Originally published on Ultrasound G.E.L. on 5/10/21 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from Ultrasound G.E.L. team!

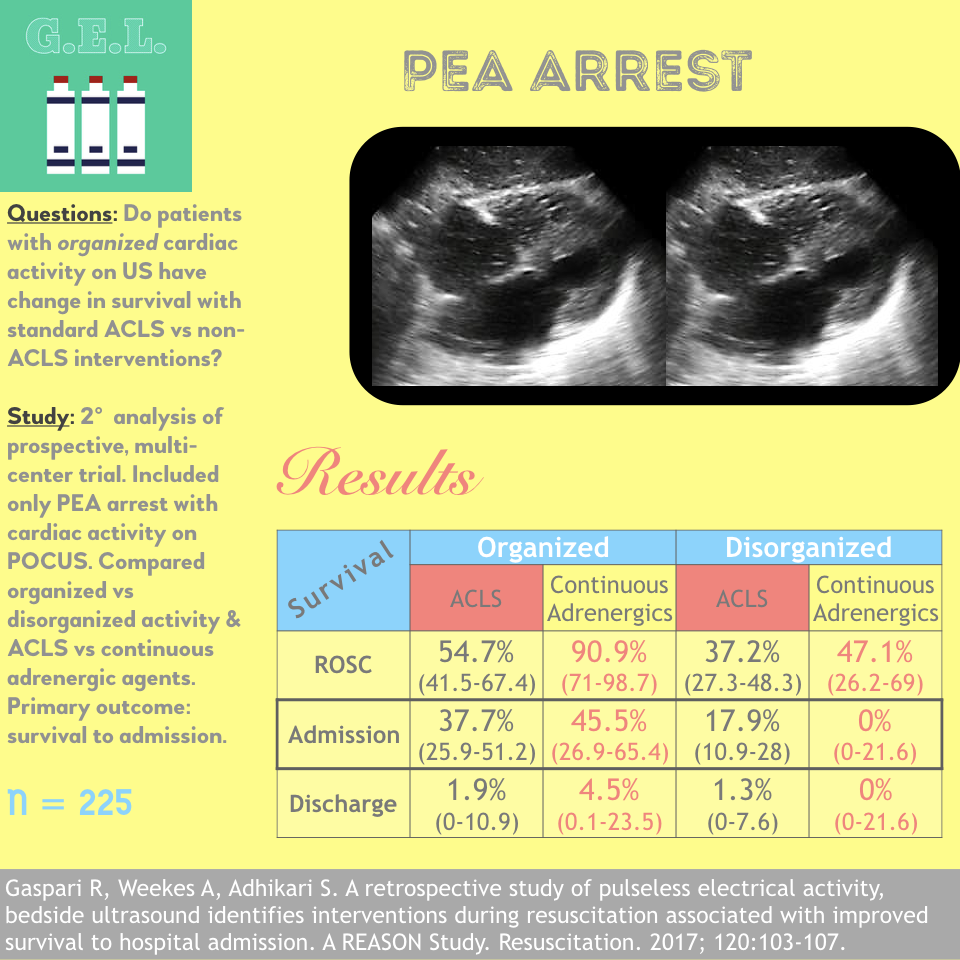
A retrospective study of pulseless electrical activity, bedside ultrasound identifies interventions during resuscitation associated with improved survival to hospital admission. A REASON Study
Resuscitation November 2017 – Pubmed Link
Take Home Points
1. Differentiating organized and disorganized cardiac activity with point of care ultrasound is feasible.
2. This distinction may influence survival and response to non-ACLS medications.
Background
There is still not enough known about exactly how we can (or should) use ultrasound in cardiac arrest. There have been studies that show ultrasound can be helpful in two main ways. First, the finding of cardiac activity on ultrasound is associated with increased survival. Secondly, ultrasound can identify causes for the arrest such as massive pulmonary embolism or cardiac tamponade. This paper is asking if we can take these purposes one step further. What if looking at the patients heart with ultrasound can help us figure out what medications will help them best during arrest? The distinction they make is between those with organized cardiac activity on ultrasound compared to those with disorganized activity (some movement but not really meaningful). They take a look at patients in PEA (pulseless electrical activity) and determine if those with organized cardiac activity would have increased survival after certain interventions.
Questions
Does the finding of organized cardiac activity on point of care ultrasound identify a population that would have a change in survival from particular interventions given during cardiac arrest? In other words, do patients with organized cardiac activity benefit more (or less) from certain medications.
