
Authors: Sidwell Kyeyune, MBBS (EM Resident Physician, Makerere University, Kampala, Uganda); Ashley Qualls, MD (EM Resident Physician, University of Missouri-Columbia); Catherine Parker, MD (PD, Associate Professor of EM/Attending Physician, University of Missouri-Columbia); Jessica Pelletier, DO, MHPE (APD/Assistant Professor of EM/Attending Physician, University of Missouri-Columbia) // Reviewed by: Sophia Görgens, MD (EM Physician, Yale University, CT), Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 12-year-old girl is brought by her mother to the ED with a 2-day history of headache and fever. She reports symptoms began after returning home from a summer camp. The patient started vomiting with fevers this morning, and her mother was unable to wake her from her afternoon nap.
On exam, the patient is lethargic and responds to painful stimuli with temperature of 38.2 C, blood pressure 88/65 mmHg, and HR 132 bpm. She has a petechial rash on her lower back and lower extremities, as well as resistance to neck flexion.
Lumbar puncture is performed; CSF analysis shows:
- WBC – 2500/mL
- Proteins – 300mg/dL
- Glucose – 20mg/dL
- Neutrophils – 85%
What is the diagnosis?
Answer: Meningococcal disease
Background:
- Neisseria (N.) meningitidis is a bacterium that causes meningococcal disease that often causes community-acquired sepsis, meningitis, and death.1
- Meningococcal disease is symptomatic; asymptomatic carriers are not included.
- Common symptoms: flu-like symptoms, septicemia, and meningitis.
- Less common symptoms: arthritis, conjunctivitis, myocarditis, pericarditis, pneumonia, or urethritis.2
- Meningococcal disease presents as meningitis in approximately 50% of cases in the United States and higher than 50% in developing countries.3
- Most exposed individuals are asymptomatic carriers, with N. meningitidis colonizing the nasopharynx.1
- Known to infect a large number of individuals within a short time due to asymptomatic carriers.
- Often spread quickly among those living in close proximity to each other.1.
- Overcrowded populations, college dormitories, and military bases
- Case fatality rate of 10-15%4 for meningococcal disease and 3-10% for meningococcal meningitis.5
- 1 in 5 have severe, life-long complications like deafness, neurologic deficits, and cognitive deficits.4
Etiology:
- N. meningitidis is one of the most common causes of bacterial meningitis in the U.S.2
- High mortality and morbidity rate.
- Morbidity includes deafness, neurologic deficits, and cognitive deficits.
Epidemiology:
- N. meningitidis is a ubiquitous bacterium found worldwide.
- The greatest incidence of meningococcal disease occurs in the Meningitis Belt in Africa, running from Gambia-Senegal in the West to Ethiopia-Eritrea and Northern Kenya in the East.6
- During epidemics and in the dry seasons, incidence can rise to as high as 1 case per 100 people.6
- With the introduction of various vaccination programs in the Meningitis Belt, the occurrence of such epidemics has significantly decreased.3
- Rates of meningococcal disease are much lower in Europe and the U.S., with less than 5 cases per 100,000 population per year due to well-developed vaccination schedules.7
- Meningococcal disease shows a bimodal distribution, with incidence rates highest among infants, and a second peak is seen among youth and adolescents.3,8

Clinical Presentation:
- The presentation of patients with meningococcal disease varies according to the severity of disease, immune status, and age of the patient, ranging from fever and flu-like symptoms to sepsis, meningitis, and fulminant disease.
- Patients usually present within 1-10 days after exposure; often within 4 days.1
- There are several distinct clinical syndromes:1
- Meningococcal meningitis (60%)10
- Headache, malaise, myalgias, fever.
- However, this can be differentiated from meningococcemia by the presence of:
- Meningeal signs like neck stiffness, and photophobia.
- Altered mental status, seizures, and irritability in infants and young children.
