requiring escalated care.
Why does this matter?
Bronchiolitis is a common reason for ED visits and hospitalization in infants. ED predictors of escalated care would be helpful for emergency physicians as well as pediatricians evaluating infants with bronchiolitis. Which babies should we not send home? Which ones likely need ICU care?
Hypoxic, grunting, dehydrated babies are a risky bunch
In this study, researchers performed a secondary analysis of retrospective data from the international Pediatric Emergency Research Network. Infants less than 12 months of age with a diagnosis of bronchiolitis were included in the study for a total of 2722 infants. Of these, 261 (9.6%) infants required escalated care, defined as need for hospitalization and need for any of the following: high-flow nasal cannula (HFNC), noninvasive ventilation support, tracheal intubation and ventilation, or management in an ICU setting without airway support. Multivariable analysis showed that the predictors that correlated most with escalated care needs were oxygen saturation <90% (OR 8.92), nasal flaring and/or grunting (OR 3.76), retractions (OR 3.02), apnea (OR 3.01), dehydration (OR 2.13), age under 2 months (OR 2.10), and poor feeding (OR 1.85). A risk score was derived from these factors that varied from 0 to 14 points. This corresponded with an estimated risk for escalated care of 0.9% for a score of 0 to 96.3% for a score of 14. While awareness of these risk factors may help in management and disposition decisions, the clinical utility of this risk score remains untested. Knowing these predictors makes bronchiolitis less SCARY.
Which babies with bronchiolitis NOT to send home:
- Saturation <90%
- Can’t take PO
- Apnea
- Retracting/flaring/grunting
- Younger than 2 months
Source
Predicting Escalated Care in Infants With Bronchiolitis. Pediatrics. 2018 Sep;142(3). pii: e20174253. doi: 10.1542/peds.2017-4253. Epub 2018 Aug 20.
Open in Read by QxMD
#4: Which Is Better – VL or DL?
Spoon Feed
Video laryngoscopy (VL) gets the green light from Academic Emergency Medicine over direct laryngoscopy (DL) – clear benefit, no harm. For every 17 intubations using VL, one less patient will have a failed intubation.
Why does this matter?
The FELLOW, MACMAN, ED-based RCT, and dubious meta-analysis all found that VL did not improve first pass success over DL. Yet a Cochrane review in 2016 found VL had big advantages. AEM summarized that review.
Levitan says don’t choose VL or DL – use one that does both
This was a meta-analysis of 7044 patients in 64 RCTs, only 3 of which were based in the ED. Use of VL vs DL reduced the number of failed intubations. In the original study, the absolute risk of failed airway was 9.4% with DL, 3.5% with VL; ARR = 0.094 – 0.035 = 0.059; 1/ARR = NNT = 17. For every 17 intubations, this means one less failed intubation. That’s a big deal. Authors said the NNT was 14 (not sure why the difference). Odds of an easy view of the glottic opening were 677% greater for VL over DL (OR 6.77, 95%CI 4.17-10.98). Odds of having no glottic view were reduced by 82% with VL (OR 0.18, 95%CI 0.13-0.27). There was heterogeneity among the RCTs, with 9 VL devices used. In subgroup analysis, the Storz C-MAC reduced failed intubation more than other VL devices. They did not find harm associated with VL. The downsides – most intubations were were performed by anesthesiologists in the OR, not the ED, and device use could not be blinded. VL devices excelled especially in patients with known or predicted difficult airway. In a 2015 study, 93% of difficult airways were unanticipated. In the ED, we anticipate 100% of our patients will have a difficult airway. Why would we not give ourselves and our patients every advantage in such a critical procedure?
Another Spoonful
- Again, here is the original Cochrane review this Academic EM summary was based on.
- See Levitan’s take in EP Monthly.
Source
Video Laryngoscopy vs. Direct Laryngoscopy. Acad Emerg Med. 2018 Oct 15. doi: 10.1111/acem.13627. [Epub ahead of print]
Open in Read by QxMD




