
Author: Annahieta Kalantari, DO (@akkalantari, Clinical Associate Professor of Emergency Medicine, Philadelphia College of Osteopathic Medicine, Associate Program Director, Aria Jefferson Health) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
An 80-year-old female is brought to your institution unresponsive after she fell and hit her head. She has a history of nonvalvular atrial fibrillation. Her family is unsure of the exact agent, but knows that she is on a newer anticoagulant. Prior to this event the patient has lived a very active, independent, and vibrant life. You perform standard ATLS stabilization, and ultimately the patient is diagnosed with a subdural hematoma. How will you reverse her if her anticoagulant is dabigatran? Apixaban?
How do we clot?
There are two key components in clot formation. In the first part, platelets interact with vascular subendothelium to form a platelet plug at the site of injury. This requires intact platelets, functional collagen, normal von Willebrand Factor, glycoproteins, and normal fibrinogen. The second part involves the universally loved and memorized coagulation cascade. Here is an abbreviated version:

The intrinsic pathway can be triggered via inflammation, infection, and other cytokines and is measured by the PTT. The extrinsic pathway, measured via PT/INR, is due to some kind of injury or trauma. Both pathways meet at factor X. From there, we continue to the formation of fibrin which is what reinforces the platelet aggregate.
Key Point: Clotting is made up of platelet aggregation and fibrin stabilization. Coagulation factors are the key components in fibrin formation.
Who are the NOACs?
NOACs are the novel oral anticoagulants or non-vitamin K agonist oral anticoagulants and are also known as direct oral anticoagulants (DOACs).
Dabigatran is really dabigatran etexilate. It is a prodrug that is converted to its active form dabigatran. It’s a very strong, competitive, reversible direct inhibitor of thrombin. The drug actually binds to both unbound and fibrin-bound thrombin, locking up the final stages of the coagulation cascade. It’s rapidly absorbed in the GI tract, peaks at about 2 hours, has about a 14-hour half-life, and is approximately 35% protein bound.1
The Xa inhibitors, also known as the xabans, reversibly inhibit Xa halting the coagulation cascade. They are in active form, unlike dabigatran. Depending on the individual agent, they peak between 1-3 hours, with half-life between 8-14 hours depending on a patient’s renal function. They are all fairly protein bound, but rivaroxaban is the highest at about 95%.2
The NOACs have a few advantages over vitamin K antagonists (VKA). They have easier dosing schedules,2 fewer drug interactions,3 and better patient compliance.4 They are just as effective in preventing MI and CVA in nonvalvular atrial fibrillation, with less bleeding risk and a lower overall mortality.5
Because of these advantages, NOACs are emerging in many guidelines. The Chest 2012 guidelines listed NOACs as 1B recommendations for deep vein thrombosis prevention in total hip and total knee arthroplasty.6 Additionally dabigatran was given a 2B recommendation as a first line agent in the treatment of atrial fibrillation to prevent CVA.7 The 2014 AHA guidelines gave a 1B recommendation for NOACs in patients with nonvalvular atrial fibrillation with a prior history of cerebrovascular accidents and a CHADS/VASC score > 2.8 In the 2016 Chest guideline, NOACs are a 2B recommendation for first line use for deep vein thrombosis and pulmonary embolism in patients without cancer. 9
Key Point: The NOACs include dabigatran, a direct thrombin inhibitor, and the xabans, Xa inhibitors. They have a favorable profile when compared to VKAs and are recommended in several clinical guidelines.
How do we test for NOAC activity?
The short answer is that we can’t. With dabigatran, the aPTT can be elevated, but there is no linear relationship in aPTT level and dabigatran activity. For the Xa inhibitors, an elevated INR may suggest the presence of rivaroxaban. Normal coagulation studies are meaningless and do not suggest the absence of NOAC activity.3
Key Point: There are no reliable laboratory tests to assess NOAC activity readily available for emergent use.
How do we reverse dabigatran?
