
Author: Zachary Aust, MD (Assistant Professor of EM/Attending Physician, UTSW – Dallas, TX) // Reviewed by: Andy Grock, MD; Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case:
A 34-year-old female presents to the emergency department due to a high heart rate. She noticed that her heart rate has been averaging 110 bpm on her smart watch monitor for the last 2 days. She denies any additional symptoms, no chest pain, shortness of breath. She denies any recent travel, no URI symptoms. She denies any medical problems, previous surgeries or being on any medications including OCPs. She denies any history of smoking, alcohol or drug abuse. On exam vitals show a regular rate and rhythm at 110 bpm, blood pressure is 120/70, respirations are 12, pulse ox is 100% on room air, and she is afebrile. Heart and lung exam is normal, other than the tachycardia. There is no abdominal tenderness. She is able to ambulate without change in vitals or symptoms. Labs show a normal CBC, CMP, TSH, Negative HCG. EKG shows sinus tachycardia at a rate of 110bpm. She is given 1L of IVF without change in vitals.
What additional history, exam or workup (if any) should be done? What is this patient’s disposition?
Early on in my residency training I remember one of my attendings, Dr. Raymond Fowler telling me one of the important rules of emergency medicine, “Always explain the tachycardia”. Elevated heart rate may be one of the first signs we recognize that something more insidious is wrong with the patient. When a patient in the emergency department has sinus tachycardia our job as emergency physicians is to identify and treat of the underlying pathology1-4. This is done with a HPI, review of systems, physical exam and as indicated further diagnostic studies1,2. The full differential diagnosis of sinus tachycardia in isolation is extensive ranging from benign etiologies such as anxiety to severely life threatening etiologies such as sepsis. Discharging a patient with abnormal vital signs has been linked to unanticipated death. One study when looking at a population of patients that had unexpected death within 7 days of ED discharge found that of those that had abnormal vital signs at time of discharge tachycardia was present in 83% of the cases4,5. Another study looking at patients with early death after being discharged from the ED found that tachycardia was the most common abnormal vital signs and that it tended to persist despite interventions5. However, another study looking at revisits in a pediatric population found that while tachycardia at discharge was independently associated with an increased risk in ED revisit rate (relative risk of 1.3), there was no clinically important intervention required at this revisit6.
What do we do, however, when we are not able to explain the tachycardia or the patient is not responding to treatment as expected? At this point there are two large questions.
#1. Am I missing anything?
#2. What is this patient’s disposition?
This article focuses on these two questions. The first part will look at a more systematic mental model to double check ourselves in the situation where we have an unexplained sinus tachycardia. This mental model will be for those few cases where the patient requires a second look, where no obvious cause has been found or the patient is not responding to treatment as expected. In these scenarios it is important for us to have a cognitive stop point to reevaluate. We should utilize a framework to systematically ensure we have fully evaluated and treated any possible underlying life threats4. The second part will examine the disposition of the patient with unexplained sinus tachycardia. While this question is a largely evidence free zone, I hope to give some guidance and possible solutions.
Background
In adults, sinus tachycardia is a heart rate greater than 100 beats per minute (bpm) originating from the sinoatrial (SA) node1-3,7. Pediatric rate cut off for tachycardia varies with age but again is defined as a heart rate great than what the normal appropriate resting heart rate for that particular age range, again originating from the SA node8. For the most part we will be referring to normal sinus tachycardia, which we encounter most often in the emergency department. Inappropriate sinus tachycardia is a different entity which will be discussed later1-3,7.
The differential diagnosis of sinus tachycardia is long. The elevation in heart rate may be normal under stress or during exercise3. Regarding emergent underlying causes, it may be helpful to think of etiologies of tachycardia as anything that could cause a need for increased cardiac output. This cardiac output increase is often due to need for increased oxygen delivery. Factors such as hypoxia, hemorrhage, or even fever can increase the demand of tissue for oxygen and thus lead to a compensatory increase in heart rate. Tachycardia may be present both from many medications or drugs. The removal of substances, causing a withdrawal state, is another etiology1- 3,7.
