Authors: Cosby Arnold, MD, MPH (EM Resident Physician, University of Tennessee at Memphis) and Mark Brady, MD, MPH (Affiliate Assistant Professor, Department of Emergency Medicine, University of Tennessee at Memphis) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
A 61-year-old man presents to the Emergency Department with severe headache and left arm and leg weakness. He states the headache began a few hours ago. It was initially mild but has become progressively worse while he has been working at his desk job. Past medical history is significant for uncontrolled hypertension. Vital signs are: HR 90, RR 10, BP 215/110, T 99º F. Physical exam reveals decreased left-sided grip strength and inability to lift his left leg without assistance. The remainder of his neurological exam is normal.
Background
Intracranial hemorrhage (ICH) is the second most common cause of stroke, accounting for 10 to 15% of all acute strokes and affecting about 65,000 patients per year.1 Long-standing hypertension, resulting in hypertensive vasculopathy, is the most significant risk factor.2 Other causes include cerebral amyloid angiopathy, underlying vascular malformations (including arteriovenous malformations (AVMs) and aneurysms), hemorrhagic infarction (including venous sinus thrombosis), septic or mycotic aneurysm, tumors, blood dyscrasias, hemorrhagic transformation of ischemic stroke, Moyamoya disease, and drug intoxication (particularly sympathomimetics, such as cocaine and amphetamines).3
How does ICH present? Unlike subarachnoid hemorrhage, symptoms are not classically maximal at onset. Headache and nausea/ vomiting only occur in about half of cases, and when they do they are typically gradual in onset rather than “thunderclap.” Patients with ICH may present identically to those with ischemic stroke, and these two processes cannot be reliably differentiated from each other without imaging.
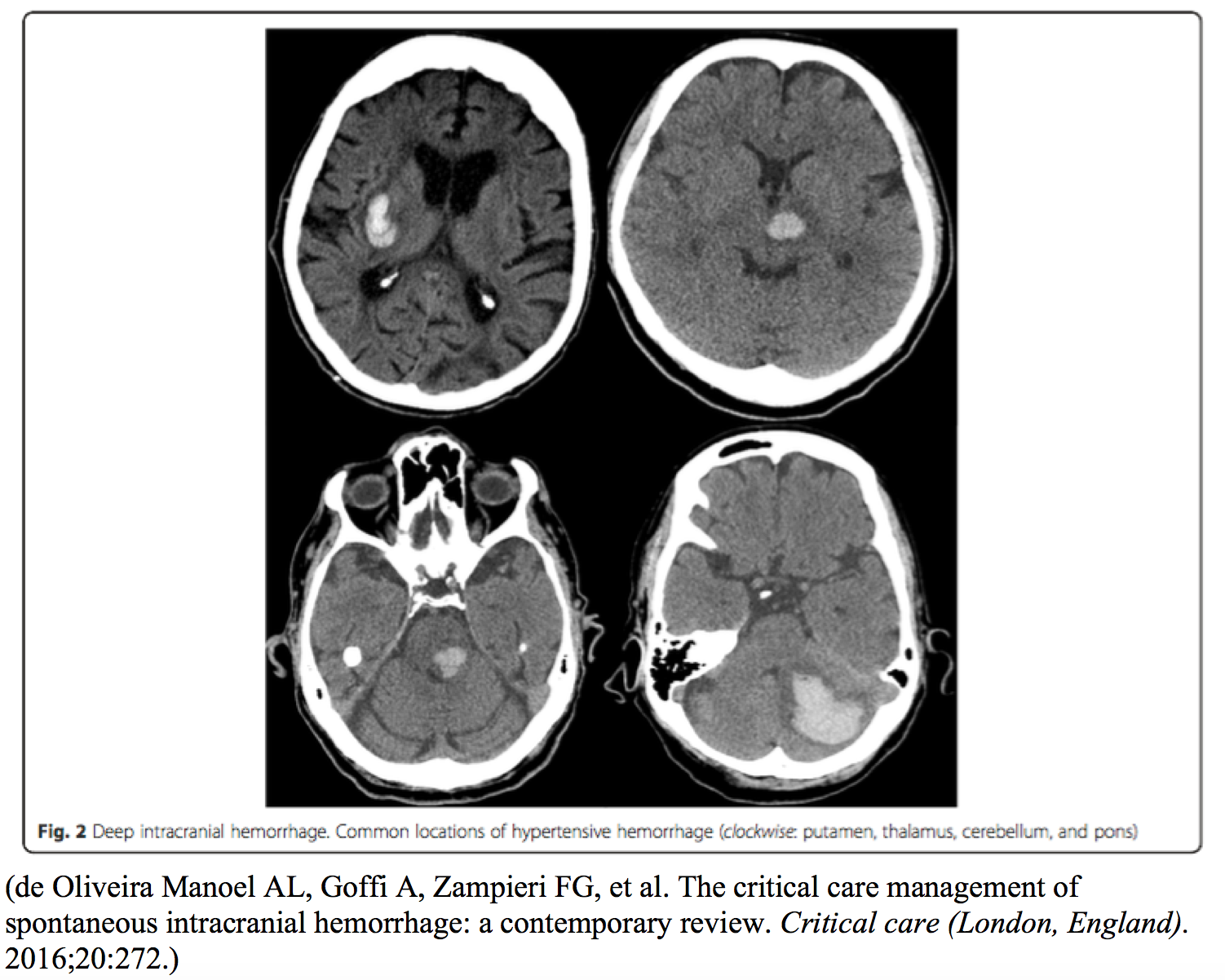
Neurologic signs reflect hemorrhage location (Table 1). Bleeding into the putamen is the most common, followed by the subcortex, cerebellum, thalamus, and pons.1,3
Table 1. Clinical presentation corresponding to intracranial hemorrhage location
| Putamen | Hemiplegia, hemisensory loss, homonymous hemianopsia, gaze palsy, stupor, coma |
| Cerebellum | Gait imbalance, vomiting, headache, neck stiffness, gaze palsy, facial weakness |
| Thalamus | Hemiplegia, hemisensory loss, transient homonymous hemianopsia, aphasia or neglect, upgaze palsy with miotic unreactive pupils that look toward tip of nose, are skewed, or point toward the weak side |
