Author: Jennifer Robertson, MD, MSEd (Assistant Professor, Emory University, Atlanta GA) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
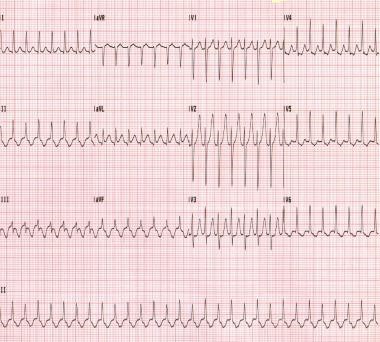
Case 1: A 37 yo G1P0 female at approximately 17 weeks gestational age presents to the emergency department (ED) with a chief complaint of a racing heart. She denies any past medical history. Her heart rate is 180 beats per minute (bpm) but otherwise her vital signs are within normal limits. She denies chest pain. Her electrocardiogram (EKG) is shown below:
http://emedicine.medscape.com/article/156670-overview
Case 2: A 21 year old G1P0 female at approximately 16 weeks gestational age presents with a chief complaint of syncope. She arrives to the ED with a complaint of lightheadedness but is alert and oriented and able to converse. She does complain of some mild chest pain. Her heart rate is 160 bpm and her blood pressure is 85/60 mmHg. Her other vital signs are within normal limits.

http://lifeinthefastlane.com/ecg-library/rvo/
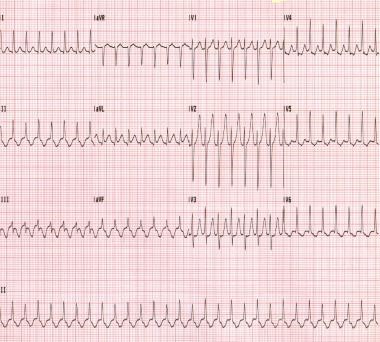
Case 3: A 40-year-old G4P3 female at approximately 12 weeks gestational age presents after feeling palpitations for the last several days. She denies chest pain, syncope or shortness of breath. She denies any past medical history and denies taking any medications. Her initial heart rate is 165 bpm (irregular) and her blood pressure is 130/80 mmHg. Her EKG is shown as follows:

http://misc.medscape.com/pi/iphone/medscapeapp/html/A156670-business.html
Introduction
Compared to the non-pregnant population, cardiac arrhythmias are rare in pregnancy, with an incidence of about 1.2 per 1000 pregnant women (1). However, they can negatively affect the health of both the mother and child, especially if they lead to hypoperfusion. Thus, emergently addressing them is important. Additionally, it is important to understand that the management of arrhythmias in pregnancy may vary considerably from the non-pregnant patient due to the potential effects of anti-arrhythmic medications and electrical therapy with sedation (2). Thus, this is a brief review of the evaluation and management of the pregnant patient who may present to the emergency department with a tachy-arrhythmia. Pathologic bradycardia is very rare in pregnancy and will not be covered in this current article (3).
General Physiology: Brief Review
Arrhythmias in pregnancy can be due to a number of causes including congenital heart disease, channelopathies, and other structural heart diseases (3). Examples include Wolff Parkinson White Disease, pulmonary hypertension, Marfan syndrome with a dilated aortic root, arrhythmogenic right ventricular dysplasia, and even coronary artery disease (4,5). They can also be due to reasons that are commonly seen in non-pregnant patients such as idiopathic, infection/sepsis, electrolyte abnormalities, medications, toxins, pulmonary emboli and hyperthyroidism (2,6,7). Similar the general population, these causes should also be considered when evaluating for the underlying cause of the arrhythmia (6, 7).
For some pregnant patients, an arrhythmia may be recurrent from a previously diagnosed cardiac disease or a first-time presentation. Due to the many physiologic changes and stresses on the cardiovascular system, pregnancy can provoke arrhythmias in some women with undiagnosed structural heart disease (s) (4). In addition, in women with known tachy-arrhythmias, pregnancy may cause an increased risk of recurrence or worsening of the dysrhythmia (3, 7). A thorough family and personal history of structural heart disease should be obtained in addition to a family history of sudden or unexplained death (3).
