
Authors: Tyler Humphrey, MD (Emergency Medicine Resident, Advocate Christ Medical Center, Oak Lawn, IL), Michael Cirone, MD (@mcironeMD – Assistant Program Director, Advocate Christ Medical Center, Oak Lawn, IL) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 31-year-old previously healthy male is brought into the Emergency Department by friends for a speech disturbance that occurred while scuba diving. His symptoms started approximately one minute after surfacing. He is alert, follows commands, and moves all extremities, but is aphasic. He has no past medical history and does not take any medications.
What are your interventions? What tests do you order? Does he need a head CT? Who can you consult for assistance?
Introduction
Recreational scuba diving has inherent risks, but serious injuries and fatalities related to diving are relatively uncommon.1,2 Many emergency physicians may never see a true diving emergency during their career (especially those not practicing near a coast). Diving emergencies are a low frequency, yet high impact area of practice for emergency physicians.
Barotrauma of Descent
Mask Barotrauma – As a diver descends, the ambient pressure increases, causing the volume of air in the dive mask to decrease (Boyle’s Law). As a diver descends, they musk exhale through the nose to increase the volume of air to maintain pressure in the mask. If unable to do so a vacuum effect is created from the negative pressure and can rupture capillaries causing subconjunctival hemorrhage, periorbital ecchymosis, and lid edema. Treatment is supportive care with cold compress and analgesia.1 Rarely, mask squeeze can be severe, and the patient may have symptoms including diplopia and vision loss which may suggest an orbital or subperiosteal hemorrhage.3-6 A careful dive history and physical exam should be performed to distinguish from arterial gas embolism or decompression sickness (see below). This distinction is critical, as a suspected orbital hemorrhage needs imaging (CT) and emergent ophthalmology consultation, rather than transfer to hyperbaric facility for case of suspected arterial gas embolism (AGE) (and hyperbaric treatment is contraindicated in orbital hemorrhage).3
Sinus Barotrauma – Normally, air should easily flow between the paranasal sinuses and the nasal cavity (via the sinus ostia). Obstruction of airflow between the sinuses and the nasal cavity can occur from an upper respiratory infection or allergies. This impairs the ability to maintain pressure in the sinuses as a diver descends and the ambient pressure increases. Negative pressure in the sinuses acts as a vacuum causing mucosal edema or in severe cases, bleeding.7,8 Divers most commonly present with sinus pain during descent.7,9 Sinus barotrauma is treated with supportive care including vasoconstrictors to reduce mucosal edema.7,10 A systemic decongestant like pseudoephedrine (Sudafed) 60mg every 6 hours can be used if no contraindications such as uncontrolled hypertension or glaucoma. Addition of a topical decongestant like oxymetazoline (Afrin) 0.05%, 2 sprays per nostril BID for up to 3 days can also provide relief. A short course of oral corticosteroids may help speed recovery.7,11 If medical management fails or patients have recurrent sinus barotrauma, they should be referred to ENT for surgical evaluation.12
Ear Barotrauma
