
Author: Kreshmeh Khosrowani, MD (EM Resident Physician); Curren Smith, MD (EM Resident Physician); and Cam Mosley, MD (EM Attending Physician) (Louisiana State University Health Sciences Center-New Orleans School of Medicine, Emergency Medicine Residency Program, Baton Rouge Campus, Baton Rouge, Louisiana) // Reviewed by: Skyler Lentz, MD (@skylerlentz); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case
A 66-year-old woman with a past medical history of hypertension, diabetes, and hyperlipidemia presents to the emergency department with complaints of general malaise, fever, and a rash that has developed over the course of hours. The rash is macular and involves mucous membranes. She states she is beginning to have difficulty swallowing because of the pain. When mechanical pressure is applied to the edge of the blisters or on normal skin further ulceration results. She reports she is currently completing a course of antibiotics for a UTI she was diagnosed with at an urgent care last week. Blood pressure is 167/89, HR is 104, RR is 14, temperature is 98.9°F.
SJS/TEN
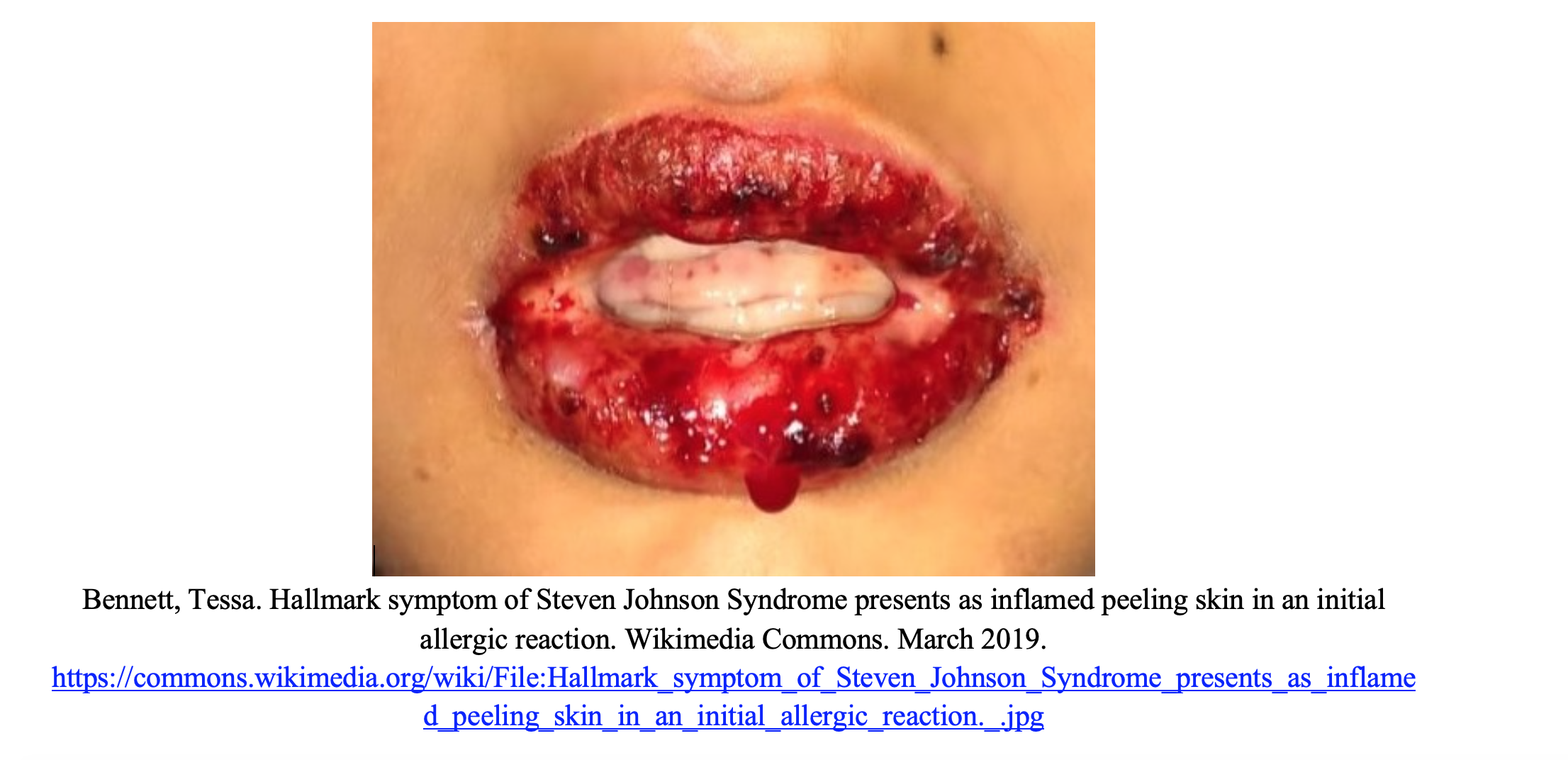
Stevens-Johnson syndrome (SJS) is a life-threatening skin condition that exists on a spectrum of severity. It begins with a prodrome of high-grade fever, flu like symptoms, skin tenderness and blistering. The characteristic rash is commonly described as a confluent erythematous macular rash with purpuric centers that blister and peel. SJS involves at least 10% body surface area (BSA); toxic epidermal necrolysis (TEN) is diagnosed if the rash involves at least 30% BSA. The hallmark mucosal involvement can result in symptoms such as conjunctival itching and pain with swallowing. The rash typically begins on the torso and face and spreads to the rest of the body, usually sparing the palms and soles. This rash is importantly Nikolsky sign positive, where lateral pressure on intact skin causes shedding of the epidermis (1). This is an important distinguishing feature in differentiating SJS/TEN from the other life-threatening rashes discusses later. Of these patients, 70 to 100% have mucosal involvement and up to 80% have ocular involvement presenting with conjunctivitis and discharge (2). Given this fact, it is important to perform a thorough ocular and gynecologic exam.
Risk factors for developing SJS/TEN include patients with active cancer, HIV, women, and taking many medications. The common medication offenders include trimethoprim-sulfamethoxazole, phenobarbital, carbamazepine, lamotrigine, acetaminophen, and chemotherapeutic agents. Penicillins are cited as the most common antibiotic agent to cause SJS/TEN. It is unclear if this is due to how frequently penicillins are prescribed or if the antibiotic was being used to treat an early skin manifestation of SJS as a bacterial infection (3). Therefore, a careful history and timeline should be taken to assess the true trigger.