Palpitations are usually benign and life threatening arrhythmias are rare in pregnant patients (1, 3, 7, 8), but evaluation for more serious arrhythmia is always necessary from an emergency medicine standpoint. As previously mentioned, assessing for underlying reversible causes such as infection, hyperthyroidism and toxins is important. However, if no underlying cause can be found and/or if the patient is unstable, then medical and/or electrical management is warranted.
Unstable Rhythms
In any unstable patient, the American Heart Association (AHA) makes the following recommendations (all Level C recommendations-consensus opinion of experts, case studies or standard of care) (9):
(a) Place the patient in the full left lateral decubitus position to relieve aortocaval compression.
(b) Administer 100% oxygen by facemask to treat and prevent hypoxemia.
(c) Ideally, intravenous (IV) access should be established above the diaphragm to ensure that medications can be adequately distributed into the circulation (not obstructed by the gravid uterus)
(d) Evaluate for any underlying causes of the patient’s symptoms.
Please review the following article for any specifics about cardiac arrest in pregnancy:
Jeejeebhoy FM, Zelop CM, Lipman S, Carvalho B, Joglar J, Mhyre JM, Katz VL, Lapinsky SE, Einav S, Warnes CA, Page RL. Cardiac Arrest in Pregnancy A Scientific Statement From the American Heart Association. Circulation 2015; 132(18):1747-73.
However, just as in non-pregnant patients with an unstable tachycardia causing hemodynamic compromise, immediate direct current (DC) cardioversion is indicated (1, 2, 10, 11). Overall, DC cardioversion has been found to be safe in all trimesters of pregnancy, but it does carry a small risk of inducing a fetal arrhythmia (3). Therefore, it is strongly recommended that when possible, cardioversion should be conducted with concurrent fetal monitoring and emergency caesarean section (C-section) availability (1, 3, 6, 12). Women in later stages of pregnancy should have their pelvis tilted to the left to relieve compression of the vena cava, however the process, including the dosing of electricity, is otherwise the same as in non-pregnant patients (3, 7, 13). Higher doses of energy (up to 360J) in refractory cases still remains safe for both the mother and fetus (13).
Medication options for sedation (for cardioversion):
This article is also not intended to be a review of safe sedation in pregnancy. However, some excellent articles on sedation in pregnancy include:
Neuman G, Koren G. MOTHERISK ROUNDS: Safety of Procedural Sedation in Pregnancy. J Obstet Gynaecol Can 2013; 35(2):168-73.
Shergill AK, Ben-Menachem T, Chandrasekhara V, et al. Guidelines for endoscopy in pregnant and lactating women. Gastrointest Endosc. 2012; 76(1):18-24.
Stable Tachyarrhythmias
The majority of arrhythmias during pregnancy are stable and can be managed with conservative therapies (7). Medication therapy should be considered in patients who are symptomatic and/or have tachyarrhythmias that may lead to negative hemodynamic or physiologic complications (7). Of course, any significant acute hemodynamic compromise should lead the provider to consider cardioversion, as mentioned in the above section (14)
In addition, as previously discussed, a thorough history and physical should be conducted to rule out any reversible causes of the arrhythmia such as a pulmonary embolism, hyperthyroidism, hemorrhage, or infections (). A history of prior episodes and/or a history of structural heart disease are also important to obtain. Once reversible causes are ruled out and a thorough history is obtained, a primary stable arrhythmia requiring drug therapy can be considered (3).
The risk of any medication on the mother and fetus should be reviewed prior to its administration. Most antiarrhythmic medications have not been systematically studied in pregnancy and thus, all should be viewed as potentially harmful in pregnancy (6, 15). Most of these drugs are labeled as a Food and Drug Administration (FDA) category C except for amiodarone and atenolol, which are labeled as category D (16). As a review, category C means that risk cannot be ruled out and any category C medication should be used only if the potential benefits outweigh any potential risks to the fetus. Category D means that there is evidence of risk. There may be a benefit of this drug but that patients should be informed of all risks of the drug prior to giving it (16).
It should be noted that as of June 2015, the FDA initiated a change to pregnancy category labeling and that the use of letters will be phased out. In place of letters, a narrative summary based on the risk of each medication will be provided (17). Any medications submitted to the FDA after June 30, 2015 will use the new format immediately and that any prior prescription medications approved after June 2001 will have new labeling within 3-5 years (17). So as of now, most of these antiarrhythmic medications are still under the old letter category labeling but may change in the future.