External Auditory Canal – Obstruction of the canal (tight wetsuit hood, cerumen) traps air in the canal, preventing pressure equalization. The negative pressure can cause erythema, swelling, hemorrhagic bullae, ecchymosis of the canal and rarely, tympanic membrane rupture.1,13,14 The diver may experience ear pain or the sensation of fullness during descent. Hemorrhagic bullae should not be excised if present. External auditory canal barotrauma is treated with warm water irrigation and a fluoroquinolone – steroid otic drops if tympanic membrane rupture (ciprofloxacin 0.3% and dexamethasone 0.1%, three drops BID for seven days).1,13,15
Middle Ear Barotrauma is the most common cause of otalgia in scuba, affecting up to 40% of divers.16,17 Hydrostatic pressure from water in the external auditory canal pushes the tympanic membrane into the middle ear. The inability to equalize pressure by adding air to the middle ear leads to a pressure vacuum causing inflammation. Symptoms include ear pain, sensation of fullness, or decreased hearing.1 Physical exam should evaluate for tympanic membrane rupture, and if present, treat with a fluoroquinolone – steroid otic drops (see above). Combining oral and intranasal decongestants are the mainstay of treatment.18
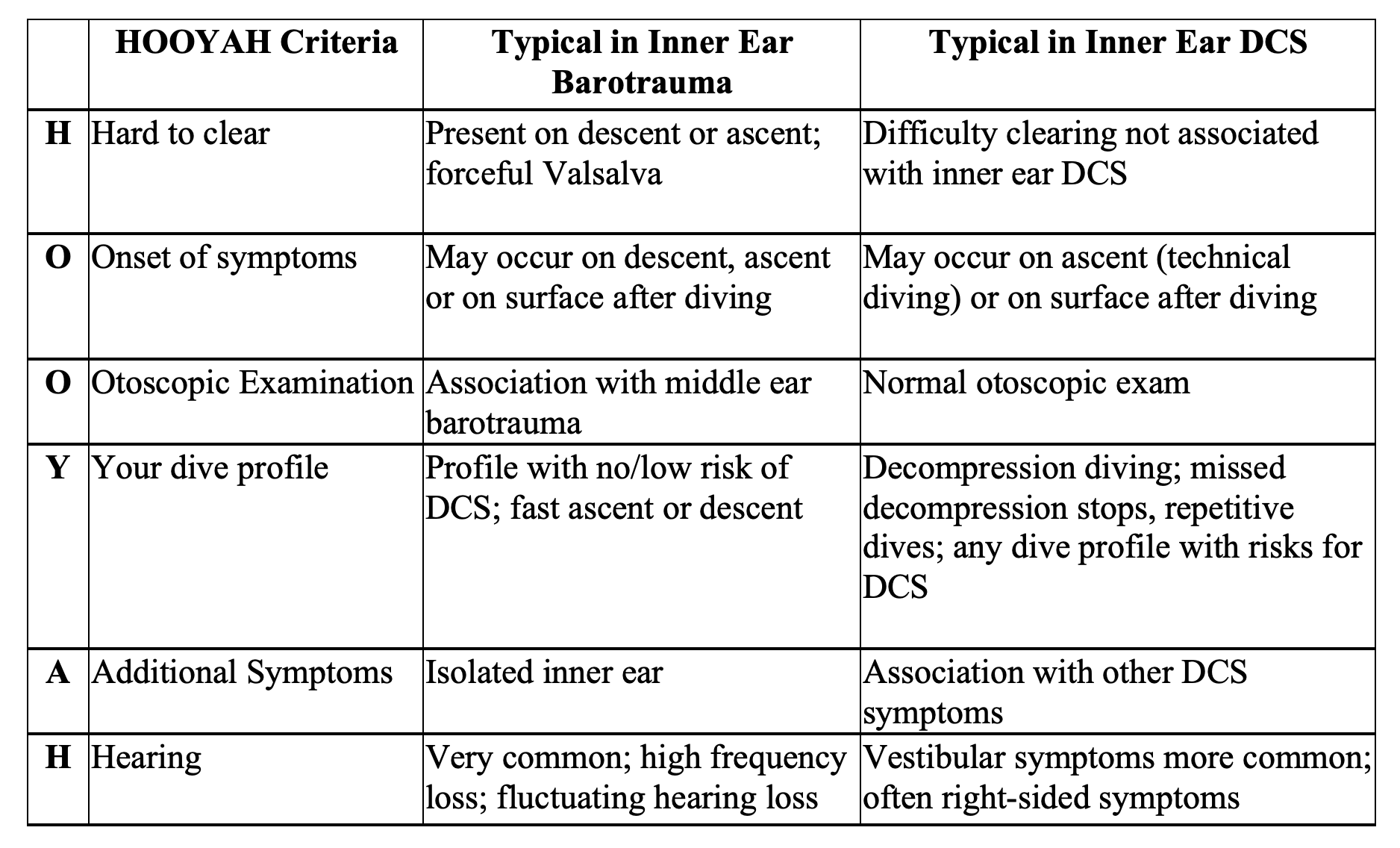
Inner Ear – During descent the tympanic membrane bulges inward causing the stapes to push against the oval window. This increased pressure is propagated through the perilymph and endolymph causing the round window to bulge outward. If the diver valsalvas, intracranial pressure (ICP) increases, and pressure propagates through the perilymphatic duct to the inner ear causing round or oval window rupture.19 Symptoms include tinnitus, hearing loss, and vertigo, although the triad is not always present.20 Management includes ICP precautions including maintaining the head of bed at 30 degrees and avoidance of nose blowing and strenuous activities.21Patients should follow-up with ENT, especially if they have worsening symptoms or persistent vertigo, as it may indicate fistulization of the round window requiring surgical repair.22 In a diver with vertigo, hearing loss, and tinnitus, it is important to determine the time of onset of symptoms. A diver who develops auditory symptoms during descent, or has a difficult time clearing the ears suggests inner ear barotrauma which is treated conservatively. However, development vertigo following a dive suggests inner ear decompression sickness that requires hyperbaric oxygen chamber (contraindicated in inner ear barotrauma). The HOOYAH tool (Hard to clear, Onset of symptoms, Otoscopic exam, Your dive profile, Additional symptoms, and Hearing) may be useful to differentiate between the two processes.23
Pulmonary Barotrauma of Ascent
During ascent, decreased atmospheric pressure leads to expansion of gas in the alveoli. If the diver is unable to exhale the expanding volume (rapid ascent), the alveolar pressure can exceed the ambient pressure causing alveolar rupture. Air from the alveoli can cause four major injury patterns, the most local being alveolar hemorrhage.24 The diver may have chest pain, cough, and hemoptysis, and a chest x-ray may demonstrate an area of hemorrhage/intraparenchymal injury. Treatment of local pulmonary injury is supportive care, including oxygen if needed. Hyperbaric oxygen therapy is not needed for isolated pulmonary injury.
Pneumomediastinum can occur if air from the ruptured alveoli travels along the bronchioles into the mediastinum. Divers may be asymptomatic or present with chest pain, hoarseness, or odynophagia.25 Unlike pneumothorax, there is usually no respiratory distress. Physical exam may demonstrate crepitance under the skin of the chest and neck. Treatment includes rest, avoidance of pressure changes (flying), and supplemental O2 to improve air resorption. Recompression is only indicated if history and exam suggest AGE.1,25
