Author: Tim Montrief (@EMinMiami, EM Resident Physician, Jackson Memorial Health System) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case: A 75-year-old male with PMH of HTN and DM presents to the ED with complaints of shortness of breath and dyspnea on exertion. He states he had emergent “triple bypass” more than 1 week prior, complicated by a small pericardial effusion, and was discharged home yesterday. Since he got home, he has become increasingly short of breath and is now unable to sit up without feeling incredibly dyspneic. ROS is otherwise negative. Vital signs reveal hypotension, tachypnea, and tachycardia. Exam demonstrates jugular venous distention (JVD) and distant heart sounds.
Background
How common are post-CABG complications? What are the risk factors for complications?
While there has been a recent decline in all cardiac revascularization procedures, there remains over 200,000 coronary artery bypass graft (CABG) surgeries performed in the United States annually.1 Coronary artery bypass graft (CABG) surgery is often considered a high-risk procedure, associated with a 30-day morbidity and mortality rate up to 14.0% and 2.0%, respectively.2 Recently, there has been an increased institution of early extubation and fast track protocols, which has resulted in earlier hospital discharge, with an average post-op length of stay of 5.4 days.3 This leads to more patients at home and more post-CABG patients presenting to the ED for acute complications. Many of the patients discharged after CABG surgery require ED visits and hospital readmissions within 30 days, often for similar diagnoses. Approximately 14% of Medicare post-CABG patients are readmitted within 30 days of discharge, while an additional 10% visit the ED, many for complications from and care related to the surgery.4-6 Overall, 7% of post-CABG patients will experience more than 1 readmission or ED visit within 30 days of surgery.4
Risk factors for perioperative mortality and morbidity after CABG surgery can be divided into 3 categories: patient characteristics, provider characteristics, and postoperative factors.7,8 Patient characteristics include older age, female sex, African American race, greater body surface area, and previous myocardial infarction within 1 week. Patient comorbidities associated with increased morbidity/mortality include history of femoral/popliteal disease, COPD, CHF, calcified ascending aorta, carotid/cerebrovascular disease, aortoiliac disease, hepatic failure, renal failure, previous myocardial infarction, and previous open heart surgery. Provider factors include annual surgeon CABG volume less than 100 cases per year and hospital risk-adjusted mortality rate in the highest decile. Postoperative factors include discharge to nursing home or rehabilitation/acute care facility and length of stay during index CABG admission greater than 5 days.9,10
Definition
What are the most common post-CABG complications?
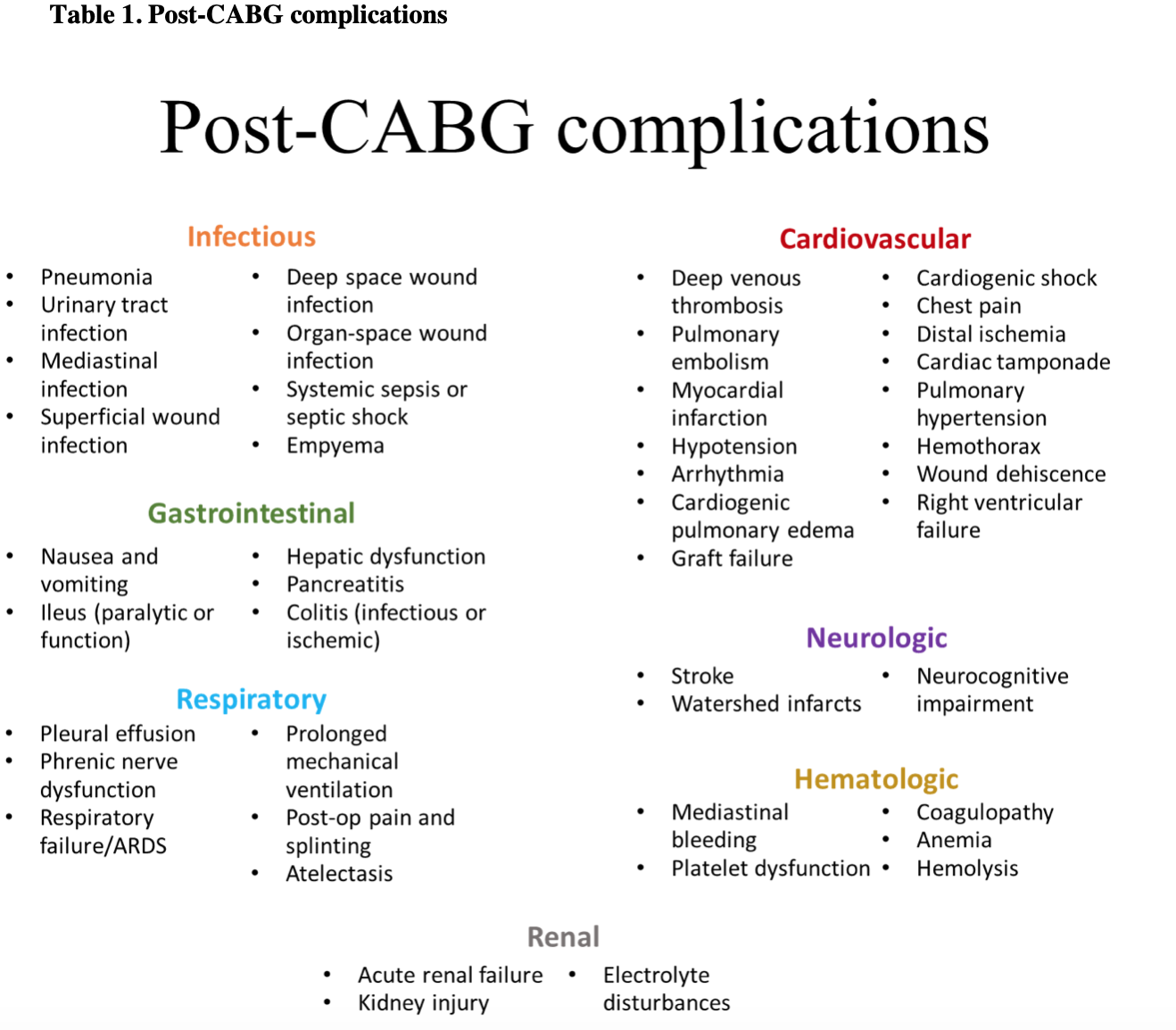
Using cardiopulmonary bypass and having your blood pumped in a non-pulsatile fashion during CABG is a perverse physiological state which results in a series of post-operative issues. Post-CABG complications can affect many different systems other than the cardiovascular system, as patients are at risk for common post-surgical complications, including respiratory failure, stroke, UTI, renal failure, coagulopathy, limb ischemia, wound dehiscence, pleural effusion, and hematologic abnormalities.11-17 It is important to consider this when evaluating the patient to maintain a broad differential of the potential causes that may lead to the patient’s presentation to the ED.