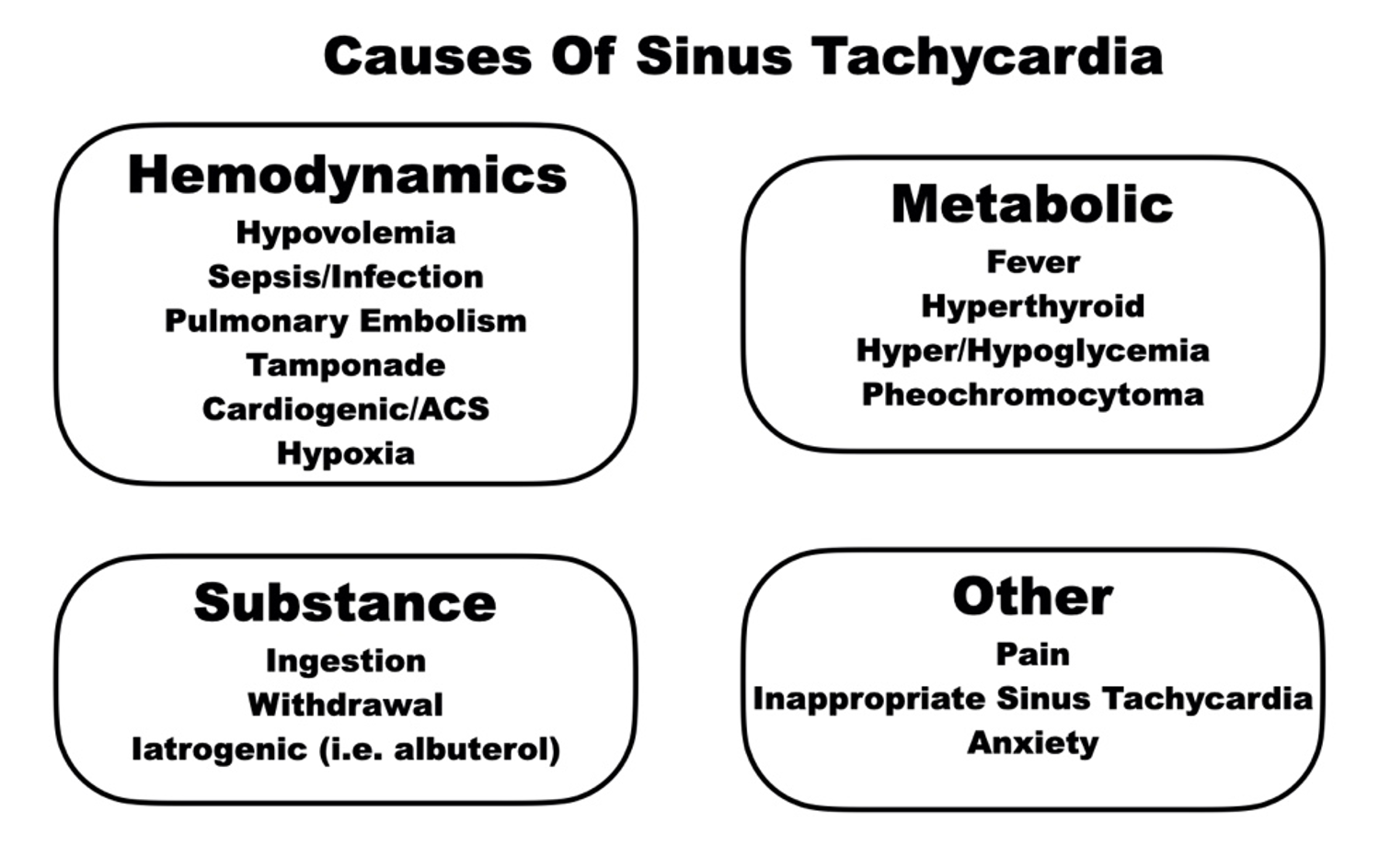
Many of these underlying etiologies may be obvious initially. A patient’s history and physical often will give us strong clues with additional evidence coming back on diagnostic workups. What I present here is not suggested for the initial evaluation as this would cognitively slow us. This is designed for the second look when the pieces do not fit together as they should. Here is the mental model in full, and while much of this happens in tandem, for sake of digestion it will be laid out in list format.

Vital Signs
Start with double checking vital signs. This prompts us to do a reassessment and evaluate where we are. Do they have any other explanation on their vitals that could contribute to the heart rate?
- Heart Rate
- Does the patient still have tachycardia?
- Has there been any change increase or decrease after intervention?
- Blood Pressure
- What is the patients blood pressure trend?
- Have they had any hypotension?
- Do they have a widened or narrowed pulse pressure?
- SPO2
- Any Hypoxia?
- Are we getting a good waveform on the SPO2?
- Poor waveforms more often indicate decreased perfusion than hypoxia.
- Respiratory Rate
- Temperature
- Do we have a recent and accurate temperate?
- A core temperature may be indicated.
- Glucose POC
- Do we have a recent and accurate temperate?
EKG
Then next question is: Is this actually sinus tachycardia? Looking at the initial or even repeating the EKG will be helpful here.
- QRS (wide/narrow)
- Regular/Irregular
In general sinus tachycardia should be regular and narrow complex (excluding having a bundle branch block), wide complex tachycardia should make you think Ventricular Tachycardia until proven otherwise.
- P waves?