Teratogenic risk is also the highest in the first eight weeks after fertilization and thus, especially careful consideration should be given to women in early pregnancy who receive drug therapy (18). This is not to say there is no risk in the other stages of pregnancy, but the risk to the fetus is significantly reduced after the first eight weeks (18).
Finally, it should be remembered that many of the physiologic changes of pregnancy will affect drug metabolism (19). Some of these changes include increased plasma volume, reduction in plasma proteins, changes in renal clearance of drugs and altered gastrointestinal absorption (7, 19). Progesterone levels also increase, which can affect hepatic metabolism (7). Thus, administering the lowest effective dose of a medication is prudent in this patient population (7).
- Palpitations/Premature Ventricular Contractions
Palpitations are very common during pregnancy. Along with paroxysmal supraventricular tachycardia, premature atrial and ventricular beats are the most frequently seen arrhythmias in pregnancy (3, 14). Treatment is typically not necessary but in patients with unbearable symptoms, cardioselective beta blockers can be started, but preferably after the first trimester (6).
- Atrioventricular (AV) Nodal Re-entrant Tachycardia (AVNRT) and AV Re-entrant Tachycardia (AVRT):
The most common supraventricular tachycardia in pregnancy is AVNRT. AVNRT occurs when there are dual AV nodal pathways (slow and fast) that form a part of a re-entry circuit. The tachycardia is initiated when a premature beat is blocked in the fast pathway but conducts over the slow pathway (20). If there is enough time for the fast pathway to recover from its refractory period, then the slow pathway impulse (initiated by the premature beat) may conduct retrogradely over the fast pathway and cause the re-entry circuit (20).
AVNRT should not be confused with AVRT, which is the second most common supraventricular tachycardia in pregnancy (21). AVRT occurs in patients with WPW. In AVNRT, the accessory pathways are located within or near the AV node, while in AVRT, the accessory pathways are located in the AV valvular rings (22). The majority of patients will have the orthodromic form with anterograde conduction through the AV conduction system and retrograde conduction via the accessory pathway, which leads to a regular, narrow complex tachycardia. On occasion, antidromic conduction can occur and cause a wide complex tachycardia (Obel et al). If there is concomitant atrial fibrillation and it is conducted via the antidromic pathway, a wide complex, irregular tachycardia can occur (22).
If AVNRT or AVRT is rapid enough, hemodynamic instability can occur and thus, cardioversion may be necessary (1, 14, 21). However, the majority of patients will not have hemodynamic instability and thus, conservative or medication therapies can be initiated.
First line therapies for stable AVNRT in pregnancy (1, 3, 4, 6, 7, 14, 23):
- Vagal maneuvers such as carotid massage or the Valsalva maneuver.
- Adenosine: safe and should be the initial drug of choice. The initial standard doses are the same as in non-pregnant patients – 6mg and 12 mg. Adenosine has a short half live and does not cross the placenta. Minor effects in the mother may include transient bradycardia and dyspnea. Note adenosine can induce bronchospasm and should be a consideration if the patient has a history of asthma.
- Intravenous metoprolol or propranolol can be used if adenosine is ineffective. Beta blockers are considered safe in pregnancy but they have been associated with intrauterine growth retardation. Atenolol should never be given, however as it has been associated with fetal hypotonia, neonatal respiratory depression, low birth weight and hypoglycemia.
- Verapamil should be considered as a third line agent if the above medications are not effective. Doses up to 10mg can be given without affecting the fetal heart rate. Watch for hypotension in the mother, however.
First line therapies for stable AVRT in pregnancy (3, 6, 7, 14, 15, 18):
- Vagal maneuvers
- Adenosine: may be used but only in regular tachycardias. Patients who have orthodromic AVRT with concomitant atrial fibrillation should not receive adenosine or any other AV nodal blocking agent as this can potentially lead to accelerated conduction through the accessory pathway and lead to dangerous ventricular tachycardias.
AV nodal blocking agents including calcium channel blockers and digoxin should also be used with caution in patients with wide complex tachycardias of unknown pathogenesis. Just as in non-pregnant patients, procainamide is the drug of choice in these circumstances.
- Procainamide: IV procainamide is safe in the short-term treatment of AVRT. It should be avoided in patients with underlying structural heart disease as it can be pro-arrhythmogenic. It should not be used long term as it can cause a lupus-like syndrome.