Idarucizumab is considered the go-to agent for reversal of dabigatran. Idarucizumab is a monoclonal antibody fragment that binds dabigatran with an affinity 350x that of thrombin. This blocks dabigatran from binding to thrombin and thrombin-bound fibrin allowing the coagulation cascade to proceed. Idarucizumab comes in premade 2.5 gm vials. The standard dose is 2.5 gm boluses given back-to-back for a total of 5gm. The retail prices is $4200.00 for a 5gm treatment.
The REVERSE-AD study evaluated the efficacy and safety of idarucizumab in the reversal of dabigatran in life threatening bleeds (Group A) and need for reversal for emergent surgery (Group B). The primary endpoint was the percentage of dabigatran reversal based on dilute thrombin time (dTT) and escarin clotting time (ECT). Secondary outcomes were based on clinical outcomes of patients.
The interim REVERSE-AD10 data was released in 2015 with 90 patients enrolled. 100% of patients in group A had achieved laboratory reversal of dabigatran but the median time to reversal was 11.5 hours. As you will recall, the half-life of dabigatran is approximately 14 hours. Because this was a prospective cohort observational study, there was no control group. Whether the 11.4-hour reversal time was due to administration of idarucizumab vs. the half-life of dabigatran was unknown. In group B, 93% of patients achieved normal hemostasis during surgery.
The final data of the REVERSE-AD11 study was published in August 2017. There were just over 500 patients enrolled with 301 in group A and 202 in group B. 95% of the patients enrolled were on dabigatran for atrial fibrillation.
At 4 hours post infusion, 100% pts achieved laboratory reversal of dabigatran. In group A, hemostasis was achieved in 2.5 hours. The median time to start of procedure was 1.6 hours in group B and 93% of the patients achieved normal hemostasis. 30-day mortality in both groups was 13%. 90-day mortality was 18%. Recall that the median age of patients was 78 years old, and 95% of them had a fib. They presented with life threatening bleeds and required emergency surgery. At 30 days, 5% of patients had a thrombotic event and 7% at 90 days. These are the same values reported in prior studies after major surgical procedures and hospitalizations for bleeding.
The major adverse effect was hypersensitivity that occurred in 4 patients. 5.6% had either pre-existing antibodies or developed antibodies to idarucizumab. There were also episodes of delirium, cardiac arrest, and septic shock, but there was no consistent pattern. These were thought to be due to underlying disease processes of the patients.
There are some major limitations to this study. The first is a major conflict of interest. This study was done by Boehringer Ingelheim who also make dabigatran. The second is that this was a prospective cohort study that was not compared to placebo as no one wanted to withhold potential reversal from patients requiring emergent care. Another major limitation is the use of laboratory tests for the primary outcome, rather than patient-centered mortality. Lastly in the group A cohort, data from patients was not included if the bleeding source was not identified which may skew the bleeding cessation time to a more favorable direction.
Key Point: Idarucizumab is the reversal agent of choice for dabigatran. If the specific anticoagulant is unknown, PCC can be used.
How do we reverse the xabans?
There are currently two drugs under study that have not been FDA approved as of 12/1/17.
The first one is andexanet alfa. It is a factor Xa decoy protein. It basically draws the xabans away from Xa allowing the coagulation cascade to proceed.
The ANNEXA-412 trial is an interim analysis that was published in 2016 that measured the reversal of direct and indirect factor Xa inhibitors in patients presenting with acute bleeding. A total of 67 patients were enrolled. Inclusion criteria were 18 years of age or older on apixaban, rivaroxaban, edoxaban, or enoxaparin presenting with life threatening bleed. Coprimary outcomes were percentage of change in anti-factor Xa activity and rate of good/excellent hemostasis at 12 hours after infusion. There were several exclusion criteria: anticipated surgery within 12 hours, intracerebral hemorrhage with GCS <7, intracerebral hemorrhage with volumes > 60mL, anticipated survival of < 1 month, any thrombus within 2 wks, any other reversal agent used within 1 wk, or dabigatran use within 1 wk.