- Are there p waves or is this possibly another SVT?
- Origin from SA node?
- Upright p waves in I, II, aVL
- Negative p waves aVR
- Flutter?
- Then ask are we missing another underlying arrhythmia such as Atrial Flutter. Think about this especially with the rate being consistently around 150 bpm (+/-20 bpm)
History
- Repeat ROS
- Infectious
- Cardiopulmonary
- Tox
- Ingestion or withdrawal
Have we done a comprehensive review of symptoms? Have we asked about any possible infectious etiologies for the patient’s symptoms? Is there any history of medications or substances that could be causing the tachycardia either from acute ingestion or withdrawal? Is the patient having any shortness of breath at rest or with exertion?
Physical Exam
Is there anything we have overlooked on physical exam? A more detailed exam may provide a clue to the underlying etiology.
- General
- On repeat assessment how does the patient generally appear, what is your overall gestalt?
- Cardiopulmonary
- Are there any abnormal sounds that may point to a diagnosis?
- Abdominal Tenderness?
- Neuro/Tox
- Pupils
- Clonus/Rigidity
- Reflexes
- All may help indicate another underlying cause such as toxic ingestion or withdrawal.
- Skin
- Diaphoretic/Dry?
- May point to Toxic or infectious etiology
- Infections/Wounds/Rashes
- Have we overlooked an infectious source?
- Axilla, Sacral, GU
- Overall Volume Status?
- Do they have edema?
- JVD?
- How are their mucous membranes?
- Diaphoretic/Dry?
POCUS
- RUSH Exam
My personal favorite way to assess for volume status is using point of care ultrasound (POCUS) which is the next part of our mental model. For this I believe doing the RUSH exam (Rapid Ultrasound for Shock and Hypotension) is a helpful framework. While it was derived to help identify unexplained hypotension, if we accept that sinus tachycardia may be an early indicator of shock, we can utilize this general approach to help reevaluate as clinically indicated.
Are there signs of pericardial effusion or tamponade? Are the ventricles normal sized? How is the cardiac squeeze? Any signs of fluid or PTX in the lungs? Does the IVC indicate to you that the patient is severely volume up or down. Any signs of AAA? Any signs of free fluid in the abdomen?
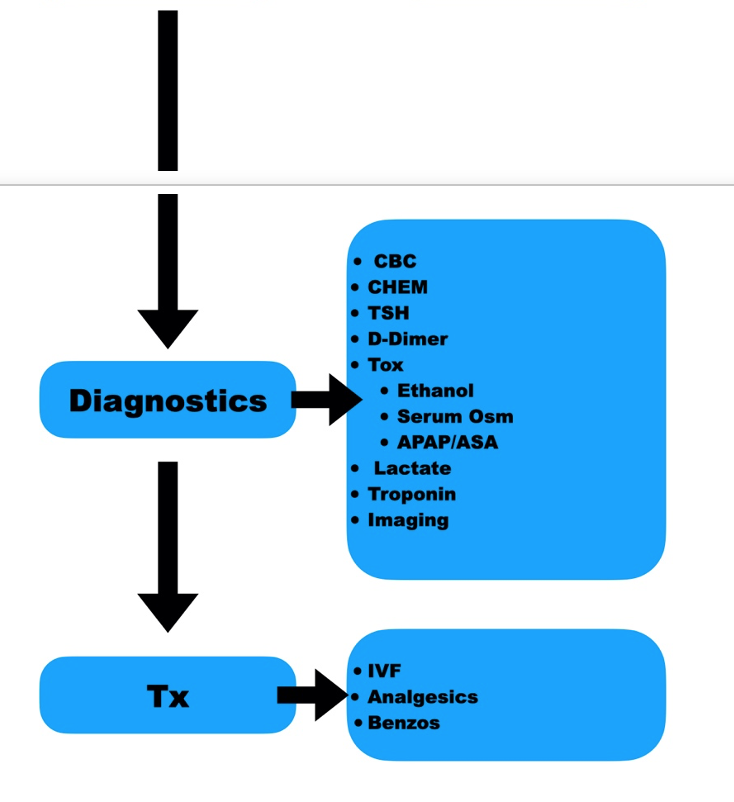
Diagnostics
Are there any laboratory abnormalities that either we overlooked or need to consider adding on?
- CBC
- Chem
- Have we fully elevated for anemia and electrolyte disturbances?
- TSH
- D-Dimer
- Is this patient low to intermediate risk for pulmonary embolism?
- Tox
- Ethanol
- ASA/APAP
- Serum Osm
- On repeat exam is there any more concern for toxic ingestion we may consider adding on APAP/ASA or looking for toxic alcohols.
- Lactate
- Troponin
- Could this be ACS or myocarditis?