Pneumothorax has been observed in pulmonary barotrauma, although itis less common than pneumomediastinum,26 as the dissecting air has more resistance traveling through the visceral pleura compared to traveling into the mediastinum.1 As opposed to pneumomediastinum, the patient with pneumothorax will usually be dyspneic. Chest pain may be absent if the pneumothorax is large causing the visceral pleura to no longer be in contact with the chest wall. Most pneumothoraces related to diving are small, and thus treated with supplemental oxygen to help resorption, repeat exam, and chest x-ray to ensure resolution. Tube thoracostomy may be required for large pneumothoraces.1,27
Although infrequent, pneumothorax is important to rule out in any diver with suspected AGE or those undergoing recompression therapy. An unidentified pneumothorax can develop into a tension pneumothorax because the gas cannot be vented to the environment during hyperbaric treatment. If a diver has indications for recompression, a chest tube should be placed to allow venting of intrapleural air and prevent conversion to tension pneumothorax.1
Arterial Gas Embolism
Pulmonary barotrauma can cause air from the ruptured alveoli to enter into pulmonary capillaries, to the pulmonary veins, and into the left atrium and left ventricle where they enter the arterial vasculature. Bubbles cause mechanical obstruction and inflammation, leading to ischemia or infarction.1 The bubbles may enter the carotid or vertebral arteries, and if there multiple embolizations affecting separate anatomic areas, patients may have a confusing neurologic picture. Symptoms usually develop within 2 minutes of surfacing.1 Loss of consciousness or neurologic symptoms when surfacing should be considered AGE until proven otherwise.1 In addition to neurologic effects, AGE can produce multiple effects on the cardiovascular system. Gas bubbles in the brainstem may produce dysrhythmias from activation of the autonomic nervous system. 28 Additionally, air bubbles may enter into the coronary arteries. ECG changes may be seen, but acute coronary syndrome is rare.29,30 ECG may demonstrate signs of right heart strain in severe cases of AGE.31 Cardiac arrest may occur from complete obstruction of the central circulation with air.32,33
Diagnosis
Arterial Gas Embolism is primarily a clinical diagnosis based on dive history and physical exam. In general, transfer to a hyperbaric chamber should not be delayed for lab results. However, both hemoconcentration and elevations in creatine phosphokinase may correlate with the severity of arterial gas embolism and provide additional prognostic information.34,35 An ECG should be obtained to evaluate for any dysrhythmias or signs of ischemia, though this is rare. In addition, a chest x-ray should be obtained to evaluate for pneumothorax. In general, a CT or MRI brain will not change management and will likely delay transfer to a hyperbaric facility. Imaging with CT may be needed to evaluate for intracranial hemorrhage or other pathology unrelated to diving.1
Treatment
