
Author: Richard J. Cunningham, MD (@HappyDays_EM, EM Resident Physician, Creighton/Maricopa Emergency Medicine Residency, Phoenix, AZ) // Reviewed by: Alex Koyfman, MD @EMHighAK) and Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
An 8-year-old male presents after falling onto an outstretched hand. He has an obvious dinner fork deformity to the right forearm. He is neurovascularly intact, and x-ray confirms a fracture of the distal radius and ulna. You prepare for procedural sedation with ketamine while you reduce and splint the fracture. You run through the pre-sedation assessment and exam, then gather all medications and airway supplies. You warn them to administer the ketamine slowly in order to avoid adverse side effects. However, once the ketamine is pushed you hear a high-pitched stridor and see the patient’s chest rise and fall irregularly as his oxygen saturation drops. While you’ve read about this dreaded effect of ketamine, this is your first time encountering it.
What is the diagnosis and management?
Answer: Laryngospasm
Epidemiology:
- Vagally-mediated involuntary closure of the vocal folds
- High incidence with extubation after general anesthesia (0.78-5%)1, though most commonly associated with ketamine use in the Emergency Department (ED)
- Large doses and rapid administration increase risk
- Incidence of 4.2 per 1000 among patients undergoing procedural sedation in the emergency department2
- Risk higher with airway manipulation, recent upper respiratory infection, and pediatric patients3
- However, case-control series found no association of ketamine-induced laryngospasm with age, dose, oropharyngeal procedure, underlying physical illness, route, or co-administration with anticholinergics4
- Can lead to aspiration, hypoxia, post-obstructive pulmonary edema, and cardiac arrest1
Clinical Presentation:
- Partial obstruction may present as stridor, tracheal tugging, and paradoxical chest movement
- Complete obstruction will present with apnea and no end-tidal CO2 waveform
- Up to 23% of laryngospasm may not be clinically obvious, and 61% can result in oxygen desaturation1
- Pediatric patients are at particular risk of developing bradycardia as a result of hypoxia
Evaluation and Treatment:
- Laryngospasm is a clinical diagnosis that requires prompt recognition and treatment
- Use the following stepwise approach:
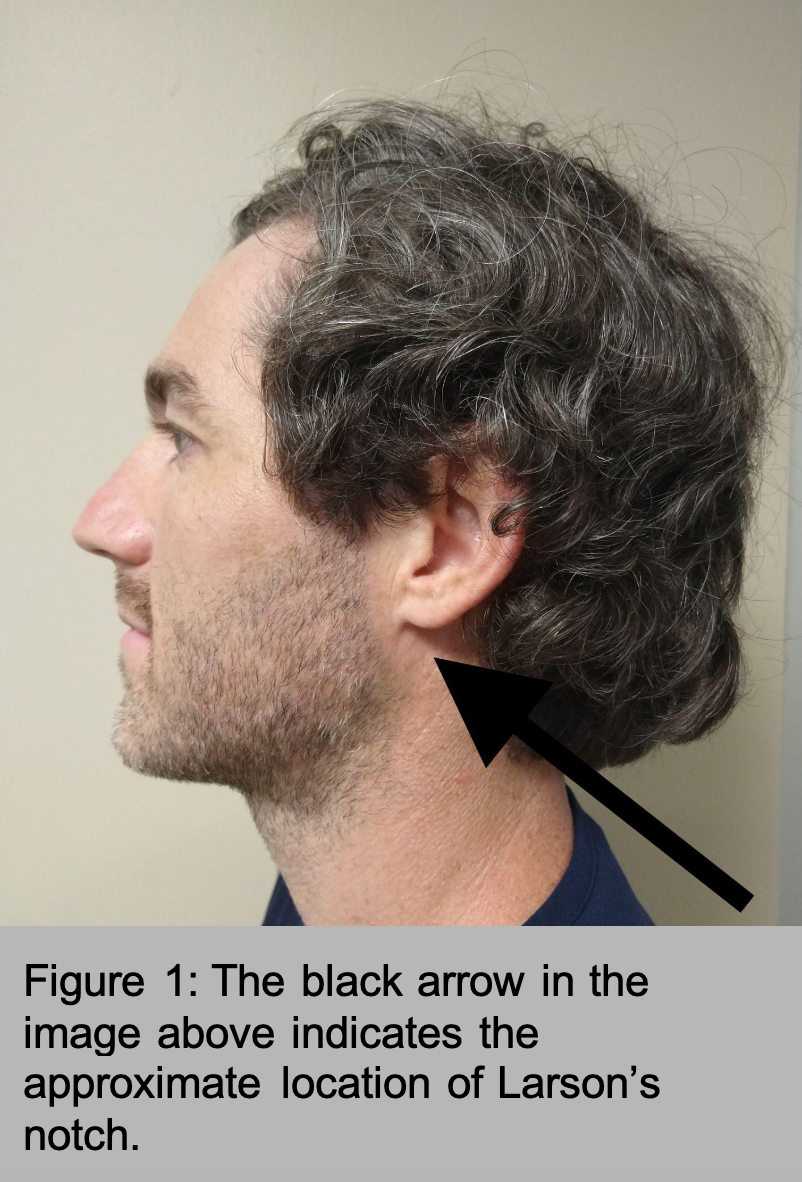
- Perform jaw thrust with pressure applied posterior to the ramus of the mandible and anterior to the mastoid process at Larson’s notch5 (Figure 1)
- Administer 100% FiO2 positive pressure ventilation via BVM with PEEP valve
- If these do not correct laryngospasm, propofol can be administered, followed by succinylcholine if laryngospasm is not relieved, but be prepared for endotracheal intubation
- Propofol 0.5 mg/kg IV can deepen sedation and result in muscle relaxation, breaking the laryngospasm