There are a variety of post-CABG complications, and while no single diagnosis accounts for the majority of ED visits and readmissions, the 3 most common diagnoses include post-operative infections, congestive heart failure, and chest discomfort, respectively.6 “Post-operative infection” is a general term encompassing superficial site infections, pneumonia, UTI, and deep sternal wound infections, including mediastinitis, pericarditis, and myocarditis. Deep sternal wound infections (DSWI) are a relatively uncommon event, occurring in 1–2% of all patients undergoing cardiac surgery. However, DSWIs confer a serious risk to the post-CABG patient, with a 6-30% mortality rate, much higher than the estimated mortality rate of 2% for all cardiac surgery patients.18-22 Toumpoulis and colleagues18 showed that DSWIs conferred an approximately 2.5-fold increase in long term mortality even in successfully treated patients who had survived for at least 6 months postoperatively. Chronic poststernotomy pain varies from 21-56% of all cardiac surgery patients and remains a common presenting complaint in the ED.23-28
There are many causes of CHF in the post-CABG patient, which can be broken into 2 categories: complications from the cardiac surgery itself and complications of the underlying disease that led to CABG. Complications due to CABG itself include graft ischemia, likely due to air bubbles in the graft in the immediate post-op period, which peaks during the first 2 hours post-reperfusion. Early graft failure due to thromboembolism has been reported up to 30 days post-surgery.29-31 One of the most devastating complications is cardiac tamponade. The risk of having a pericardial effusion after cardiac surgery is around 1.5% in the immediate post-op period. Of these patients, almost half have some evidence of clinically significant tamponade and require immediate intervention, and delayed cardiac tamponade is well described.32 Finally, cardiac surgery is inherently arrhythmogenic, producing a variety of electrophysiological disturbances, most commonly atrial fibrillation.33-34 CHF can also occur secondary to the patient’s underlying disease process that led to cardiac surgery, including complications of acute myocardial infarction, such as cardiogenic shock, myocardial rupture, or post-infarction pericarditis. Below is a list of common post-CABG complications organized by organ system:
Important items in history and physical exam
History pearls
History is essential in determining a potential cause of the presentation to the ED and need for further investigations.35 Information regarding the chief complaint can help focus the physician on the possible organ system involved. Additionally, it is necessary to obtain a thorough surgical history including the date of the surgery, current postoperative day, surgical approach, indication for surgery, and what it entailed. Hospital course, as well as any perioperative or immediate postoperative complications such as pericardial effusion, pleural effusion, or arrhythmia should be reviewed, as this may be a clue to a potential complication. Elective versus emergent surgery is important, as emergent surgeries do not have the ability to obtain pre-operative risk factors and have been found to have a significantly increased mortality and morbidity compared to elective operations.36 Finally, an updated medication reconciliation should be performed including any antibiotics, analgesics, any antiplatelets or anticoagulants, and any cardiovascular medications the patient may be taking.