Management of AGE entails supportive care and expedited transfer to a hyperbaric facility for recompression therapy. In addition to the ABC’s, supplemental oxygen should be started, as it can increase the resolution of gas bubbles.1Victims of AGE tend to be intravascularly depleted, so intravenous fluids can increase the hydrostatic pressure, encouraging removal of gas bubbles in the pulmonary circulation.1 Consultation with an expert in dive medicine, like the Diver’s Alert Network (919-684-9111; https://www.diversalertnetwork.org) can assist with further management recommendations and in locating a nearby hyperbaric facility. Even if a patient has no neurologic symptoms, transfer to a hyperbaric facility should be strongly considered as cerebral edema may develop in a delayed fashion.36
Decompression Sickness1,2
Decompression sickness (DCS) is a systemic disorder resulting from excessive gas formation in the tissues and venous blood. During descent, increased atmospheric pressure causes inert gases like nitrogen (N₂)to cross the alveoli into the pulmonary circulation and dissolve in blood. As a diver ascends, the atmospheric pressure decreases, and these gases can come out of solution forming bubbles in the tissues or venous blood. The bubbles cause an inflammatory reaction by activation of complement system, neutrophils, and microparticles. Bubbles can also damage the endothelial lining causing increased vascular permeability leading to tissue edema.37-41
Clinical Manifestations
DCS has multisystemic effects. Previously, DCS was categorized as Type I or Type II. Type I DCS included mild skin and musculoskeletal manifestations whereas involvement of the inner ear, brain, spinal cord, or cardiopulmonary system was considered the Type II DCS. Describing DCS based on the organ system affected is more appropriate than using Type I and II classifications, which implies that Type I DCS is not serious or cannot progress to “Type II”.1
Cutaneous DCS – “Skin Bends”
A variety of skin manifestations may be seen including a scarlatiniform or erysipeloid rash or pruritus.1Skin mottling or cutis marmorata (marbled appearance) are indications of severe DCS.1,42
Musculoskeletal DCS – “The Bends”
Bubbles may form in the muscles or joints, causing significant pain commonly known as “the bends” or musculoskeletal DCS. Symptoms include a dull, aching pain, most commonly affecting the shoulder and elbow joints. Patients may have a vague sensation of numbness around the joint. Physical exam may demonstrate erythema, swelling, or pain with range of motion. A thorough history should be obtained to determine if the patient sustained any trauma. A bedside test to differentiate DCS versus other dive related trauma involves the use of a sphygmomanometer around the joint inflated to 150-250 mm Hg. The increased pressure can reduce the volume of gas in a joint affected by DCS leading to improvement in symptoms. Although this test may be useful if positive, the poor sensitivity (61%) prevents it from being used as a rule out test. A test of pressure in a hyperbaric chamber may be required.43 The patient undergoes recompression for twenty minutes, and if symptoms improve during this time, DCS is presumed to be the cause of the symptoms.44 Occasionally, a form of avascular necrosis, known as dysbaric necrosis may result from inadequate decompression.45,46
Inner Ear DCS – “The Staggers”
Decompression Sickness can affect the inner ear causing symptoms of vertigo, hearing loss (40%), and tinnitus.47 It is important to distinguish from inner ear barotrauma because inner ear DCS requires hyperbaric chamber rather than supportive care, and delay in hyperbaric chamber for greater than 5 hours results in permanent hearing damage in up to 90% of individuals.48 Patients should receive 100% oxygen while awaiting transportation to hyperbaric facility.49 As discussed previously, it is important to differentiate inner ear barotrauma from inner ear DCS.