- While this strategy is common in the OR, many emergency physicians would feel uncomfortable giving these agents to a patient with an unprotected airway; proceeding to RSI may be more prudent
- Succinylcholine 0.5 mg/kg may break laryngospasm without causing full paralysis, thereby avoiding need for intubation.
- Doses as low as 0.1 mg/kg may be successful3
- This can be attempted if propofol not effective
- If no IV access, can give 4mg/kg IM; will break laryngospasm in 45 seconds to 1 min and lead to full paralysis in 3-4 min, but this requires intubation6
- If above measures fail, perform rapid sequence intubation (RSI)
- Propofol 0.5 mg/kg IV can deepen sedation and result in muscle relaxation, breaking the laryngospasm
- One small study performed in the OR showed gentle chest compression to be more successful than positive pressure ventilation in breaking laryngospasm (73.9% vs 38.4%, p<0001)7
Disposition:
- Patients will likely require a several-hour period of observation in the ED before discharge to monitor for signs of aspiration or post-obstructive pulmonary edema
- If intubated, attempt extubation with anesthesia present as there is a risk of recurrence
Pearls:
- Laryngospasm is a clinical diagnosis that requires prompt recognition and treatment to avoid morbidity and mortality
- Laryngospasm is most commonly associated with ketamine use in the ED
- It can present as stridor and respiratory distress or apnea depending on degree of obstruction
- To treat, perform a jaw thrust while applying pressure at Larson’s point and administering positive pressure via BVM
- If above fails, RSI will likely be required
Further Reading:
emDOCs: 10 Procedural Sedation Errors in the Emergency Department
5 Minute Airway: Beating Laryngospasm
First 10 EM: Managing laryngospasm
References:
- Visvanathan T, Kluger MT, Webb RK, Westhorpe RN. Crisis management during anaesthesia: laryngospasm. Qual Saf Health Care. 2005;14(3):e3. doi:10.1136/qshc.2002.004275
- Bellolio MF, Gilani WI, Barrionuevo P, et al. Incidence of Adverse Events in Adults Undergoing Procedural Sedation in the Emergency Department: A Systematic Review and Meta-analysis. Acad Emerg Med. 2016;23(2):119-134. doi:10.1111/acem.12875
- Hobaika AB, Lorentz MN. Laryngospasm. Rev Bras Anestesiol. 2009 Jul-Aug;59(4):487-95. PMID: 19669024.
- Green SM, Roback MG, Krauss B; Emergency Department Ketamine Meta-Analysis Study Group. Laryngospasm during emergency department ketamine sedation: a case-control study. Pediatr Emerg Care. 2010;26(11):798-802. doi:10.1097/PEC.0b013e3181fa8737
- Larson CP Jr. Laryngospasm–the best treatment. Anesthesiology. 1998;89(5):1293-1294. doi:10.1097/00000542-199811000-00056
- Gavel G, Walker RWM. Laryngospasm in anaesthesia. Contin Educ Anaesth Crit Care Pain. 2014; 14: 47–51.
- Al-Metwalli RR, Mowafi HA, Ismail SA. Gentle chest compression relieves extubation laryngospasm in children. J Anesth. 2010;24(6):854-857. doi:10.1007/s00540-010-1036-9