The mainstay of SJS/TEN treatment is supportive care. First, stop the offending agent. Local wound care, pain control, and IV fluids should be continued through the course of the illness, much like you would treat a burn patient (3,4). A retrospective analysis in 2010 recommended an initial IV fluid volume of 2 ml/kg body weight multiplied by the % body surface area of epidermal detachment in the first 24 hours (5). Have a high clinical suspicion for secondary infections which are most commonly due to S. aureus and Pseudomonas aeruginosa. Although prophylactic antibiotics are not recommended, skin cultures can help guide therapy (6). Studies have shown that there unfortunately was no survival benefit to those treated with systemic corticosteroids when compared to those treated with usual care (7). A useful decision tool in determining the clinical setting best suited for management of your patient is the SCORTEN (seen below) scale which can assess severity of disease; those with a score greater than equal to 2 are recommended for ICU or Burn center admission (8).

As SJS/TEN has a broad range of presentations and a potentially high mortality rate, it is important to distinguish from other rashes which present similarly. In fact, when the term TEN was first suggested in 1956, the paper included patients with what have now been differentiated into fixed drug eruptions and staphylococcal scalded skin syndrome (9). Below, we discuss several SJS/TEN mimics which have varying prognoses, causes, and management pathways.
Acute Generalized Exanthematous Pustulosis
Acute Generalized Exanthematous Pustulosis (AGEP) is an uncommon yet severe skin reaction that is often confused with SJS/TEN. It is a drug reaction presenting with non-follicular, sterile pustules on an erythematous and edematous base. It is more common on flexural surfaces and is often seen first in intertriginous areas that spread to the trunk. It usually develops quickly and presents within 24 to 48 hours of starting a medication, unlike SJS which can start days to weeks after being on a medication. Oral mucosal involvement is seen in 25%, opposed to involving the majority of those with SJS (10). Many medications can cause this reaction, notably penicillins, quinolones, sulfonamides, and hydroxychloroquine. Fever, leukocytosis, elevation of acute phase reactants, and eosinophilia are often seen. AGEP is often a clinical diagnosis but biopsy can confirm. Additionally, after resolution, a patch test may be helpful in determining the causative agent. Conveniently, the management is very similar to SJS/TEN — primarily consisting of discontinuing the offending agent and supportive care which usually leads to resolution of the rash within 2 weeks. Topical steroids are useful, but again systemic steroids have no clear benefit (11).