- Focal Atrial Tachycardia:
Focal atrial tachycardia (FAT) is usually associated with structural heart disease and is rarely seen in pregnancy (14). FAT can be difficult to treat as many are resistant to medications and even cardioversion (7, 15). The main objective is to control the maternal heart rate so that tachycardia-induced cardiomyopathy can be prevented. Adenosine should be attempted first as it is diagnostic and may, on occasion, terminate the arrhythmia (6). If adenosine does not work, the next recommended initial therapies are beta blockers, non-dihydropyridine calcium channel blockers or digoxin. Sotalol, flecainide or propafenone can be given if the beforementioned drugs do not work. Finally, amiodarone can be given but only in severe, refractory cases (7, 15).
- Atrial fibrillation/Atrial Flutter:
Unless there is underlying structural heart disease or hyperthyroidism, atrial flutter and atrial fibrillation are rarely seen during pregnancy (15, 21). However, if atrial flutter (AFL) or atrial fibrillation (AF) with a rapid ventricular response is present in pregnancy, serious hemodynamic effects can occur to both mother and fetus (15). Thus, urgent treatment is important in these patients.
Therapeutic options for stable patients with AFL or AF with rapid ventricular response:
- DC or pharmacologic cardioversion: similar to the non-pregnant population, stable pregnant patients who have had AFL or AF for > 48 hours duration will require 3 weeks of anticoagulation and/or a transesophageal echocardiogram to evaluate for a left atrial thrombus prior to the procedure (15). However, if the duration of the arrhythmia is less than 48 hours and the patient’s CHADS2-VASC score is < 2, post-cardioversion anticoagulation may not be necessary (7, 15). In this case, the patient should receive a dose of heparin or weight adjusted low molecular weight heparin (LMWH) prior to and during cardioversion (15). For patients who require anticoagulation after cardioversion, LMWH is the drug of choice (15). Warfarin can be used in the second and third trimesters but not in the first trimester or last month of pregnancy (6, 15). As of now, given the limited research, the new oral anticoagulants should not be used in pregnant patients (6, 15).
If pharmacologic cardioversion is considered, ibutilide or flecainide can be given but only in patients with structurally normal hearts (15, 21, 24). Ibutilide is particularly useful in treating AF in patients with pre-excitation syndromes. It can prolong the QT and thus, pre-treatment with magnesium is recommended (7). Again, amiodarone can be given but only as a last resort. There is less experience with propafenone so it should be avoided unless it must be used as a last resort as well (15).
- Rate control: For stable patients who are not candidates for cardioversion and/or have refractory AF or AFL, rate control is recommended (6, 7, 14, 15, 25). The AHA/ACC do not define what adequate rate control in pregnancy is, nor could any other literature be found regarding a goal maternal heart rate (26).
With the exception of atenolol, beta blockers are recommended as first line rate control medications in patients with rapid AF or AFL who do not have acute heart failure (6, 7, 14, 15, 25).Metoprolol 5mg IV over 5 minutes and repeated, if necessary, is an option for initial rate control (14). Verapamil, diltiazem and digoxin are second line agents (6, 14, 15, 25). Remember that these drugs should not be given if a pre-excitation syndrome is present.
- Ventricular Tachycardia:
Ventricular tachycardia (VT) is rare during pregnancy and inherited disorders should be considered when asking patients about their past medical and family histories (15). Some of the more common causes of VT in pregnancy may include idiopathic right ventricular (RV) outflow tract tachycardia, long QT syndrome, valvular heart disease and hypertrophic cardiomyopathy (3, 6, 15, 27). Rarely does ischemia cause a cardiomyopathy or arrhythmias in pregnant patients but coronary artery dissection or vasospasm has been known to occur in pregnant patients (6). Post-partum cardiomyopathy should also be ruled out in women presenting with new onset VT during the last 6 weeks of pregnancy or in the early post-partum period (15).
The most important goal for pregnant patients with VT is timely conversion back to normal sinus rhythm because eventually, poor perfusion to both mother and fetus can occur (15).Just as in unstable supraventricular rhythms, acute treatment of any unstable VT should always be treated with DC cardioversion (15). Conversely, pharmacotherapy may be considered in pregnant patients with stable VT (6, 13, 15, 27). Importantly, any pregnant patient with a wide complex tachycardia should be evaluated by obstetric and cardiology specialists (18).