Pulmonary DCS – “The Chokes”
Gas bubbles in the pulmonary vasculature can cause this serious form of DCS, which may progress to neurological DCS or shock. Symptoms include pleuritic substernal pain, dyspnea, and cough. The patient may be tachypneic, tachycardia, and cyanotic.
Neurological DCS
DCS can affect both the brain and spinal cord. Spinal Cord DCS is believed to be due to gas bubble formation within the spinal cord itself, as well as gas bubbles with the epidural venous plexus leading to congestive injury.50 The lower thoracic and lumbar spine are most commonly affected. Symptoms include paresthesias (34-87%), limb numbness (56%), followed by lower extremity weakness(23-40%), general malaise (28%), and low back pain (21%).51,52 Exam findings may include paresis, a sensory level, and bladder dysfunction.51
Neurological DCS affecting the brain can cause altered mental status, visual disturbance, vertigo, and ataxia. The presentation is indistinguishable from arterial gas embolism.
Diagnosis of DCS
Decompression sickness is generally a clinical diagnosis based on dive history, time of symptoms, and exam. Symptoms are generally not seen immediately upon surfacing, but most tend to appear within 1 hour.1,52Labs are rarely helpful, but if labs are obtained, hemoconcentration with hematocrit of 50-60 may be seen in severe DCS.34 In musculoskeletal DCS, x-rays are not useful as they do not show abnormalities. In pulmonary DCS, a chest x-ray may reveal pulmonary edema and evaluate for pulmonary barotrauma of ascent. In neurological DCS, CT findings are rarely present and do not correlate with neurologic findings.53 MRI has an unclear prognostic role, but is not recommended in the acute setting as it would delay transfer to a hyperbaric facility.54
Treatment
Given the severity of DCS, treatment should be started as soon as suspected. Hyperbaric chamber therapy is the cornerstone of treatment. The Diver’s Alert Network (919-684-9111; https://www.diversalertnetwork.org) should be contacted to discuss additional management and locating the nearest available hyperbaric treatment facility. If air transport is required, an aircraft capable of maintaining sea level cabin pressure should be used. If a helicopter is used, the flight crew will need to fly at the lowest altitude possible altitude, preferably under 1000 feet.1 In addition to HBOT, intravenous fluids and supplemental oxygen via a non-rebreather should be initiated immediately as they help bubble resorption.
Back to the Case
This is a case of arterial gas embolism, which should be suspected given the neurological disturbance shortly after surfacing. The patient should be started on supplemental oxygen and IV fluids. A fingerstick glucose should be checked given his neurological symptoms, but otherwise lab work will not significantly affect management. A chest x-ray should be obtained to rule out pneumothorax. A head CT should not be obtained if you have a low suspicion for intracranial hemorrhage and if it will delay transfer to hyperbaric chamber.Consultation with Diver’s Alert Network should be performed early for next steps and assistance in locating the nearest hyperbaric chamber.
Key Points
- Conditions related to descent are generally treated with symptomatic management.
- Pulmonary barotrauma of ascent can lead to local pulmonary injury, pneumomediastinum, pneumothorax, or AGE.
- A chest x-ray should be obtained in all cases of suspected pulmonary barotrauma or AGE.
- Any neurological symptoms or loss of consciousness upon surfacing is considered AGE until proven otherwise. Treatment is supplemental O2, IV fluids, and most importantly, a hyperbaric chamber.
- Decompression sickness is more appropriately categorized by the organ system affected, as even minor manifestations can progress to more serious forms.
- While AGE and neurological DCS may be clinically indistinguishable, both are managed similarly with supplemental oxygen, IV fluids, and hyperbaric oxygen therapy.