Population
Real-time Evaluation and Assessment Sonography Outcomes Network (REASON)
20 sites in US and Canada
Inclusion:
- Presenting to emergency department in cardiac arrest
- Advanced cardiac life support (ACLS) employed
- PEA as initial rhythm on presentation to ED (note that the original study included both PEA and asystole)
- Ultrasound performed during cardiac arrest
Exclusion:
- No cardiac activity on initial ultrasound
Design
Secondary analysis of a prospective observational trial. See our previous post on the REASON trial for those methods.
Patients in PEA arrest were compared in four groups based on two binary characteristics:
- Organized cardiac activity + Received only standard ACLS medications
- Organized cardiac activity + Received non-ACLS medications
- Disorganized cardiac activity + Received only standard ACLS medications
- Disorganized cardiac activity + Received non-ACLS medications
Primary outcome was survival to hospital admission.
Secondary outcomes were ROSC (return of spontaneous circulation) and survival to hospital discharge.
Intervention
Categorized all interventions to patient during the arrest resuscitation as either:
- ACLS intervention
- Intervention outside of ACLS
Interventions only counted between resuscitation and return of spontaneous circulation (ROSC)
Initial ultrasound interpreted as binary cardiac activity or no cardiac activity.
Each clip was subsequently reviewed by two blinded interpreters who designated it as not only positive or negative for cardiac activity but determined for clip with activity, whether or not it was organized activity.
Important New Definition Alert!
The authors’ definition of Organized Cardiac Activity = movement of the myocardium with change in size of the ventricular cavity and synchronized movement of the ventricular wall.
Who did the ultrasounds?
Emergency Physicians credentialed in bedside US. No specific training noted.
The Scan
Probe unspecified – likely phased array or curvilinear array probe.

Remember, it is important to minimize time not doing chest compressions. Record a quick clip, get out of there, and then interpret it later. You are looking for A) If the heart is beating B) Is it beating well (organized vs disorganized) and C) Is there evidence of a cause for this arrest
How to do point of care ultrasound during cardiac arrest by Michael Schick (@ultrasoundstuff and sonostuff.com). Nice, brief, overview.
Point of care Ultrasound in Cardiac Arrest by Felipe Teran (@FTeranmd) Longer but tons of great info.
Short clip of cardiac standstill
Results
Patients
N=225
(Only 170 analyzed for organized vs disorganized)
- ROSC 55.5%
- Hospital admission 32%
- Hospital discharge 1.8%
- 75 patients (33.3%) had organized activity
- 95 patients (42.2%) had disorganized activity
- 55 patients (24.4%) had indeterminant activity. These cases were described as cardiac activity being visualized but “insufficient image resolution” to determine the type of activity
Comparing differences in characteristics of organized versus disorganized activity patients:
- Patients with organized activity had longer resuscitation (38.1 min vs 26.2 min)
- Other factors not significantly different including: age, gender, down time, location or arrest, bystander CPR, # of 1 mg Epinephrine doses
- 56% of this population (PEA with cardiac activity) was treated by ACLS protocols
- 44% were treated with medications outside of ACLS protocols
-Most commonly calcium chloride
-Second most common was intravenous adrenergic agents (Dopamine > Norepinephrine > Epinephrine, Dobutamine, Neosynephrine)
-Other meds given were magnesium(4), thrombolytics (6), and intralipid (1)
Ultimately, it looks like the “non-ACLS group” became labeled as the “intravenous adrenergic agent group”. As the total patients adds up, we are led to assume that in fact, every patient who received non-ACLS medications, received intravenous adrenergic medications.

Primary Outcome Survival to Hospital Admission
In those that received standard ACLS medications only:
Organized cardiac activity: 37.7% (CI 29.9 to 51.2)
Disorganized cardiac activity: 17.9% (CI 10.9-28)
In those that received IV adrenergic medications:
Organized cardiac activity: 45.5% (CI 26.9 to 65.4)
Disorganized cardiac activity: 0% (CI 0 – 21.6)
Secondary Outcomes
ROSC
In those that received standard ACLS medications only:
- Organized Cardiac Activity: 54.7%
- Disorganized Cardiac Activity: 37.2%
In those that received IV adrenergic medications:
- Organized Cardiac Activity: 90.9%
- Disorganized Cardiac Activity: 47.1%
Patients with organized cardiac activity + receiving IV adrenergic medications were 8.2 times more likely to get ROSC, compared to organized activity + ACLS meds.