Idiopathic RV outflow tract tachycardia is one of the more common types of VT seen in pregnancy. It is almost always a stable tachycardia and most of the time, it is not sustained. The recommended treatment is beta blockade or verapamil. Idiopathic LV tachycardia is not as common but it responds well to verapamil (3, 15).
In pregnant patients with stable monomorphic VT, lidocaine, procainamide, or sotalol are recommend as first line agents (3, 15, 27).
Polymorphic VT is definitely most concerning as it has a higher likelihood of converting to ventricular fibrillation (3). Long QT syndrome should be a concern in patients with polymorphic VT and thus, all medications that may prolong the QT should be eliminated. In addition, treatment should include magnesium and correction of any electrolyte disturbances (3). Magnesium should be given at a dose of 1-2 grams IV over 1-2 minutes (13). It is controversial whether pregnant patients with long QT are at risk for VT during pregnancy, but it has been demonstrated that patients with long QT are definitely at an increased risk for arrhythmias post-partum (28, 29). Thus, any post-partum patient who presents in VT should have long QT syndrome as a possible etiology of her condition.
Conclusions
While there are a few differences, the management of tachycardic arrhythmias in pregnancy is quite similar to the non-pregnant patient. DC cardioversion should always be conducted in patients with hemodynamic instability. Pharmacologic cardioversion of supraventricular and ventricular arrhythmias is possible in the stable patient. No drugs are completely safe in pregnancy, but most are rated category C in pregnancy and if the benefit exceeds the risk, then the medication may be given. Amiodarone and atenolol are two medications that should be avoided in the pregnant patient, especially in the first trimester. Rate control with beta blockers or calcium channel blockers is an option in patients with supraventricular tachycardias who are not immediate candidates for cardioversion. Stroke risk should still be accounted for and at risk patients should be anticoagulated with LMWH or vitamin K antagonists (only in the 2nd and 3rd trimesters and not in the last month of pregnancy). Finally, close cardiac monitoring of both the mother and fetus and availability of emergency C section should be available whenever medication or cardioversion is indicated. Finally, but importantly, obstetrics and cardiology consultation is prudent whenever a pregnant patient with an abnormal tachycardic arrhythmia presents to the ED.
Case Resolution
Case 1: The patient in this case has new onset AVNRT. Her electrolytes are normal, her thyroid function is normal, and her infection workup is negative. Since her vital signs are otherwise stable and she denies chest pain, adenosine 6mg IV push is administered. Her rhythm returns back to normal sinus rhythm and she is discharged home with close cardiology and obstetrics follow up.
Case 2: This patient has unstable ventricular tachycardia. She is immediately cardioverted with direct current. She was ultimately found to have right ventricular (RV) outflow tract tachycardia. Obstetrics and cardiology were consulted and the patient was admitted for maternal and fetal cardiac monitoring. She was eventually discharged with a beta blocker for prophylaxis and cardiology follow up.
Case 3: The last patient has atrial fibrillation with rapid ventricular response. Her workup for infection is also negative and her thyroid function tests and electrolytes are normal. Since her symptoms had been present for several days, rate control was chosen. Metoprolol was given and she achieved adequate rate control. She was admitted for a transesophageal echo prior to cardioversion and eventually she was cardioverted back to normal sinus rhythm.
References/Further Reading
- Tromp CH, Nanne AC, Pernet PJ, Tukkie R, Bolte AC. Electrical cardioversion during pregnancy: safe or not? Neth Heart J 2011;19(3):134-6.
- Ferrero S, Colombo BM, Ragni N. Maternal arrhythmias during pregnancy. Arch Gynecol Obstet 2004; 269(4):244-53.
- Adamson DL, Nelson-Piercy C. Managing palpitations and arrhythmias during pregnancy. Heart. 2007; 93(12):1630-6.
- Newstead-Angel J, Gibson PS. Cardiac drug use in pregnancy: safety, effectiveness and obstetric implications. ExpertRev Cardiovasc Ther 2009; 7(12):1569-80.
- Gaiser R. Physiologic changes of pregnancy. Chestnut’s obstetric anesthesia: Principles and practice. 2009;4:15-36.
- Enriquez AD, Economy KE, Tedrow UB. Contemporary management of arrhythmias during pregnancy. Circ Arrhythm Electrophysiol 2014;7(5):961-7.