Physical exam pearls
Vitals signs are crucial in the evaluation of a post-CABG patient, although normal vital signs do not exclude an emergent process. A post-operative fever is a temperature of >100.4ºF.37 Tachypneaor hypoxia may suggest infection, pulmonary embolism (PE), acute pulmonary edema, or pleural effusion as the etiology. Hypotension may be suggestive of sepsis from a DSWI, cardiac tamponade, or cardiogenic shock from a variety of reasons and warrants immediate resuscitation. Tachycardia may be due to pain, infection, anemia, or delayed bleeding, although a broad differential should be maintained to determine the etiology.
While the cardiopulmonary evaluation usually focuses on the heart and lungs, it should also include a broad assessment for other abnormalities. A thorough cardiovascular exam should include auscultation for murmurs and distant heart sounds, perfusion status, peripheral pulses, presence or absence of JVD, hepatomegaly, peripheral edema, and bilateral upper extremity blood pressure. Assess all lung fields for absent breath sounds, rales, consolidation, wheezes, and rhonchi. Additionally, evaluate for depth of breathing, tachypnea, splinting, and accessory muscle use. Careful evaluation of the surgical incision is important to evaluate for dehiscence and infection, although the physical exam may be normal in patients with a DSWI. Overlying erythema, warmth, or induration suggest the presence of infection. Any fluctuance or drainage is also important to note, suggesting the presence of a hematoma or abscess.
Diagnostic Considerations
Laboratory Testing
Laboratory testing should be guided by the patient’s clinical presentation, history, and underlying comorbidities. Several important investigations for a patient presenting with chest discomfort include an EKG, CBC, type and screen, troponin, basic metabolic panel, and imaging (bedside ultrasound, Computed Tomography (CT), chest x-ray). Likewise, a patient presenting with a fever may necessitate an infectious workup, which can include laboratory investigations ranging from complete blood counts, blood cultures, urine cultures, and imaging (plain films, ultrasound, CT).
Imaging
Imaging should be guided by the patient’s clinical presentation, history, and underlying comorbidities. However, point of care ultrasound (POCUS) is an invaluable tool to evaluate for pleural effusions, global and regional wall motion abnormalities, valvular dysfunction, vegetations or abscesses, aortic dissection, and for the presence of pericardial effusion and any associated tamponade physiology. When evaluating for a pericardial effusion, care must be taken, as a retrocardiac clot is difficult to see on either transthoracic echo or X-ray. Chest x-ray also provides information on the integrity of sternal closure wires, while allowing evaluation of the lung fields. Chest CT is often warranted in evaluation for the various complications during the postoperative period including deep space infection, dysphagia, or surgical leak. It is important to consider IV contrast or the use of CT angiography to help in deciphering structures and highlighting the vascular structures of interest.
Medication Considerations
Pain is often the chief complaint that has brought the patient to the ED. A routine post-sternotomy home regimen includes opiates, acetaminophen, and NSAIDs. However, when considering treatment in the ED, opiates remain the mainstay.38 A variety of antiemetics are available for treatment of nausea. Ondansetron is a common, safe, and readily available medication, and is often the first line due to its lack of sedation seen in promethazine or risk for akathisias seen with metoclopramide and prochlorperazine. Additional consideration should be given to the evaluation of any new medications the patient is taking, as post-cardiac surgery patients may begin many new medications after discharge, including anti-platelet agents, β-blockers, nitrates, ACE inhibitors, lipid-lowering agents, and possibly antibiotics.