- In general, AGE and DCS are clinical diagnoses. Labs and imaging should not delay transfer to a hyperbaric facility.
- Consultation with Diver’s Alert Network (919-684-9111; https://www.diversalertnetwork.org) should be performed early in cases of diving emergencies.
References/Further Reading
1. Van Hoesen, K, Lang, M. Diving Medicine. Auerbach’s Wilderness Medicine, by Paul S. Auerbach, 7th ed., vol. 2, Elsevier Mosby, 2012, pp. 1583–1618.
2. Denoble PJ, Pollock NW, Vaithiyanathan P, et al. Scuba injury death rate among insured DAN members.Diving Hyperb Med.38:182 2008 PMID 22692749)
3. Latham E, Van Hoesen K, Grover I. Diplopia due to mask barotrauma.J Emerg Med.41 (5):486-488 2011 189930134
4. Andenmatten R, Piguet B, Klainguti G. Orbital hemorrhage induced by barotrauma. Am J Ophthalmol. 118:536 1994 7943142
5. Butler FK, Gurney N. Orbital hemorrhage following face-mask barotrauma. Undersea Hyperb Med. 28:31 2001 11732882
6. Woo D, Rogers S, Leong J, et al. Non-traumatic subperiosteal orbital hemorrhage secondary to barotrauma. Orbit. 31 (5):347 2012 22694278
7. Livingstone D, Lange B. Rhinologic and Oral-Maxillofacial Complications from Scuba Diving: a Systematic Review with Recommendations. Diving and Hyperbaric Medicine, The Journal of the South Pacific Underwater Medicine Society and the European Underwater and Baromedical Society, 30 June 2018, PubMed ID 6156823
8. Edmonds CB, Bennett M, Lippmann J, Mitchell S, editors. 5 Edition. Florida: CRC Press; 2015. Diving and subaquatic medicine; p. 865.
9. Fagan P, McKenzie B, Edmonds C. Sinus barotrauma in divers . Ann Otol Rhinol Laryngol. 1976;85(1):61–64. PMID 1078539
10. Skevas T, Baumann I, Bruckner T, Clifton N, Plinkert PK, Klingmann C. Medical and surgical treatment in divers with chronic rhinosinusitis and paranasal sinus barotrauma . Arch Otorhinolaryngol. 2012;269:853–860. doi: 10.1007/s00405-011-1742-4.
11. Skevas T, et al. Medical and Surgical Treatment in Divers with Chronic Rhinosinusitis and Paranasal Sinus Barotrauma. European Archives of Oto-Rhino-Laryngology : Official Journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : Affiliated with the German Society for Oto-Rhino-Laryngology – Head and Neck Surgery, U.S. National Library of Medicine, Mar. 2012, PMID 21901337.
12. Skevas T, Baumann I, Bruckner T, Clifton N, Plinkert PK, Klingmann C. Medical
and surgical treatment in divers with chronic rhinosinusitis and paranasal sinus
barotrauma.Eur Arch Otorhinolaryngol. 2012 Mar;269(3):853-60. doi:
10.1007/s00405-011-1742-4. Epub 2011 Sep 8. PubMed PMID: 21901337.
13. Livingstone DM, Smith KA, Lange B. Scuba diving and otology: a systematic
review with recommendations on diagnosis, treatment and post-operative care.
Diving Hyperb Med. 2017 Jun;47(2):97-109.
14. Becker GD, Parell GJ. Barotrauma of the ears and sinuses after scuba diving. Eur Arch Otorhinolaryngol. 2001;258:159-63. PubMed PMID: 11407445.
15. Lacey JP, Amedee RG. The otologic manifestations of barotrauma.J La State Med Soc. 2000;152:107-11.
16. Green SM, Rothrick SG, Hummel CB, et al. Incidence and severity of middle ear barotrauma in recreational scuba diving.J Wilderness Med. 4:270 1993.
17. Jansen S, et al. “Prevalence of Barotrauma in Recreational Scuba Divers After Repetitive Saltwater Dives.” Otology & Neurotology : Official Publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology, U.S. National Library of Medicine, Oct. 2016, PubMed ID 27636390.
