
US Probe: Serratus Anterior Block
When, how, and why should you perform the serratus anterior block?
US Probe: Serratus Anterior Block Read More »
When, how, and why should you perform the serratus anterior block?
US Probe: Serratus Anterior Block Read More »

How can you use POCUS to evaluate for necrotizing soft tissue infection?
POCUS Diagnosis of NSTI Read More »
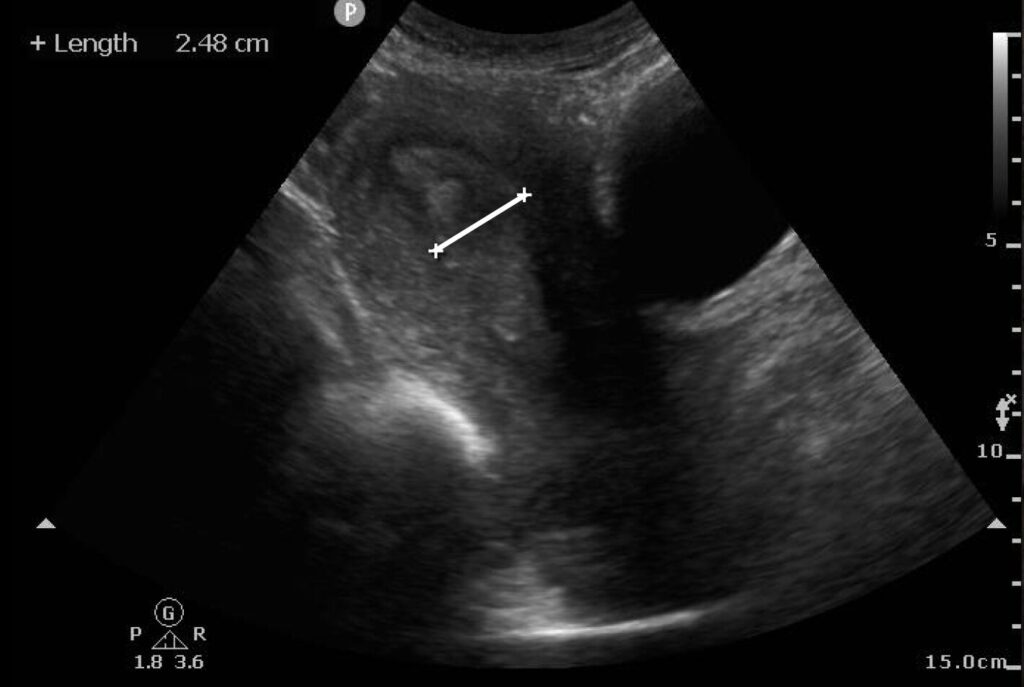
How can you use POCUS to evaluate for retained products of conception?
Point-of-Care Ultrasound for Recognizing Retained Products of Conception Read More »

How can you estimate LV function using ultrasound?
US Probe: Left Ventricular Ejection Fraction Semi-Quantitative Estimation Read More »

When should you consider an ultrasound guided erector spinae plane block, and how do you perform it?
Ultrasound Guided Erector Spinae Plane Block Read More »

How can you use POCUS to diagnose upper extremity DVT?
US Probe: Upper Extremity DVT Read More »