| Pons | Total paralysis, pinpoint reactive pupils, absent horizontal eye movements, deep coma within minutes of onset |
| Subcortex | Most commonly affect parietal (contralateral lower extremity hemiplegia) or occipital (contralateral homonymous hemianopsia) lobe; highest incidence of seizure |
Differential
The differential diagnosis for ICH is broad and includes:
- Migraine
- Seizure
- Bell’s palsy
- Labyrinthitis
- Vestibular neuronitis
- Peripheral nerve palsy
- Demyelinating diseases
- Meniere’s disease
- Giant cell arteritis
- Tumor
- Abscess
- Hypertensive encephalopathy
- Ischemic stroke
- Subarachnoid hemorrhage
- Cavernous sinus thrombosis
- Carotid or aortic dissection
- Air embolism
- Metabolic abnormalities
- Trauma
Diagnosis
While the history and clinical findings may suggest the diagnosis of ICH, imaging is required for confirmation. Either CT or MRI can detect ICH,4,5 but noncontrast head CT is faster and is the usual initial imaging modality in the ED. CT can demonstrate hemorrhage size and location, extension into the ventricles, surrounding edema, and herniation. Density is inversely related to timing of the bleed, with chronic blood appearing hypodense on CT. A patchy appearance of hyperdensity with a larger area of iso- or hypodensity suggests hemorrhagic transformation of ischemic stroke. MRI is superior for evaluating for underlying structural malformations. Alternatively, CT angiography or conventional angiography are useful adjuncts to demonstrate underlying macrovascular causes.6
The optimal approach to exclude ICH with a normal noncontrast head CT is debatable. The sensitivity of noncontrast head CT is inversely proportional to the time from onset of symptoms. Options for further studies include lumbar puncture, CTA, or MRI/ MRA. It is prudent to document whether a patient declines further workup if there is an unremarkable noncontrast CT head.7 You can read more about the controversies here: http://www.emdocs.net/controversies-in-the-diagnosis-of-subarachnoid-hemorrhage/.
Obtain platelet count, prothrombin time, and partial thromboplastin time to evaluate for bleeding disorders in all patients with ICH. A drug screen to evaluate for sympathomimetic use may be performed in patients in whom substance abuse is suspected. Underlying vascular malformations are relatively common in patients with ICH after cocaine use and require vascular imaging (e.g., CTA, MRA, angiography) for detection.