Erythema Multiforme
Erythema multiforme (EM) is an immune-mediated condition that presents with distinctive target lesions with or without mucosal involvement. The target lesions are classic but the rash has a varied presentation that evolves over the course of the disease. A significant distinction is that the lesions of EM tend to be papular as opposed to the atypical target lesions of SJS which tend to be macular in nature. When these lesions affect mucosal areas, it is typically called erythema multiforme major. When there is little to no mucosal involvement it can be described as erythema multiforme minor. The lesions typically develop over 3 to 5 days and resolve within 2 weeks. There are a variety of risk factors that contribute to the development of EM including but not limited to infections, medication, malignancy, and autoimmune disease. However, infections account for approximately 90% of cases with HSV being most common in adults and mycoplasma in children (12).
Treatment of erythema multiforme is typically symptomatic care such as topical steroids and antihistamines. If there is mucosal involvement IV or oral steroids should be considered. Severe mucous membrane involvement such as with multiforme major may require admission and an ophthalmology consult should be considered if there is ocular involvement. It is important to note that treating an underlying, causative infection does not affect the severity or the length of EM (13).

DRESS
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) as hinted by the name, is another severe drug induced reaction that may be difficult to differentiate. This syndrome presents with fever, eosinophilia or elevation in atypical lymphocytes, lymphadenopathy, facial edema, and generalized malaise. This rash usually does not present for 2 to 8 weeks after drug exposure and may continue or even worsen after withdrawal of the causative agent. Include a hepatic panel when checking labs as there is usually organ involvement; most often the liver, lungs or the kidneys. Some of the most common drugs to cause DRESS include aromatic anticonvulsants (e.g. phenytoin, carbamazepine, and phenobarbital), sulfonamides, allopurinol, and vancomycin (14). DRESS usually presents with a morbilliform rash starting from the trunk and upper extremities. The rash becomes edematous causing periorbital edema in the face. It can take many forms and presents with pustules, folliculitis, or scaling or even a rare form with mucosal involvement. Therefore, it can be very difficult to diagnose and differentiate from other rashes and requires a high index of suspicion. Treatment entails topical steroids. Systemic steroids with a long taper over 6 to 8 weeks are indicated for patients with systemic signs such as hepatitis, pleurisy, pneumonia, and kidney injury. For refractory cases, IVIG and plasmapheresis have been used (15).
Pemphigus Vulgaris
Pemphigus vulgaris is a chronic autoimmune disease that is characterized by acantholysis. Destruction of the desmosomes in the epidermis results in loss of keratinocyte to keratinocyte adhesion resulting in painful blisters. These blisters are Nikolsky sign positive. Important distinctions of this rash from others we have discussed is that pruritis is typically absent and there is almost always mucosal involvement, primarily of the buccal mucosa. Risk factors include UV light and medications. Certain thiol drugs, such as penicillamine and captopril, are the most common causative agents (16). Systemic glucocorticoids are the treatment of choice and are responsible for rapid control of this disease. There are also emerging studies researching the use of rituximab, a monoclonal antibody or combinations of nonsteroidal systemic immunomodulatory medications, such as azathioprine or mycophenolate as an adjunct to glucocorticoids with positive outcomes. The use of these adjuncts reduces the amount of steroids necessary and therefore results in less adverse events (17). For severe refractory cases, IVIG may be beneficial as well. In these cases, consult a rheumatologist or dermatologist.