Post-surgical Complication Management Pearls based on Differential Diagnosis
Sternal Wound Infections
In defining sternal wound infections, it is important to distinguish between DSWI and superficial sternal wound infections (SSWI).A SSWI involves the skin, subcutaneous tissue, and/or pectoralis fascia only. There is no bony involvement, nor is there mediastinal involvement. The incidence of SSWI ranges from 0.5-8% with a combined morbidity and mortality of 0.5-9%.39 In contrast, deep sternal wound infections (DSWI) are a relatively uncommon event, only occurring in about 1–2% of all patients undergoing cardiac surgery. However, DSWIs confer a serious risk to the post-CABG patient, with a 6-30% mortality rate. Despite the significant clinical consequences of sternal wound infections, there are currently no specific guidelines for the prevention and treatment of sternal wound infections. The Centers for Disease Control and Prevention, however, have a definition of DSWI and require the presence of one of the following criteria:40
- An organism isolated from culture of mediastinal fluid or tissue;
- Evidence of mediastinitis seen during operation; or
- Presence of either chest pain, sternal instability, or fever (>38° C), and purulent drainage from the mediastinum, or isolation of an organism present in a blood culture or a culture of the mediastinal area.
Sternal wound infections are a clinical diagnosis, although imaging support usually consists of chest CT, which is highly sensitive and assists in determining the depth of sternal wound dehiscence.41 The treatment of sternal wound infections must be individualized based on the depth of the infection, the organisms that are cultured, and the patient’s clinical status. Treatment of superficial infections is similar to localized abscesses: incision and drainage to allow unimpeded drainage of the purulent material and packing the wound with dressing changes. For deep sternal wound infections, management principles include debridement of devitalized/necrotic tissue, drainage of infected spaces, antibiotic therapy, and techniques to achieve closure of the sternal space.42 In a 10 year surveillance study of sternal wound infections, methicillin-sensitive Staphylococcus aureus accounted for 28.3% of the isolates, Pseudomonas aeruginosa 18.3%, MRSA14.6%, and Enterobacter species 6.7%.43 In terms of establishing a causative organism, superficial swabs of the sternal incision predicted the pathogen 75% of the time in DSWIs, which improved to 82% of the time when blood cultures were included.43
Management in the ED of a suspected DSWI consists of obtaining appropriate imaging, sternal wound cultures, blood cultures, and starting empiric antibiotic therapy covering both gram-negative and gram-positive species. Early consultation with the surgical team for possible debridement andnegative pressure wound therapy (NPWT) is critical.
Pneumonia
Postoperative cardiac surgery patients are at a markedly increased risk for developing pneumonia secondary to postoperative chest wall pain that limits their mobility, ability to cough, and inspiratory effort. In those who undergo mechanical ventilation, even for a short period of time, risk and mortality are both increased.45 Post-operative pneumonia incidence can range from 6.37% to as high as 35.2% in high-risk groups, with a 30-day post-operative mortality as high as 42%.46-47 This is dependent on patient comorbidities, illness severity, and the causative pathogen, with ventilator-associated pneumonia having a higher mortality rate. Evaluation of possible pneumonia includes a thorough clinical history and physical exam, as well as laboratory tests, chest radiography, and consideration of a possible DSWI when beginning broad-spectrum antibiotics.
Venous Thromboembolism (Deep Vein Thrombosis/Pulmonary Embolism)
Venous thromboembolism (VTE) continues to remain one of the most common preventable causes of readmission, accounting for 6.3% of all post-CABG readmissions, despite the low overall cumulative incidence of PE following cardiac surgery (1.3%), and low associated mortality (0.5%).13, 48-49 The low incidence is likely due to the high rate of anticoagulation in this population. However, these patients undergoing CABG have predisposing risk factors for VTE formation, including prolonged immobilization and recovery, surgical trauma to the lower limbs during vein harvesting, myocardial infarction, atrial fibrillation, heart failure, hyperlipidemia, obesity, and postoperative heparin‐induced thrombocytopenia.
While D-dimer has a high sensitivity, it has only moderate specificity, and should not be used in the post-CABG surgical patient. There are no other differences in imaging and treatment of VTEs in the post-CABG patient, and ACEP guidelines may be followed.50 Hemodynamically unstable patients presenting with PE without contraindications may undergo thrombolytic therapy, catheter assisted thrombolectomy, or surgical pulmonary embolectomy, although discussion with the operative team should be considered in conjunction to treatment.
Approach to the hemodynamically unstable cardiac surgery patient
The hemodynamically unstable, crashing post cardiac surgery patient provides a diagnostic and therapeutic challenge due to the numerous potential underlying mechanisms and pathophysiology. These patients may present in any combination of obstructive, cardiogenic, septic, or hypovolemic shock. In addition to the standard history and physical examination obtained on every patient, the following simple evaluations should be performed immediately on every hemodynamically unstable post-CABG patient:
- Blood glucose measurement to screen for hypoglycemia.
- Assessment of hands and feet for abnormal vasodilation and symmetric bilateral pulses.
- Assessment of skin for urticaria, facial swelling, and angioedema present in anaphylactic shock.