Management
All patients with ICH require ICU admission and neurosurgery consult for possible surgical intervention. These patients are at especially high risk of deterioration in mental status requiring endotracheal intubation. Short-acting sedatives are advisable in intubated patients to facilitate serial neurological examinations. Treat hyperthermia with antipyretics, titrate insulin dosing to maintain a target serum glucose level to avoid both hyper- and hypoglycemia (optimal glucose level is not agreed upon), administer antiepileptics if seizure occurs, and keep the head of the bed elevated 30 degrees to decrease intracranial pressure. Discontinue all anticoagulant and antiplatelet drugs, and administer appropriate agents for anticoagulant reversal.6
Blood pressure control after ICH is controversial. Hypertension may exacerbate bleeding, but an elevated mean arterial pressure (MAP) may be required to maintain cerebral blood flow (CBF) in patients who are chronically hypertensive.8 The INTERACT II trial found that patients randomly assigned to rapid reduction in blood pressure to <140 mm Hg within 1 hour demonstrated better functional outcomes when compared to those patients who underwent traditional management of target systolic blood pressure <180 mm Hg; however, there was no significant difference in rate of mortality or disability between the two groups.9 The ATACH II trial, just released in 2016, found no difference in death, disability, or hematoma size when targeting systolic blood pressure of 110-139 mm Hg or 140-179 mm Hg.10 Of note, investigators used nicardipine for BP lowering.10 Several agents can be used for BP control. For proper use of nicardipine, please see http://emcrit.org/wp-content/uploads/2014/07/bolus-dose-nicardipine.pdf. Labetalol is another option. Current guidelines for managing hypertension in ICH patients are presented in Table 2.6
Table 2. Management of hypertension in ICH
| SBP 150-220 mm Hg | Aggressive lowering to SBP <140 mm Hg is safe |
| SBP >220 mm Hg | Aggressive lowering to SBP < 140 mm Hg may be reasonable, but fewer data are available regarding safety and efficacy |
Current guidelines recommend IV fosphenytoin or phenytoin as the first-line anti-epileptic drug in the treatment of seizure; prophylactic use of anti-epileptic drugs may be harmful and is not recommended by current AHA ICH guidelines.3,6
Medical measures to reduce ICP in patients with clinical or radiographic findings suggestive of elevated ICP include elevating the head of the bed to 30 degrees and appropriate analgesia and sedation. Recommended IV sedatives include propofol, etomidate, or midazolam; morphine or alfentanil are recommended for analgesia. Fentanyl is an option as well. Normal saline is considered the fluid of choice; hypotonic fluids are contraindicated due to risk of cerebral edema. Mannitol is the treatment of choice to lower ICP. Hypertonic saline may be used as an adjunct or alternative. Hyperventilation may dramatically lower ICP, but the effect only lasts minutes to hours. This approach may be utilized in the interim until definitive treatment.
Pearls
- Imaging needs to be considered in all patients with undifferentiated headache because ICH often has an indolent presentation
- Follow-up angiography to determine source of bleed
- Control blood pressure and reverse anticoagulation in conjunction with local standard of care
Pitfalls
- Failure to obtain imaging in a patient with atypical presentation of cerebral bleed (e.g., gradual onset headache)
- With a normal noncontrast head CT, consider LP and further neuroimaging; if you do not pursue further testing document that a patient declines further workup or that in your judgment the risk is greater than benefit of further workup for ICH
References / Further Reading
- Marx J, Hockberger R, Walls R. Rosens Emergency Medicine Concepts and Clinical Practice. Philadelphia: Mosby/Elsevier; 2013.
- Woo D, Sauerbeck LR, Kissela BM, et al. Genetic and environmental risk factors for intracerebral hemorrhage: preliminary results of a population-based study. Stroke; a journal of cerebral circulation. 2002;33(5):1190-1195.
- de Oliveira Manoel AL, Goffi A, Zampieri FG, et al. The critical care management of spontaneous intracranial hemorrhage: a contemporary review. Critical care (London, England). 2016;20:272.
- Kidwell CS, Wintermark M. Imaging of intracranial haemorrhage. The Lancet Neurology. 2008;7(3):256-267.
- Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM. Tintinalli’s Emergency Medicine A Comprehensive Study Guide. New York: McGraw Hill; 2016.
- Hemphill JC, 3rd, Greenberg SM, Anderson CS, et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke; a journal of cerebral circulation. 2015;46(7):2032-2060.
- Farzad A, Radin B, Oh JS, et al. Emergency diagnosis of subarachnoid hemorrhage: an evidence-based debate. The Journal of emergency medicine. 2013;44(5):1045-1053.
- Garg RK, Liebling SM, Maas MB, Nemeth AJ, Russell EJ, Naidech AM. Blood pressure reduction, decreased diffusion on MRI, and outcomes after intracerebral hemorrhage. Stroke; a journal of cerebral circulation. 2012;43(1):67-71.
- Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. The New England journal of medicine. 2013;368(25):2355-2365.
- Qreshi et al. Intensive Blood-Pressure Lowering in Patients with Acute Cerebral Hemorrhage. New England journal of medicine. 2016;375:1033-1043.





1 thought on “Critical Intracranial Hemorrhage: Pearls and Pitfalls in Evaluation and Management”
Pingback: emDOCs.net – Emergency Medicine EducationEM Educator Series: Not all head bleeds are alike – Spontaneous Intracerebral Hemorrhage - emDOCs.net - Emergency Medicine Education