Meningococcemia
One of the first symptoms of meningitis to present is a classical rash that can progress from nonspecific to petechial to hemorrhagic in a matter of hours. The rash begins as 1-2 mm non-blanching petechiae on the trunk and lower extremities. Approximately 50% of patients with meningococcemia will have petechiae present. The degree of thrombocytopenia can be estimated by the presence of these petechiae and thus heighten concern of potential bleeding complications (e.g. risk of LP) secondary to DIC (18). These petechiae can then coalesce into larger purpura. Purpura fulminans is a severe complication that can occur in approximately 15-25% of those with diagnosed meningococcemia. It is characterized by the acute onset of cutaneous hemorrhage, DIC and vascular thrombosis. Bullae and vesicles form that can eventually lead to gangrenous necrosis (19).
Unlike many of the rashes we have discussed thus far, the meningococcemia rash is a symptom of a much larger disease process rather than the disease itself. Treatment of meningococcemia can be found at this emDocs post..
SSSS
Staphylococcal Scalded Skin Syndrome is a potentially deadly skin condition caused by a bacterial toxin from Staphylococcus aureus which undergoes hematogenous spread from the skin. It presents with erythematous painful skin that starts primarily in high friction areas such as skin folds. Flaccid bullae, desquamation, and a positive Nikolsky sign characterize the rash. Importantly, unlike SJS/TEN, there is no mucosal involvement and the rash is more superficial. This rash most often affects infants and children and may present early with irritability and poor oral intake (20). If seen in adults, the mortality rate is high, often up to 60% due to the high burden of infection, whereas the mortality rate in infants is 5%. Treatment is supportive with antibiotics that cover Staph infections. Nafcillin, oxacillin, and vancomycin are common options as most bacteria causing SSSS are resistant to penicillin. Steroids are contraindicated due to immunosuppression (21).
Erythroderma
Erythroderma, also called exfoliative dermatitis, is a rare rash identified by widespread scaling that covers most of the skin surfaces. It is most often seen in the elderly male population. Many causes can incite the rash, including underlying skin conditions, drug reactions, HIV and cutaneous T cell lymphoma (22). The skin is red, warm, pruritic and painful. The patient is often shivering due to heat loss from cutaneous vasodilation. There may be other exam findings that correlate with the underlying cause such as nail changes with psoriasis; lymphadenopathy and splenomegaly may be seen in T cell lymphomas. The rash has a quick onset if caused by medications, while it can take longer to develop when due to other etiologies. Treatment is discontinuing potential medication causes, supportive care, and topical steroids (22,23).

Key points
1) Take a thorough history. Identifying any new medication exposures over the past several months is valuable information.
2) The Nikolsky sign (skin sloughing with lateral pressure) and presence of mucosal involvement can be important differentiating factors in identifying critical rashes – SJS/TEN, pemphigus vulgaris and SSSS are Nikolsky positive.
3) Treatment Breakdown:
- SJS/TEN: supportive care, treat like any other burn
- AGEP: supportive care, +/- topical steroids
- EM: supportive care, consider IV or PO steroids if major
- DRESS: topical steroids, systemic steroids if solid organ involvement
- Pemphigus vulgaris: systemic glucocorticoids + nonsteroidal systemic immunomodulatory medications
- Meningococcemia: antibiotics
- SSSS: antibiotics
- Erythroderma: supportive care, topical steroids
References/Further Reading
- Mockenhaupt M. The current understanding of Stevens-Johnson syndrome and toxic epidermal necrolysis. Expert Rev Clin Immunol. 2011;7(6):803-13.
- Schwartz RA, Mcdonough PH, Lee BW. Toxic epidermal necrolysis: Part I. Introduction, history, classification, clinical features, systemic manifestations, etiology, and immunopathogenesis. J Am Acad Dermatol. 2013;69(2):173.e1-13.
- Fakoya AOJ, Omenyi P, Anthony P, et al. Stevens – Johnson Syndrome and Toxic Epidermal Necrolysis; Extensive Review of Reports of Drug-Induced Etiologies, and Possible Therapeutic Modalities. Open Access Maced J Med Sci. 2018;6(4):730-738.
- Stern RS, Divito SJ. Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Associations, Outcomes, and Pathobiology-Thirty Years of Progress but Still Much to Be Done. J Invest Dermatol. 2017;137(5):1004-1008.
- Shiga S, Cartotto R. What are the fluid requirements in toxic epidermal necrolysis? J Burn Care Res. 2010;31(1):100-4.