Survival to Discharge
No statistical difference between any groups
In those that received standard ACLS medications only:
- Organized Cardiac Activity: 1.9% (n=1)
- Disorganized Cardiac Activity: 1.3% (n=1)
In those that received IV adrenergic medications:
- Organized Cardiac Activity: 4.5% (n=1)
- Disorganized Cardiac Activity: 0% (n=0)
Interestingly, in those with disorganized cardiac activities – the non-ACLS group lead to higher ROSC, then lower survival to admission, then the same survival to discharge (but none of these differences were significant)
Summary of Main Results
No difference in any group survival to discharge (secondary outcome)
Organized cardiac activity had better survival than disorganized cardiac activity in both ACLS and non-ACLS groups
Within organized cardiac activity group, Non-ACLS group had better survival than ACLS group
Within disorganized activity group, no significant difference in survival between ACLS group and non-ACLS group
Other Results
Agreement in determining organized or disorganized. Kappa = 0.77
Patients that survived to hospital admission given intravenous adrenergic agents apart from ACLS ultimately received less total epinephrine (3 mg vs 5 mg).
Authors’ Conclusions:
Patients with organized cardiac activity respond better to standard ACLS interventions.
Patients with organized cardiac activity may respond differently to medications such as continuous intravenous vasopressors.
Limitations
Confidence intervals are wide here and many of the comparisons have an overlap in their 95% confidence intervals (CI). Overlapping confidence intervals do not necessarily mean that these differences are not significant BUT it opens up that possibility. Overall, of the twelve possible comparisons – there are only three comparisons without overlapping in confidence intervals and from these we can draw more trustworthy conclusions: 1) There was more ROSC in the organized activity with IV adrenergic than the organized activity with ACLS 2) There was more ROSC and more hospital survival in the organized IV adrenergic compared to disorganized IV adrenergic. Keep in mind ROSC was a secondary endpoint.
These are associations. Can not determine causality. In other words, just because those with organized rhythm survived more, does not mean that having the organized rhythm is what is responsible for their increased survival.
It is not explicitly mentioned why they went from comparing standard ACLS medications and non-ACLS medications to comparing standard ACLS medications to the IV adrenergic subset of non-ACLS medications. Presumably, they thought that this would have the most difference on these patients, but calcium, which was given more often – could have just as easily lead to a survival difference.
Does excluding those without sonographic cardiac activity initially lead to a bias in population? It might certainly lead to better survival based on the results of this groups previous publication. Granted, in this paper they are looking specifically at PEA with cardiac activity because they thought this group might show the best chance of difference in the interventions. It would have been nice to compare patients with no cardiac activity to disorganized to organized. If the point is that organized rhythms may benefit more from interventions, how do we know that disorganized rhythms don’t benefit more than those without cardiac activity?
Losing 24.4% of the population because of uninterpretable ultrasounds could have significantly affected the results.
The same criticisms relevant to the first REASON trial apply here. Most importantly, the lack of neurological outcomes in survivors. We can talk all day about how an intervention might improve ROSC, but that is not that important of an endpoint. Increasing survival to hospitalization is a good start. Even if they don’t survive to discharge, perhaps that extra time is valuable to family or to the patient in some way. Similarly, if this showed improved survival to discharge – that certainly can be important to people. Some people and their families would prefer coma to death. Obviously, what would be ideal is showing that people are not only surviving more, but surviving with good neurologic status. We have a long way to go to get there.
Since this is an analysis of previously collected data, there is no way to tell why the treating physicians started IV adrenergic medications. It would be nice for these authors if the reason they did this was because of what they saw on ultrasound. If not – perhaps there are other variables not accounted for that both instigated their decision and could account for some survival benefit.
Discussion
Is this sub-categorization practical in real-life? Can physicians not only differentiate yes or no cardiac activity but also organized and disorganized? Two recent articles show potential problems. First – ultrasound already poses a risk of delaying chest compressions and adding another component to the interpretation may make that worse (not that it necessary needs to if people are doing it correctly, but it could be a consequence because that doesn’t always happen). Secondly, there is already sub-par agreement among physicians as far as what constitutes cardiac standstill – I imagine that this added distinction of organization of activity may have similar challenges. Nonetheless, just because something is hard doesn’t mean it shouldn’t be implemented if it helps people. We just need more evidence that it does help people and also that it won’t cause harm.
Take Home Points
1. Differentiating organized and disorganized cardiac activity with point of care ultrasound is feasible.
2. This distinction may influence survival and response to non-ACLS medications.
Our score
Cite this post as
Michael Prats, MD. PEA Arrest. Ultrasound G.E.L. Podcast Blog. Published on November 20, 2017. Accessed on September 10, 2021. Available at https://www.ultrasoundgel.org/32.