Dosing was varied based on xaban type and last time it was taken. Andexanet alfa was given in bolus form followed by an infusion. The anti-Xa activity displayed in ng/mL sharply dropped immediately after infusion for both rivaroxaban and apixaban. Levels started to increase 2 hours post infusion. In the rivaroxaban group, levels slightly decreased from 4 hrs to 12 hrs. In the apixaban group, anti-Xa activity leveled off after 4 hours.

At 12 hrs, the anti-Xa activity decreased approximately 40% for rivaroxaban and 30% for apixaban. Approximately 79% of the patients achieved good or excellent hemostasis. There was a 5% mortality, and 18% of the patients had a thrombotic event.
Other issues that were not stated in the study include it requires reconstitution, refrigeration, and A LOT of vials to achieved the doses that were evaluated in the study.
The other drug under study is ciraparantag. It’s a small water-soluble molecule that noncovalently binds everything – UFH, LMWH, fondaparinux, and NOACs. It is currently under phase 2 testing with planned phase 3. What we do know from a very small report of a randomized placebo-controlled trial of edoxaban reversal in 80 healthy males is that its onset is about 10 minutes and lasts about 24 hours. There were no thrombotic events reported. The major adverse reaction was flushing.13
Key Point: Andexanet alfa and ciraparantag are two drugs currently under study and show promising results for Xa inhibitor reversal but are not yet FDA approved.
As stated, these 2 drugs are under study and not FDA approved. So, what can we use that is available to reverse the xabans? Basically, 4 factor PCC or activated PCC is the go-to.14
4F PCC, also known as Kcentra, is available as a single-use vial containing coagulation Factors II, VII, IX, X, and antithrombotic Proteins C and S as a lyophilized concentrate.15 FEIBA (Factor eight inhibitor bypassing activity), aka aPCC, is comprised of non-activated factors II, IX, X, and activated factor VII.16 These agents flood the coagulation cascade with factors including prothrombin, which is factor II. Unfortunately, the data supporting 4FPCC and aPCC are limited. Much of the data is a based on rodent and other animal studies.17 Human trials were done on healthy individuals.18
Theoretically fresh frozen plasma (FFP) can be used, and if it is all you have, you should use it. The main issue is that it will take approximately 2 liters of FFP to provide the factors available in PCC.3
Tranexamic acid (TXA) is another option, as it inhibits fibrinolysis by inhibiting the binding of plasma to fibrin. In other words, whatever clot your body has formed cannot be broken down in the presence of TXA. There is a paucity of data addressing the use of TXA in anticoagulated patients.
We learned from CRASH 2 that trauma patients had a better mortality if TXA was given within 1 hour, but there was a very small cohort who had traumatic brain injury and the anticoagulation was not discussed. So, the data cannot be directly extrapolated.19
There was a double blind randomized trial published in BMC EM Med that compared TXA vs. placebo in traumatic brain injury. 238 patients were enrolled, and no statistical difference was identified between the 2 groups.20
Hemodialysis will work for dabigatran (not xabans). Recall that the xabans are highly protein bound. Additionally, they are hepatically and renally cleared. Only about 35% of dabigatran is protein bound, and it is predominantly renally cleared. Even though hemodialysis is possible for dabigatran, it takes an extended amount of time to set patients up for dialysis. Additionally, they require a large catheter in an anticoagulated state. Most of these case reports came out prior to the availability of idarucizumab.21
Charcoal is useful for xaban reversal IF the person is a good candidate for charcoal, i.e., intubated or awake enough to swallow without risk of aspiration AND the last dose was taken within 2 hours.14 This is in the neurocritical care recommendations as well.