18. Mallen J, Roberts DS. SCUBA Medicine for Otolaryngologists: Part II. Diagnostic, Treatment, and Dive Fitness Recommendations – Mallen – – The Laryngoscope – Wiley Online Library. The Laryngoscope, John Wiley & Sons, Ltd, 18 Feb. 2019, onlinelibrary.wiley.com/doi/abs/10.1002/lary.27874.
19. Bohm F, Lessle M: Round window membrane defects in divers. Laryngorhinootologie. 78:169 1999 10407821
20. Böhm F, Lessle M. [Round window membrane defect in divers].
Laryngorhinootologie. 1999 Apr;78(4):169-75. Review. German. PubMed PMID:
10407821.
21. Parell GJ, Becker GD. Conservative management of inner ear barotrauma resulting from scuba diving.Otolaryngol Head Neck Surg. 93:393 1985 3927237)
22. Edmonds C, Freeman P, TonkinF. Fistula of the round window in diving. Trans Am Acad Ophthalmol Otolaryngol. 78:444 1974
23. Rozycki S, et al. “Inner Ear Barotrauma in Divers: an Evidence-Based Tool for Evaluation and Treatment.” Diving and Hyperbaric Medicine, The Journal of the South Pacific Underwater Medicine Society and the European Underwater and Baromedical Society, 30 Sept. 2018, PubMed ID 30199891.
24. Balk M, Goldman JM. Alveolar hemorrhage as a manifestation of pulmonary barotrauma after scuba diving.Ann Emerg Med. 19:930 1990 PubMed ID 2372179.
25. Kosaka T, Haraguchi M, Tsuneoka N, Furui J. Spontaneous pneumomediastinum as
a result of SCUBA diving. Eur J Emerg Med. 2007 Apr;14(2):118-9. PubMed PMID:
17496692.
26. Harker, T. The Roentgenographic Findings Associated with Air Embolism in Sport Scuba Divers. The Journal of Emergency Medicine. 1993 Jul-Aug;11(4):443-9. PubMed PMID: 8228108
27. Moon R. Pulmonary Barotrauma – Injuries; Poisoning. Merck Manuals Professional Edition, Merck Manuals, July 2019, www.merckmanuals.com/professional/injuries-poisoning/injury-during-diving-or-work-in-compressed-air/pulmonary-barotrauma.
28. Evans DE, Kobrine AI, Weathersby PK, Bradley ME. Cardiovascular effects of
cerebral air embolism. Stroke. 1981 May-Jun;12(3):338-44A. PubMed PMID: 7245300.
29. Smith RM, Neuman TS. Elevation of serum creatine kinase in divers with
arterial gas embolization. N Engl J Med. 1994 Jan 6;330(1):19-24. PubMed PMID:
8259140.
30. Sammut M, et al. Coronary Artery Air Embolism Causing Pulmonary Edema Secondary to Acute Coronary Syndrome in a Diver. The Journal of Invasive Cardiology, U.S. National Library of Medicine, Dec. 2008, PubMed PMID 19057040
31. BoveAA, NeumanRS, Smith RM. ECG changes associated with pulmonary barotrauma. Undersea Hyperb Med. 22:55 1995
32. Neuman TS, Jacoby I, Bove AA. Fatal pulmonary barotrauma due to obstruction
of the central circulation with air.J Emerg Med. 1998 May-Jun;16(3):413-7.
PubMed PMID: 9610969.
33. CalesRH, Humphreys N, Pilmanis AA, et al. Cardiac arrest from gas embolism in scuba diving.Ann Emerg Med. 10:539 1981
34. Smith RM, Van Hoesen KB, Neuman TS. Arterial gas embolism and hemoconcentration. J Emerg Med. 1994 Mar-Apr;12(2):147-53. PubMed PMID: 8207148
35. Smith RM, Neuman TS. Elevation of serum creatine kinase in divers with arterial gas embolization. N Engl J Med. 1994 Jan 6;330(1):19-24. PubMed PMID: 8259140.