- Meningococcemia (5-20%)11 – presents with a flu-like illness, including:
- Fever
- Headache
- Myalgias
- Pharyngitis
- Rhinorrhea
- Vomiting
- In 40-70% of patients, these initial symptoms will progress to shock and the pathognomonic petechial rash.12
- In more severe cases:
- Acute adrenal hemorrhage (i.e., Waterhouse-Frederickson syndrome)
- Multiorgan failure
- Pallor with cold extremities
- Less common manifestations include:11
- Pneumonia
- Septic arthritis
- Osteomyelitis
- Epiglottitis
- Urethritis
- Pericarditis
- Conjunctivitis
- Meningococcal meningitis (60%)10

Evaluation:
- Initial presentations are often non-specific, making a thorough history and physical examination essential.
- Key history findings: close proximity living to others, vaccination status, travel history, especially to areas in the Meningitis Belt, quick symptom onset, immunocompromise.
- Key exam findings: Altered mental status/confusion, fever, headache, neck stiffness, petechial rash.4
- Physical exam maneuvers to detect meningeal irritation
- Kernig’s sign:13
- Patient supine and hip flexion to 90 degrees
- Positive if extension of the knee elicits low back pain
- Sensitivity: 5%
- Specificity: 95% for bacterial meningitis in adults
- Brudzinski’s sign:13
- With patient supine, passively flex the neck
- Positive if flexion of the neck causes spontaneous flexion of the hips
- Sensitivity: 5%
- Specificity: 95% for bacterial meningitis in adults
- Jolt accentuation test:14
- Patient rotates head horizontally 2-3 times per second
- Positive if the existing headache worsens
- Sensitivity: 65.3%
- Specificity: 4%
- Kernig’s sign:13
- Physical exam maneuvers to detect meningeal irritation
- Classic triad of symptoms: fever, neck stiffness, and altered mental status15
- All three present in about 41% of patients.15
Diagnosis:
- Earlier diagnosis and antibiotic treatment lead to better outcomes; thus, immediate recognition of meningococcal disease is critical.
- Microbiological examination is key in the diagnosis of meningococcal disease.4
- The gold standard for diagnosis is the lumbar puncture (LP).
- Results of CSF analysis will show elevated white blood cells (WBCs), low glucose, high protein, and increased opening pressure.16
- Consider obtaining a computed tomography BEFORE LP in the setting of:17
- Known or suspected increased intracranial pressure (ICP), such as known intracranial mass lesion, papilledema, visual change, nausea, vomiting, headache, dizziness, or change in behavior.
- Focal neurologic deficits.
- Recent epileptic seizures.
- Severely impaired consciousness.
- Immunocompromise – there is disagreement across guidelines about this, so clinical judgment should be utilized.18
- CT imaging is used to assess for cerebral edema or other signs suggestive of increased intracranial pressure (ICP); performing LP in the setting of this clinical finding could lead to herniation or death.12
- When LP is contraindicated, other modes of detection may be used such as PCR or culture of nasopharyngeal swabs or blood cultures.12
- Blood cultures can be effective in detecting meningococcemia, while testing of other affected areas can guide detection and treatment.5,11
- If suspecting arthritis, an arthrocentesis should be performed.
- Antibiotics given before LP decrease the detection of bacteria by CSF culture, PCR, and Latex agglutination test by up to 44%.13
- Latex agglutination testing is often used in settings where PCR and culture may be unavailable. CSF is typically used for this test with serum and urine often being other sources for culture. 19


Treatment:
- Pre-hospital:
- Emergent referral to hospital for any patient in an endemic area or in the community presenting with:13
- Headache
- Altered mental state
- Neck stiffness
- Fever
- Rash
- Signs of shock
- The presence of these signs and symptoms on their own is a poor indicator of disease.13
- However, if occurring in combination, in an endemic area or during an outbreak, should raise an index of suspicion for meningococcal disease or meningitis.13
- Pre-hospital antibiotics rarely provide benefit, however should be considered if:21
- Patient presenting to a rural or remote healthcare practice and
- Long transit time to nearest referral centre or secondary hospital.