Author: Louisa Weindruch, DO (Baylor University Medical Center), Allison Harmsworth Smith, MD (Baylor University Medical Center), Chase Forehand, MD (Baylor University Medical Center), Jonathan Brewer, MD, FACEP, FPD-AEMUS (Baylor University Medical Center), and Whitney Potomac, DO, MS, FACEP, FPD-AEMUS // Reviewed By: Jonathan Warren, MD; Steve Field, DO; Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) History of Present Illness: An eight-year-old female with no significant past medical history presented with her parents to a local emergency department (ED) with left wrist pain after falling from monkey bars onto an outstretched hand. She was given over-the-counter pain medication at home with minimal relief. She continued to report left wrist pain and swelling, prompting the family to bring her to the ED for evaluation. She was otherwise at her baseline state of health. Physical Exam: Vital signs included a blood pressure of 114/98 mmHg, heart rate of 114 beats per minute, temperature of 99.1 degrees Fahrenheit, respiratory rate of 22 breaths per minute, and SpO2 99% on room air. On physical exam, the patient was overall well-appearing and in no acute distress. She had swelling and tenderness to palpation over the left distal radius with no evidence of open wounds. Sensation was intact to light touch along the radial, median, and ulnar distributions. She had a 2+ radial pulse and brisk capillary refill. She had pain with movement and limited range of motion of her wrist, however motor function of the radial, median, and ulnar nerves was grossly preserved. Point-of-Care Ultrasound: Point-of-Care Ultrasound (POCUS) of the left distal radius was performed. A linear probe was placed over where the patient had maximum area of point tenderness. POCUS revealed disruption of the hyperechoic bony cortex concerning for an acute fracture (Figure 1 and 2). Figure 1: Sagittal View of Fracture with Surrounding Hematoma. White arrow points to area of cortical bone disruption consistent with fracture. Figure 2: Transverse view of fracture. White arrow points to area of cortical bone disruption consistent with fracture. Diagnostic Imaging: A three-view x-ray of the left wrist was obtained and revealed non-displaced fractures to the left distal radius and left distal ulna. No additional workup was completed. Figure 4a: Lateral X-Ray, Fractures of Distal Radius and Ulna. Arrow points to an area of cortical bone disruption consistent with fracture. 4b: Anterior Posterior X-Ray, Fractures of Distal Radius and Ulna How To Perform: When obtaining images of musculoskeletal structures with POCUS, a linear probe is the ideal probe to use. Its higher frequency allows for easy identification of highly reflective, shallow structures. Bone will appear as a well-defined, hyperechoic line with posterior shadowing on sonographic imaging. We propose utilizing a 6-view protocol, as described in Snelling et. al. The POCUS operator uses the linear probe to visualize the radius in 3 views (dorsal, volar, and medial) and ulna in 3 views (dorsal, volar, and lateral)[1,2]. With the indicator oriented distally, the operator scans proximally and distally in the longitudinal axis to evaluate the bony cortex, looking for any deformities that would suggest a fracture. Discussion: Forearm fractures are the most common fracture in the pediatric population, making up 25% of all pediatric fractures, and are frequently seen in emergency departments worldwide [3]. While x-ray has previously been the standard diagnostic test, in recent years evidence has emerged suggesting POCUS may be used as an adjunct. Ultrasound is quick, cost effective, and can easily be performed at bedside. It provides no additional ionizing radiation, an important consideration in pediatric emergency medicine. Additionally, with increased accessibility of handheld probes, ultrasound has also become an important diagnostic tool in resource-limited and austere environments. There are many advantages to performing POCUS for suspected fractures in children. The interface between bones and the surrounding soft tissue is highly reflective of sound waves, making ultrasound an ideal modality for imaging fractures [4]. Using a linear probe, the operator can easily visualize the hyperechoic bony cortex and evaluate for any cortical abnormalities [4]. In addition to cortical disruptions, literature suggests that there may be other secondary signs to indicate a distal radius fracture, such as a pronator quadratus hematoma or periosteal hematoma [5,6]. A systematic review of 23 studies with over 3,000 children found that ultrasound is both sensitive and specific for identifying forearm fractures [4]. In this review, sensitivity ranged from 91.5% to 100% with the majority of studies achieving sensitivity >95%. Specificity ranged from 84% to 100% [4]. In a similar systematic review of 7 studies, authors found that in the United States, sensitivity ranged from 85% to 100% and specificity ranged from 73% to 100% [7]. They were ultimately able to conclude that the overall accuracy of ultrasound in diagnosing fractures was between 78.6% to 99.5% [7]. Morello et. al also found that ultrasound decreased length of stay in emergency departments, with an ultrasound-first approach shortening the stay by an average of 15 minutes [4]. This is particularly relevant as many emergency departments continue to face long wait times and boarding crises. In another study, patients had fewer missed days of school over a 4 week period compared to the radiographic group [8]. Lastly, 7 of the 23 studies looked at patient discomfort during POCUS and found that it was similar or even less than the pain experienced during x-ray [4]. It is worth noting that there was a broad range of clinicians – including emergency physicians, nurse practitioners, residents, and orthopedic surgeons – who received focused training in performing POCUS for this indication. This highlights the potential for POCUS to be taught to a variety of different clinicians who may evaluate patients within the emergency department. Notably, some of the strongest data for the use of POCUS in pediatric fractures comes from a randomized-controlled trial out of Australia where 270 children ages 5-15 years old presented with suspected forearm fractures [2]. Utilizing a panel of expert clinicians including emergency physicians, orthopedic surgeons, and radiologists as the reference standard with clinical longitudinal follow-up, POCUS was found to outperform x-ray for
US Probe: POCUS for the Diagnosis of Acute Pediatric Distal Radius Fractures Read More »
How can you use Velocity Time Integral (VTI) for the evaluation and management of sepsis?
US Probe: Velocity Time Integral (VTI) in Sepsis Management Read More »

What is the VExUS Approach to evaluating for venous congestion?
US Probe: Assessing Venous Congestion – The VExUS Approach Read More »
How do you handle US artifacts?
US Probe: An Abundance of Artifacts Read More »