- De prost N, Ingen-housz-oro S, Duong Ta, et al. Bacteremia in Stevens-Johnson syndrome and toxic epidermal necrolysis: epidemiology, risk factors, and predictive value of skin cultures. Medicine (Baltimore). 2010;89(1):28-36.
- Roujeau JC, Bastuji-garin S. Systematic review of treatments for Stevens-Johnson syndrome and toxic epidermal necrolysis using the SCORTEN score as a tool for evaluating mortality. Ther Adv Drug Saf. 2011;2(3):87-94.
- Bastuji-garin S, Fouchard N, Bertocchi M, Roujeau JC, Revuz J, Wolkenstein P. SCORTEN: a severity-of-illness score for toxic epidermal necrolysis. J Invest Dermatol. 2000;115(2):149-53.
- Weinkle A, Pettit C, Jani A, et al. Distinguishing Stevens-Johnson syndrome/toxic epidermal necrolysis from clinical mimickers during inpatient dermatologic consultation—A retrospective chart review. Journal of the American Academy of Dermatology. 2019;81(3):749-757.
- Chu C-Y. Acute Generalized Exanthematous Pustulosis (AGEP). (Mockenhaupt M, ed.). Waltham, MA: UpToDate; 2019.
- Feldmeyer L, Heidemeyer K, Yawalkar N. Acute Generalized Exanthematous Pustulosis: Pathogenesis, Genetic Background, Clinical Variants and Therapy. Int J Mol Sci. 2016;17(8)
- Huff JC, Weston WL, Tonnesen MG. Erythema multiforme: a critical review of characteristics, diagnostic criteria, and causes. J Am Acad Dermatol. 1983;8(6):763-75.
- Sokumbi O, Wetter DA. Clinical features, diagnosis, and treatment of erythema multiforme: a review for the practicing dermatologist. Int J Dermatol. 2012;51(8):889-902.
- Taghvaye Masoumi H, Hadjibabaie M, Zarif YM, Arasteh O. Exacerbation of allopurinol-induced drug reaction with eosinophilia and systemic symptoms by teicoplanin: A case report. Journal of Clinical Pharmacy & Therapeutics. 2017;42(5):642-645.
- Criado PR, Criado RF, Avancini JM, Santi CG. Drug reaction with Eosinophilia and Systemic Symptoms (DRESS) / Drug-induced Hypersensitivity Syndrome (DIHS): a review of current concepts. An Bras Dermatol. 2012;87(3):435-49.
- Brenner S, Bialy-golan A, Ruocco V. Drug-induced pemphigus. Clin Dermatol. 1998;16(3):393-7.
- Joly P, Maho-vaillant M, Prost-squarcioni C, et al. First-line rituximab combined with short-term prednisone versus prednisone alone for the treatment of pemphigus (Ritux 3): a prospective, multicentre, parallel-group, open-label randomised trial. Lancet. 2017;389(10083):2031-2040.
- Algren JT, Lal S, Cutliff SA, Richman BJ. Predictors of outcome in acute meningococcal infection in children. Crit Care Med. 1993;21(3):447-52.
- Darmstadt GL. Acute infectious purpura fulminans: pathogenesis and medical management. Pediatr Dermatol. 1998;15(3):169-83.
- Leung AKC, Barankin B, Leong KF. Staphylococcal-scalded skin syndrome: evaluation, diagnosis, and management. World J Pediatr. 2018;14(2):116-120.
- Jordan KS. Staphylococcal Scalded Skin Syndrome: A Pediatric Dermatological Emergency. Adv Emerg Nurs J. 2019;41(2):129-134.
- Aqil N, Nassiri A, Baybay H, Douhi Z, Elloudi S, Mernissi FZ. Erythroderma: A clinical and etiological study of 92 patients. Our Dermatology Online / Nasza Dermatologia Online. 2019;10(1):1-6.
- Grock A, Declerck B, Herbert M, Jhun P. Erythroderma: Not Your Everyday Sunburn. Ann Emerg Med. 2017;69(3):294-296.





1 thought on “Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Mimics – Differential Diagnosis and Initial Management”
Pingback: Quiz 64, February 28th, 2020