- Is there additional imaging indicated?
This is not saying you should just blindly order all of these labs; we want to order them only when clinically indicated. These are listed here as a cognitive stop point: have we at least considered these possible life threats?
Treatments
Finally, have we adequately treated possible underlying causes?
- IVF
- Have we rehydrated as clinically indicated?
- Analgesia
- Have we provided adequate analgesia?
- Benzos
- Are they requiring benzodiazepines for withdrawal?
- Additional Resuscitation
- Have we addressed all potential sources of shock for the patient in front of us? Does the patient require blood, a procedure to address obstructive shock, or other source control?
- Iatrogenic
- Is it possible they weren’t tachycardia to begin with but we have given them something to stimulate the heart rate such as albuterol?
Utilizing this mental model provides a thorough approach to the patient with continued unexplained sinus tachycardia.
Disposition
What now for the patient who after all of this, still continues to have a high heart rate? This will obviously be very dependent on the scenario, but the elephant in the room we need to address is: can we discharge the patient in sinus tachycardia?
In short: yes, but it depends.
This is going to be variable based on providers risk tolerance, patient status and ability to follow up. Let’s use the example of the well appearing patient, without significant co morbidities. They may have presented due to palpitations or noticing their heart rate was elevated on a home monitoring device. In this case let us say we have a patient with either:
- Asymptomatic but persistent sinus tachycardia
- Sinus tachycardia with a found/treated underlying etiology that would otherwise not make you concerned for discharge if not for the heart rate.
There are other conditions such as inappropriate sinus tachycardia and sinus node reentry tachycardia that could be causing this2,3,7. It is not unreasonable to arrange for cardiology evaluation. Patients can develop a tachycardia-mediated cardiomyopathy from any tachyarrhythmia. Often the ventricular dysfunction from this is reversible. The risk seems to be greatest once reaching 110-120 bpm, the older the patient the higher likelihood they are at risk for this. The time course, however, does seem to take from a month to possibly years9. Given this fact, it may be reasonable to discharge if patient is able to get reliable cardiology follow up in a short period of time.
Pearls
- Sinus Tachycardia is often the first sign something more insidious is wrong with the patient.
- Tachycardia can be a response to anything that causes the body to have an increased oxygen demand, sympathetic stimulus, or withdrawal of a substance.
- In the ED, our job is to identify and treat underlying causes.
- When no cause is found, or the patient is not responding to treatment as expected, a more systematic mental model is needed.
- Disposition of sinus tachycardia depends on many factors, however the well-appearing asymptomatic patient does not require admission for tachycardia alone.
#FOAMED
- http://www.emdocs.net/r-e-b-e-l-em-the-approach-to-the-most-common-cardiac-dysrhythmia-8-causes-of-sinus-tachycardia/
- https://www.aliem.com/paucis-verbis-an-approach-to-persistent-tachycardia/
- https://ddxof.com/sinus-tachycardia/
References
1) Henning A, Krawiec C. Sinus Tachycardia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; April 30, 2022.
2) Yusuf S, Camm AJ. Deciphering the sinus tachycardias. Clin Cardiol. 2005;28(6):267-276. doi:10.1002/clc.4960280603
3) Yusuf S, Camm AJ. The sinus tachycardias. Nat Clin Pract Cardiovasc Med. 2005;2(1):44-52. doi:10.1038/ncpcardio0068
4) Sklar DP, Crandall CS, Loeliger E, Edmunds K, Paul I, Helitzer DL. Unanticipated death after discharge home from the emergency department. Ann Emerg Med. 2007;49(6):735-745. doi:10.1016/j.annemergmed.2006.11.018
5) Gabayan GZ, Sun BC, Asch SM, et al. Qualitative factors in patients who die shortly after emergency department discharge. Acad Emerg Med. 2013;20(8):778-785. doi:10.1111/acem.12181
6) Wilson PM, Florin TA, Huang G, Fenchel M, Mittiga MR. Is Tachycardia at Discharge From the Pediatric Emergency Department a Cause for Concern? A Nonconcurrent Cohort Study. Ann Emerg Med. 2017;70(3):268-276.e2. doi:10.1016/j.annemergmed.2016.12.010
7) Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia: The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC) [published correction appears in Eur Heart J. 2020 Nov 21;41(44):4258]. Eur Heart J. 2020;41(5):655-720. doi:10.1093/eurheartj/ehz467
8) Fleming S, Thompson M, Stevens R, et al. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet. 2011;377(9770):1011-1018. doi:10.1016/S0140-6736(10)62226-X
9) Kim DY, Kim SH, Ryu KH. Tachycardia induced Cardiomyopathy. Korean Circ J. 2019;49(9):808-817. doi:10.4070/kcj.2019.0199