- Careful cardiopulmonary examination for any tracheal deviation, new murmurs, decreased or absent breath sounds, and increased jugular venous distention.
- Place the patient on a cardiac monitor and observe for any dysrhythmias.
These simple actions will help evaluate for the presence of anaphylaxis, arrhythmias, valve failure, and pneumothorax/tension pneumothorax. However, there are critical investigations necessary to further assess for the presence of ischemia, tamponade, hemorrhage, cardiogenic shock, PE, and septic shock. These include:
- EKG to evaluate for myocardial ischemia and arrhythmias.
- Chest x-ray or use point of care ultrasound to evaluate for the presence of pneumothorax, tension pneumothorax, pulmonary edema, or underlying pneumonia.
- Stat CBC looking for hemorrhage sufficient to cause hypovolemic shock, and leukocytosis indicative of septic shock. VBG can provide important information regarding acid/base and lactic acid.
- Perform a point of care echocardiogram to assess for valve dysfunction, myocardial contractility, presence of right heart strain, left ventricular (LV) outflow tract obstruction, right ventricular (RV) failure, or presence of cardiac tamponade.
Immediate management is focused on the basics of resuscitation: airway, breathing, circulation, and hematology. In the complicated post-CABG patient, all hemodynamic variables must be optimized, including preload, rate, rhythm, contractility, and afterload. Principles for addressing these variables are below.51
Airway:
- Intubation, if necessary, should be preceded by appropriate resuscitation, especially in the hemodynamically unstable patient, as there is a clinically significant rate of peri-intubation cardiac arrest.
Breathing:
- Maintain SpO2 ~ 96-100% in order to maintain satisfactory tissue oxygen delivery.
- Adjust positive pressure, with two goals in mind:
- Enhancement of preload by controlling intrathoracic venous return.
- Enhancement of afterload by increasing left ventricular transmural pressure.
Circulation
- Preload
- Maintain diastolic pressure with norepinephrine and/or vasopressin, if necessary.
- Ensure there is no cardiac tamponade (which decreases preload).
- Give a fluid bolus and ensure there is adequate filling. Consider performing some dynamic tests for fluid responsiveness.
- Diastolic failure is common in post-CABG patients, due to a stiff and hypertrophied ventricle with decreased compliance. These patients require increased LV filling pressures, and reduced cardiac output may be due to inadequate preload responsive to a fluid bolus.
- Dobutamine tends to improve LV diastolic relaxation, thereby improving the compliance of the chamber, allowing the fluid bolus you have given to improve LV filling. Levosimendan and milrinone are alternative choices, if available.
- Hemorrhage and hypovolemia also lead to decreased preload and need to be considered.
- The complex topic of RV failure can be summarized as follows: the management will be some combination of fluid bolus and hemodynamic support. Norepinephrine and vasopressin are the most commonly used medications.
- Rate
- This is relatively straightforward. Cardiac output = heart rate x stroke volume. If you cannot augment the stroke volume, you can try to increase the heart rate. If there is diastolic failure, this strategy will result in decreased filling of the ventricle in proportion to the rate increase.
- In most other circumstances, increasing heart rate through a combination of chronotropes (milrinone or dobutamine depending on the presence or absence of pulmonary hypertension) or electrical pacing may be needed.
- Rhythm
- The best rhythm is sinus, as up to 30% of the cardiac output is lost if the “atrial kick” disappears in atrial fibrillation, which occurs in up to 40% of post-CABG patients.51
- Contraction of the left atrium is critical for the patient in diastolic failure; poor left ventricular filling can result from the atria failing to inject an adequate amount of blood into the ventricular chamber. A patient in atrial fibrillation will have decreased preload, leading to hemodynamic instability.
- Control of the rhythm is achieved mainly by amiodarone. Electrical cardioversion should be considered only if there is severe hemodynamic compromise.
- Contractility
- The choice of specific inotrope is outside of the scope of this post. However, in brief, one can increase RV + LV contractility with epinephrine. Likewise, dobutamine which acts more as a chronotrope than an inotrope and has little effect on pulmonary vascular resistance, is an alternative.
- Ensure that the patient has not developed graft occlusion or myocardial ischemia with subsequent cardiogenic shock.
- Afterload
- Choice of vasodilatory agent depends on the patient’s clinical context, but one can decrease RV afterload with pulmonary vasodilators as necessary.
- Aortic pressure increases myocardial oxygen demand and decreases the ejection fraction, thus decreasing the cardiac output. Thus, one may consider using vasodilators to reduce afterload in these patients.