36. PearsonRR, GoadRF. Delayed cerebral edema complicating cerebral arterial gas embolism: case histories. UnderseaBiomedRes. 9:283 1982 PubMed PMID: 7168093
37.Ward CA, McCullough D, Yee D, et al. Complement activation involvement in decompression sickness of rabbits.Undersea Biomed Res. 17:51 1990 2316060
38. Thom SR, Yang M, Bhopale VM, et al. Microparticles initiate decompression-induced neutrophil activation and subsequent vascular injuries.J Appl Physiol.110:340 2011 20966192
39. ThomSR, BennettM, BanhamND, et al. Association of microparticles and neutrophil activation with decompression sickness.J Appl Physiol. 119 (5):427-4342015 26139218
40. HillsBA, JamesPB. Microbubble damage to the blood-brain barrier: Relevance to decompression sickness. Undersea Biomed Res. 18:111 1991 2042262
41. Obad A, et al. Successive Deep Dives Impair Endothelial Function and Enhance Oxidative Stress in Man. Clinical Physiology and Functional Imaging, U.S. National Library of Medicine, Nov. 2010. PubMed PMID 20718805.
42. Divers Alert Network. Signs and Symptoms of DCS. Divers Alert Network, www.diversalertnetwork.org/health/decompression/Signs-and-symptoms-of-DCS.
43. RudgeFW, StoneJA. The use of the pressure cuff test in the diagnosis of decompression sickness.Aviat Space Environ Med. 62:266 1991 2012577.
44. GilliamB. Demystifying Recompression Chambers. Divers Blogs, 27 Nov. 2009, www.undercurrent.org/blog/2009/11/27/recompression-chambers/.
45. ChryssanthouCP.Dysbaric osteonecrosis.Clin Orthop. 130:94 1978
46. Hunter Jr WL, BiersnerRS, Sphar RL, et al. Aseptic bone necrosis among U.S. Navy divers: Survey of 934 randomly selected personnel. Undersea Biomed Res. 5:25 1978 PubMed PMID 636072
47. Livingstone DM, Smith KA, Lange B. Scuba diving and otology: a systematic
review with recommendations on diagnosis, treatment and post-operative care.
Diving Hyperb Med. 2017 Jun;47(2):97-109. Review. PubMed PMID: 28641322
48. Shupak A, Gil A, Nachum Z, Miller S, Gordon CR, Tal D. Inner ear decompression sickness and inner ear barotrauma in recreational divers: a long-term follow-up. Laryngoscope. 2003;113:2141-7.
49. Talmi YP, Finkelstein Y, Zohar Y. Decompression sickness induced hearing loss. A review. Scand Audiol. 1991;20:25-8.
50. FrancisTJR, PezeshkpourGH, DutkaAJ, et al. Is there a role for the autochthonous bubble in the pathogenesis of spinal cord decompression sickness? J Neuropathol Exp Neurol. 198847:475
51. Aharon-Peretz J, Adir Y, Gordon CR, Kol S, Gal N, Melamed Y. Spinal cord
decompression sickness in sport diving. Arch Neurol. 1993 Jul;50(7):753-6.
52.Dick APK, MasseyEW. Neurological presentation of decompression sickness and air embolism in sport divers. Neurology. 35:667.
53. HodgsonM, BeranRG, ShirtleyG. The role of computed tomography in the assessment of neurologic sequelae of decompression sickness. Arch Neurol. 45:1033 1988 3415521.
54.GemppE, et al. “MRI Findings and Clinical Outcome in 45 Divers with Spinal Cord Decompression Sickness.” Aviation, Space, and Environmental Medicine, U.S. National Library of Medicine, Dec. 2008, PMID: 19070307.
55. Pneumomediastinum. Case courtesy of Dr Derek Smith, <a href=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/39652″>rID: 39652</a>
56. Pneumothorax
Case courtesy of Dr Andrew Dixon, <a href=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/48365″>rID: 48365</a>





1 thought on ““Twenty Thousand Leagues Under the ED”: Common Diving Emergencies”
Pingback: Weekend Knowledge Dump- September 27, 2019 | Active Response Training