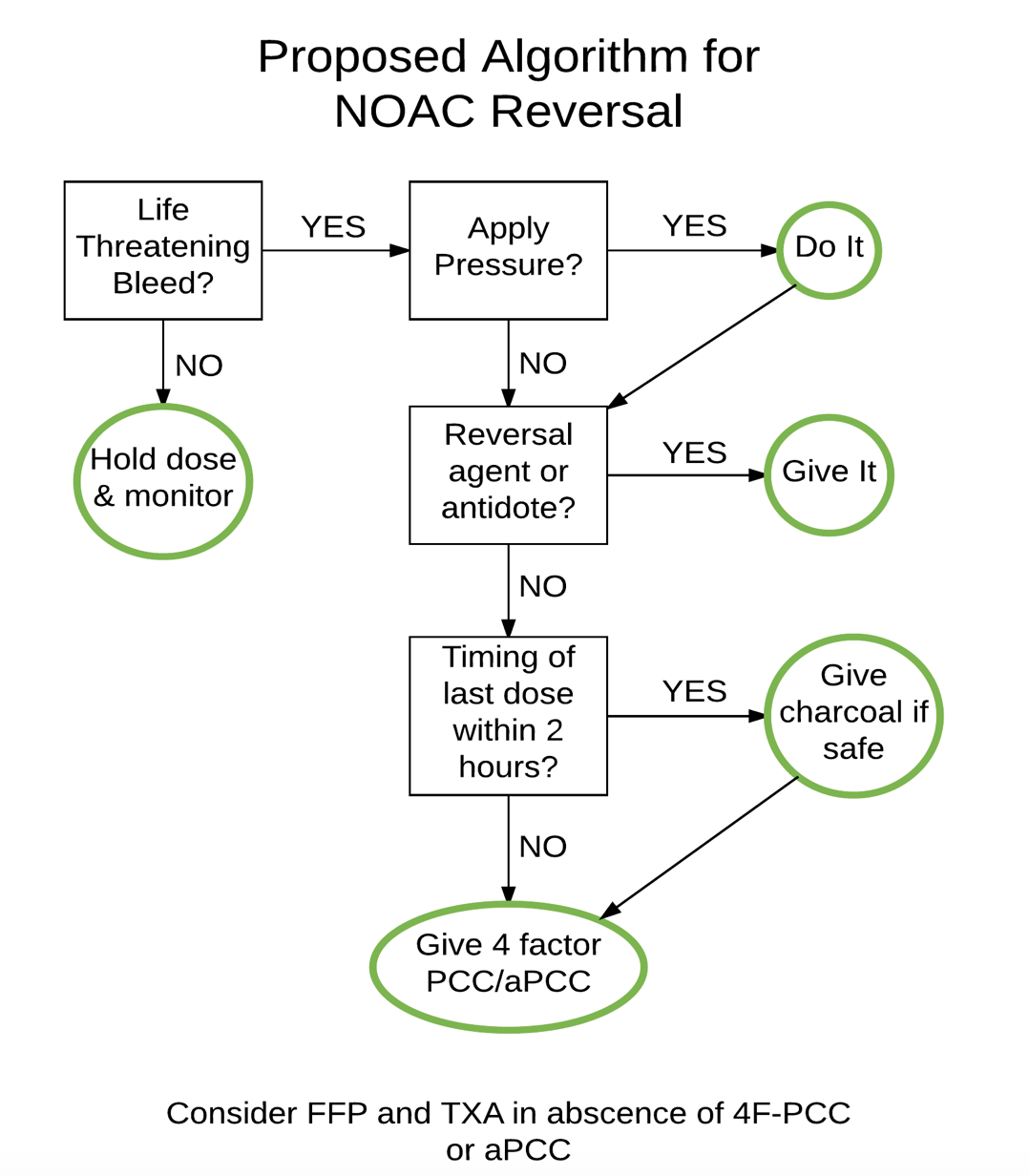
Below is a proposed algorithm for NOAC reversal:
Summary
NOACs have a favorable clinical profile when compared to VKAs and are easier to use. They have no reliable laboratory testing available to measure activity. If the clinician is unable to determine which agent the patient is taking, PCC can be used. Dabigatran can be reversed with idarucizumab. Xabans can be reversed with PCC. If PCC is not available, FFP and TXA should be utilized. Charcoal can be used in select patients who present within 2 hours of dosing.