- Systemic arterial hypotension is treated with norepinephrine or vasopressin. Vasopressors work by increasing the systolic pressure, which also increases afterload, and does not improve the diastolic filling of coronary arteries. The main contribution of vasopressors is through venoconstriction, thus increasing the preload and improving left ventricular filling.
Hematology: blood transfusion
- Keep the hemoglobin around 8.0 g/dl.
- Too little hemoglobin may result in tissue hypoxia, especially with fluctuating cardiac output.
- Too much hemoglobin adds to the myocardial workload by increasing the mass of the blood being pumped, which may end up being counterproductive.
Disposition
Early consultation with the operative team can help the clinician clarify the patient’s operative course, as well as desired diagnostic approach. Early consultation also facilitates timely management and coordinated handoff to ensure the best patient care possible. Level of care is dependent on the patient’s underlying pathophysiology, hemodynamic status, need for invasive monitoring, and underlying comorbidities. Recent literature has shown that when complications occur after a major surgical procedure, returning the patient to the index hospital to be cared for by the original surgical team significantly improves 90-day survival, compared to admission at a non-index hospital.53
Pearls and Pitfalls
- Post-CABG patients most commonly present to the ED for post-operative infections, CHF, and chest discomfort.
- DSWIs occur in 1–2% of all patients undergoing cardiac surgery, but have up to a 30% mortality rate.
- Ultrasound is an invaluable tool to evaluate for a pericardial effusion, but a retrocardiac clot is difficult to see on either transthoracic echo or X-ray and may be missed.
- Acute resuscitation of the hemodynamically unstable post-CABG patient includes optimizing preload, rate, rhythm, contractility, and afterload.
- Early surgical consultation can help guide the diagnostic and therapeutic management.
Case Resolution
Bedside echocardiogram shows a large pericardial effusion with evidence of tamponade, and a pericardiocentesis is successfully completed, returning 600 ml of blood, which re-accumulates. The surgical team is consulted, and they return to the OR where they find the source of the mediastinal bleeding. The patient makes an uneventful recovery.
References/Further Reading:
- Riley RF, Don CW, Powell W, Maynard C, Dean LS. Trends in coronary revascularization in the United States from 2001 to 2009: recent declines in percutaneous coronary intervention volumes. Circ Cardiovasc Qual Outcomes. 2011 Mar;4(2):193–197
- Lazar HL, Fitzgerald CA, Ahmad T, et al. Early discharge after coronary artery bypass graft surgery: Are patients really going home earlier? The Journal of Thoracic and Cardiovascular Surgery. 2001; 121(5):943-950.
- Shahian DM, O’Brien SM, Normand SL, Peterson ED, Edwards FH. Association of hospital coronary artery bypass volume with processes of care, mortality, morbidity, and the Society of Thoracic Surgeons composite quality score. The Journal of thoracic and cardiovascular surgery. 2010; 139(2):273-82.
- Hannan EL, Zhong Y, Lahey SJ, et al. 30-day readmissions after coronary artery bypasses graft surgery in New York State. JACC Cardiovasc Interv. 2011 May; 4(5):569–576.
- Li Z, Armstrong EJ, Parker JP, Danielsen B, Romano PS. Hospital Variation in Readmission After Coronary Artery Bypass Surgery in California. Circ Cardiovasc Qual Outcomes. 2012 Sep; 5(5):729–37.
- Fox JP, Suter LG, Wang K, Wang Y, Krumholz HM, Ross JS. Hospital-based, acute care use among patients within 30 days of discharge after coronary artery bypass surgery. The Annals of thoracic surgery. 2013; 96(1):96-104.
- Shahian DM, O’Brien SM, Normand SL, Peterson ED, Edwards FH. Association of hospital coronary artery bypass volume with processes of care, mortality, morbidity, and the Society of Thoracic Surgeons composite quality score. The Journal of thoracic and cardiovascular surgery. 2010; 139(2):273-82.
- Slamowicz R, Erbas B, Sundararajan V, Dharmage S. Predictors of readmission after elective coronary artery bypass graft surgery. Aust Health Rev. 2008 Nov; 32(4):677–683.
- Hannan EL, Wu C, Ryan TJ, et al. Do hospitals and surgeons with higher coronary artery bypass graft surgery volumes still have lower risk-adjusted mortality rates? 2003;108(7):795-801.
- Peterson ED, Coombs LP, Delong ER, Haan CK, Ferguson TB. Procedural volume as a marker of quality for CABG surgery. 2004;291(2):195-201.