- Burkart TA, Miles WM, Conti JB. Principles of Arrhythmia Management During Pregnancy. Cardiovascular Innovations and Applications. 2016;1(2):143-55.
- Joglar JA, Page RL. Management of arrhythmia syndromes during pregnancy. Curr. Opin. Cardiol. 2014; 29(1):36-44.
- Jeejeebhoy FM, Zelop CM, Lipman S, Carvalho B, Joglar J, Mhyre JM, Katz VL, Lapinsky SE, Einav S, Warnes CA, Page RL. Cardiac Arrest in Pregnancy A Scientific Statement From the American Heart Association. Circulation. 2015;132(18):1747-73.
- Petrescu V, Petrescu M, Bogdan S. Arrhythmias in Pregnancy-one case report and current recommendations from a cardiological perspective. GINECO RO 2010; 6(2):124-7.
- Crijns HJ. Electrical cardioversion in healthy pregnant women: safe yes, but needed? NethHeartJ 2011; 19(3):105-6.
- Barnes EJ, Eben F, Patterson D. Direct current cardioversion during pregnancy should be performed with facilities available for fetal monitoring and emergency caesarean section. BJOG 2002; 109(12):1406-7.
- Trappe HJ. Emergency therapy of maternal and fetal arrhythmias during pregnancy. J EmergTraumaShock 2010; 3(2):153.
- Knotts RJ, Garan H. Cardiac arrhythmias in pregnancy. In Seminars in perinatology 2014 (Vol. 38, No. 5, pp. 285-288). WB Saunders.
- Regitz-Zagrosek V, Lundqvist CB, Borghi C, Cifkova R, Ferreira R, Foidart JM, Gibbs JS, Gohlke-Baerwolf C, Gorenek B, Iung B, Kirby M. ESC Guidelines on the management of cardiovascular diseases during pregnancy. EurHeartJ 2011:ehr218.
- Food and Drug Administration; Accessed Nov 15, 2016: www.fda.gov.
- Food and Drug Administration. Content and format of labeling for human prescription drug and biological products; requirements for pregnancy and lactation labeling. Federal registrar 2014; Vol. 79 (233): 72064-72103.
- Page RL. Treatment of arrhythmias during pregnancy. AmHeartJ 1995;130(4):871-6.
- Cox JL, Gardner MJ. Treatment of cardiac arrhythmias during pregnancy. Prog Cardiovasc Dis. 1993; 6(2):137-78.
- Kwaku KF, Josephson ME. Typical AVNRT—an update on mechanisms and therapy. Card Electrophysiol Rev. 2002; 6(4):414-21.
- Merino JL, Perez-Silva A. Tachyarrhythmias and Pregnancy.
- Obel OA, Camm AJ. Accessory pathway reciprocating tachycardia. EurHeartJ 1998; 19:E13-24.
- Elkayam U, Goodwin TM. Adenosine therapy for supraventricular tachycardia during pregnancy. Am J Cardiol 1995; 75(7):521-3.
- Kockova R, Kocka V, Kiernan T, Fahy GJ. Ibutilide‐Induced Cardioversion of Atrial Fibrillation During Pregnancy. J Cardiovasc Electrophysiol. 2007;18(5):545-7.
- Cacciotti L, Passaseo I. Management of Atrial Fibrillation in Pregnancy. J AtrFibrillation 2010;2(2).
- Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Ohman EM. Management of patients with atrial fibrillation (compilation of 2006 ACCF/AHA/ESC and 2011 ACCF/AHA/HRS recommendations): a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(18):1935-44.
- Gowda RM, Khan IA, Mehta NJ, Vasavada BC, Sacchi TJ. Cardiac arrhythmias in pregnancy: clinical and therapeutic considerations. Int J Cardiol 2003;88(2):129-33.
- Meregalli PG, Westendorp IC, Tan HL, Elsman P, Kok WE, Wilde AA. Pregnancy and the risk of torsades de pointes in congenital long-QT syndrome.
Neth Heart J. 2008; 16(12):422-5. - Seth R, Moss AJ, McNitt S, Zareba W, Andrews ML, Qi M, Robinson JL, Goldenberg I, Ackerman MJ, Benhorin J, Kaufman ES. Long QT syndrome and pregnancy. J Am Coll Cardiol. 2007; 49(10):1092-8.