References / Further Reading
- Hankey GJ, Eikelboom JW. Dabigatran etexilate: a new oral thrombin inhibitor. Circulation. 2011;123(13):1436-1450.
- Liotta EM, Levasseur-Franklin KE, Naidech AM. Reversal of the novel oral anticoagulants dabigatran, rivoraxaban, and apixaban. Curr Opin Crit Care. 2015;21(2):127-133.
- Christos S, Naples R. Anticoagulation Reversal and Treatment Strategies in Major Bleeding: Update 2016. West J Emerg Med. 2016;17(3):264-270.
- Barnes GD, Lucas E, Alexander GC, Goldberger ZD. National Trends in Ambulatory Oral Anticoagulant Use. Am J Med. 2015;128(12):1300-1305 e1302.
- Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962.
- Guyatt GH, Akl EA, Crowther M, et al. Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):7S-47S.
- You JJ, Singer DE, Howard PA, et al. Antithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e531S-e575S.
- January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64(21):e1-76.
- Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-352.
- Pollack CV, Jr., Reilly PA, Eikelboom J, et al. Idarucizumab for Dabigatran Reversal. N Engl J Med. 2015;373(6):511-520.
- Pollack CV, Jr., Reilly PA, van Ryn J, et al. Idarucizumab for Dabigatran Reversal – Full Cohort Analysis. N Engl J Med. 2017;377(5):431-441.
- Connolly SJ, Milling TJ, Jr., Eikelboom JW, et al. Andexanet Alfa for Acute Major Bleeding Associated with Factor Xa Inhibitors. N Engl J Med. 2016;375(12):1131-1141.
- Ansell JE, Bakhru SH, Laulicht BE, et al. Use of PER977 to reverse the anticoagulant effect of edoxaban. N Engl J Med. 2014;371(22):2141-2142.
- Frontera JA, Lewin JJ, 3rd, Rabinstein AA, et al. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocrit Care. 2016;24(1):6-46.
- fda.gov. Prothrombin Complex Concentrate labeling. https://www.fda.gov/ucm/groups/fdagov-public/@fdagov-bio-gen/documents/document/ucm350239.pdf. Accessed 11/30/2017.
- fda.gov. Factor Eight Inhibitor Bypassing Activity label. https://www.fda.gov/downloads/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/LicensedProductsBLAs/FractionatedPlasmaProducts/UCM221749.pdf. Accessed 11/30/17.
- Zhou W, Schwarting S, Illanes S, et al. Hemostatic therapy in experimental intracerebral hemorrhage associated with the direct thrombin inhibitor dabigatran. Stroke. 2011;42(12):3594-3599.
- Levi M, Moore KT, Castillejos CF, et al. Comparison of three-factor and four-factor prothrombin complex concentrates regarding reversal of the anticoagulant effects of rivaroxaban in healthy volunteers. J Thromb Haemost. 2014;12(9):1428-1436.
- collaborators C-t, Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376(9734):23-32.
- Yutthakasemsunt S, Kittiwatanagul W, Piyavechvirat P, Thinkamrop B, Phuenpathom N, Lumbiganon P. Tranexamic acid for patients with traumatic brain injury: a randomized, double-blinded, placebo-controlled trial. BMC Emerg Med. 2013;13:20.
- Chiew AL, Khamoudes D, Chan BS. Use of continuous veno-venous haemodiafiltration therapy in dabigatran overdose. Clin Toxicol (Phila). 2014;52(4):283-287.





2 thoughts on “Reversing NOACs – Updates for Emergency Physicians”
Pingback: January FOAMed - FRCEM Success
Pingback: emDOCs.net – Emergency Medicine EducationEMin5: NOACs - Novel Oral Anticoagulants - emDOCs.net - Emergency Medicine Education