- Sachdev, G., & Napolitano, L. M. (2012). Postoperative Pulmonary Complications: Pneumonia and Acute Respiratory Failure. Surgical Clinics of North America, 92(2), 321-344. doi:10.1016/j.suc.2012.01.013
- Le Tanneur C, Mongardon N, Haouache H, et al. Acute Lower Limb Ischemia After Coronary Artery Bypass Grafting Journal of Cardiothoracic and Vascular Anesthesia. 2015; 29(6):1624-1626.
- Hannan EL, Racz MJ, Walford G, et al. Predictors of readmission for complications of coronary artery bypass graft surgery. JAMA. 2003; 290(6):773-80.
- Lorusso R, Mariscalco G, Vizzardi E, Bonadei I, Renzulli A, Gelsomino S. Acute Bowel Ischemia After Heart Operations The Annals of Thoracic Surgery. 2014; 97(6):2219-2227.
- Chaudhry R, Zaki J, Wegner R, et al. Gastrointestinal Complications After Cardiac Surgery: A Nationwide Population-Based Analysis of Morbidity and Mortality Predictors Journal of Cardiothoracic and Vascular Anesthesia. 2017; 31(4):1268-1274.
- Labidi M, Baillot R, Dionne B, Lacasse Y, Maltais F, Boulet L. Pleural Effusions Following Cardiac Surgery Chest. 2009; 136(6):1604-1611.
- Schimmer C, Reents W, Berneder S, et al. Prevention of Sternal Dehiscence and Infection in High-Risk Patients: A Prospective Randomized Multicenter Trial The Annals of Thoracic Surgery. 2008; 86(6):1897-1904.
- Mauermann WJ, Sampathkumar P, Thompson RL. Sternal wound infections Best Practice & Research Clinical Anaesthesiology. 2008; 22(3):423-436.
- Salehi Omran A, Karimi A, Ahmadi SH, et al. Superficial and deep sternal wound infection after more than 9000 coronary artery bypass graft (CABG): incidence, risk factors and mortality. BMC infectious diseases. 2007; 7:112.
- Toumpoulis IK, Anagnostopoulos CE, Derose JJ, Swistel DG. The impact of deep sternal wound infection on long-term survival after coronary artery bypass grafting. Chest. 2005; 127(2):464-71.
- De Feo M, Renzulli A, Ismeno G, et al. Variables predicting adverse outcome in patients with deep sternal wound infection. The Annals of thoracic surgery. 2001; 71(1):324-31
- Wouters R, Wellens F, Vanermen H, De Geest R, Degrieck I, De Meerleer F. Sternitis and mediastinitis after coronary artery bypass grafting. Analysis of risk factors. Texas Heart Institute journal. 1994; 21(3):183-8.
- Kalso E, Mennander S, Tasmuth T, Nilsson E: Chronic post-sternotomy pain. Acta Anaesthesiol Scand 2001; 45:935–9Kalso, E Mennander, S Tasmuth, T Nilsson, E
- Meyerson J, Thelin S, Gordh T, Karlsten R: The incidence of chronic post-sternotomy pain after cardiac surgery: A prospective study. Acta Anaesthesiol Scand 2001; 45:940–4Meyerson, J Thelin, S Gordh, T Karlsten, R
- Eisenberg E, Pultorak Y, Pud D, Bar-El Y: Prevalence and characteristics of post coronary artery bypass graft surgery pain (PCP). Pain 2001; 92:11–7Eisenberg, E Pultorak, Y Pud, D Bar-El, Y
- Bruce J, Drury N, Poobalan AS, Jeffrey RR, Smith WC, Chambers WA: The prevalence of chronic chest and leg pain following cardiac surgery: A historical cohort study. Pain 2003; 104:265–73Bruce, J Drury, N Poobalan, AS Jeffrey, RR Smith, WC Chambers, WA
- Ho SC, Royse CF, Royse AG, Penberthy A, McRae R: Persistent pain after cardiac surgery: An audit of high thoracic epidural and primary opioid analgesia therapies. Anesth Analg 2002; 95:820–3Ho, SC Royse, CF Royse, AG Penberthy, A McRae, R
- Jensen MK, Andersen C: Can chronic poststernotomy pain after cardiac valve replacement be reduced using thoracic epidural analgesia? Acta Anaesthesiol Scand 200; 48:871–4
- Szavits-Nossan J, Stipić H, Sesto I, Kapov-Svilicić K, Sipić T, Bernat R. Angiographic control and percutaneous treatment of myocardial ischemia immediately after CABG. Collegium antropologicum. 2012; 36(4):1391-4.
- Laflamme M, DeMey N, Bouchard D, et al. Management of early postoperative coronary artery bypass graft failure. Interactive cardiovascular and thoracic surgery. 2012; 14(4):452-6
- Gukop P, Momin A. Early saphenous vein graft disease following coronary artery bypass grafting Surgery (Oxford). 2018; 36(2):83-85.
- Leiva EH, Carreño M, Bucheli FR, Bonfanti AC, Umaña JP, Dennis RJ. Factors associated with delayed cardiac tamponade after cardiac surgery. Annals of cardiac anaesthesia. ; 21(2):158-166.
- Hirji SA, Lee J, Kaneko T. Current Readings: An Update on Prevention and Management of Atrial Fibrillation Post Cardiac Surgery Seminars in Thoracic and Cardiovascular Surgery. 2018;
- Khan J, Khan N, Loisa E, Sutinen J, Laurikka J. Increasing Occurrence of Postoperative Atrial Fibrillation in Contemporary Cardiac Surgery Journal of Cardiothoracic and Vascular Anesthesia. 2016; 30(5):1302-1307.
- Narayan, M., & Medinilla, S. P. (2013). Fever in the Postoperative Patient. Emergency Medicine Clinics of North America,31(4), 1045-1058.
- Schumer EM, Chaney JH, Trivedi JR, Linsky PL, Williams ML, Slaughter MS. Emergency Coronary Artery Bypass Grafting: Indications and Outcomes from 2003 through 2013. Texas Heart Institute journal. 2016; 43(3):214-9.
- Pile, JC. Evaluating postoperative fever: a focused approach. 2006. Retrieved June 01, 2018, from https://www.ncbi.nlm.nih.gov/pubmed/16570551/
- Lahtinen P, Kokki H, Hynynen M. Pain after cardiac surgery: a prospective cohort study of 1-year incidence and intensity. Anesthesiology. 2006;105(4):794-800.
- Ridderstolpe L, Gill H, Granfeldt H, Ahlfeldt H, Rutberg H. Superficial and deep sternal wound complications: incidence, risk factors, and mortality. Eur J Cardiothorac Surg. 2001;20:1168-75.
- Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for Prevention of Surgical Site Infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27(2):97-132.
- Gur E, Stern D, Weiss J, et al. Clinical-radiological evaluation of poststernotomy wound infection. Plast Reconstr Surg. 1998;101:348–355.
- Lazar HL, Salm TV, Engelman R, Orgill D, Gordon S. Prevention and management of sternal wound infections. J Thorac Cardiovasc Surg. 2016;152(4):962-72.
- Si D, Rajmokan M, Lakhan P, Marquess J, Coulter C, Paterson D. Surgical site infections following coronary artery bypass graft procedures: 10 years of surveillance data. BMC Infect Dis. 2014;14:318.
- Chaudhuri A, Shekar K, Coulter C. Post-operative deep sternal wound infections: making an early microbiological diagnosis. Eur J Cardiothorac Surg. 2012;41(6):1304-8.
- Sachdev, G., & Napolitano, L. M. (2012). Postoperative Pulmonary Complications: Pneumonia and Acute Respiratory Failure. Surgical Clinics of North America,92(2), 321-344. doi:10.1016/j.suc.2012.01.013
- Allou N, Allyn J, Snauwaert A, et al. Postoperative pneumonia following cardiac surgery in non-ventilated patients versus mechanically ventilated patients: is there any difference? Crit Care. 2015;19:116.
- He S, Chen B, Li W, et al. Ventilator-associated pneumonia after cardiac surgery: a meta-analysis and systematic review. J Thorac Cardiovasc Surg. 2014;148(6):3148-55.e1-5.
- Protopapas AD, Baig K, Mukherjee D, Athanasiou T. Pulmonary embolism following coronary artery bypass grafting. J Card Surg. 2011;26(2):181-8.
- Shammas, NW: Pulmonary embolus after coronary artery bypass surgery: A review of the literature. Clin Cardiol2000;23:637-644.
- Wolf SJ, Hahn SA, Nentwich LM, et al. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department With Suspected Acute Venous Thromboembolic Disease. Ann Emerg Med. 2018;71(5):e59-e109.
- Yartsev A. Approach to the Haemodynamically Unstable Cardiac Surgical Patient. Deranged Physiology.
- Ismail MF, El-mahrouk AF, Hamouda TH, Radwan H, Haneef A, Jamjoom AA. Factors influencing postoperative atrial fibrillation in patients undergoing on-pump coronary artery bypass grafting, single center experience. J Cardiothorac Surg. 2017;12(1):40.
- Brooke, B., Goodney, P., & Kraiss, L. Readmission Destination and Risk of Mortality After Major Surgery: An Observational Cohort Study. Journal of Vascular Surgery. 2016;63(4):1126.