- Emergent referral to hospital for any patient in an endemic area or in the community presenting with:13
- Health safety measures:
- Ensure droplet precautions to ensure health worker safety and reduce the risk of transmission of a nosocomial infection to other patients.22
- This entails:23
- Surgical face mask within 6 feet of the patient.
- Patient should wear mask, where applicable
- Wear a face shield or eye googles
- Place patient in single room, if possible
- Hand washing/alcohol rub before entering or leaving the patient’s room
- This entails:23
- Ensure droplet precautions to ensure health worker safety and reduce the risk of transmission of a nosocomial infection to other patients.22
- Initial assessment:
- Airway stabilization.
- Breathing, providing support where needed.
- Circulation – patients with meningococcal disease may present in shock24
- Insert 2 large-bore IV cannulae and give an initial bolus of 20 ml/kg bolus of crystalloids over 5-10 minutes to a maximum of 40-60 ml/kg.25
- Fluid therapy should be guided by continuous monitoring with heart rate, blood pressure, urine output, and peripheral perfusion.25
- Start vasopressors for patients who are not fluid responsive (norepinephrine is first-line, as in most cases of septic shock).26
- Establish central venous access if large-bore peripheral access cannot be obtained or if there is an anticipated prolonged need for vasopressors.25
- Empiric antibiotic treatment:22
- Once blood and CSF samples for culture have been taken off, start empiric antibiotics.
- Give IV ceftriaxone empirically PLUS IV dexamethasone.
- Vancomycin should be added in regions with high rates of S. pneumoniae resistance to ceftriaxone.5
- Antibiotics should be started before lumbar puncture is performed if;22
- The patient is in septic shock.
- Clinical exam reveals a need to get a CT scan of the head before LP
- Clinical contraindications to LP:29
- Relative
- Antiplatelet therapy
- Platelet count 20–40 × 109/L
- Absolute
- Anticoagulant therapy
- Local skin infections
- Non-communicating obstructive hydrocephalus
- Platelet count <20 × 10⁹/L
- Spinal or cranial developmental abnormalities
- Spinal stenosis or spinal cord compression above level of puncture
- Uncorrected bleeding diathesis
- Multiple failed attempts at lumbar puncture
- Relative
- In these patients, draw blood culture samples and begin intravenous empiric antibiotics then perform lumbar puncture at earliest possible opportunity.22
- Add IV ampicillin/amoxicillin in patients at risk of Listeria infection which includes:27
- Neonates
- Age > 50 years
- Immunosuppressed patients
- Pregnancy
- Other options for Listeria coverage include meropenem, linezolid, levofloxacin, or trimethoprim-sulfamethoxazole.

- Definitive treatment: After diagnostic confirmation of N. meningitidis, antibiotic treatment can be narrowed down to;
- Adjunctive management:9,33
- First dose should be given 15-20 minutes before or concurrently with the first dose of antibiotics.
- Dexamethasone 0.15mg/kg in children and 10mg in adults 6-hourly.
- Can decrease the incidence of hearing loss and neurologic sequelae.
- Contraindications:9
- Age <6 weeks or ≥60 years.
- Immunocompromised
- CSF shunt-related or other nosocomial meningitis.
- In patients with signs of elevated ICP, elevate the head of the bed to 30 degrees.9
- Typical agents used to treat elevated ICP, including hypertonic saline and mannitol, have shown no benefit and even possible increased mortality in bacterial meningitis patients.
- Close contact post-exposure prophylaxis (PEP):34,35
- Includes:
- Those living under the same roof.
- Daycare contacts.
- Those exposed to the oral secretions of an infected patients via kissing, mouth-to-mouth resuscitation, or aerosol-generating procedures (without appropriate PPE).
- Provide regardless of immunization status if indications present.
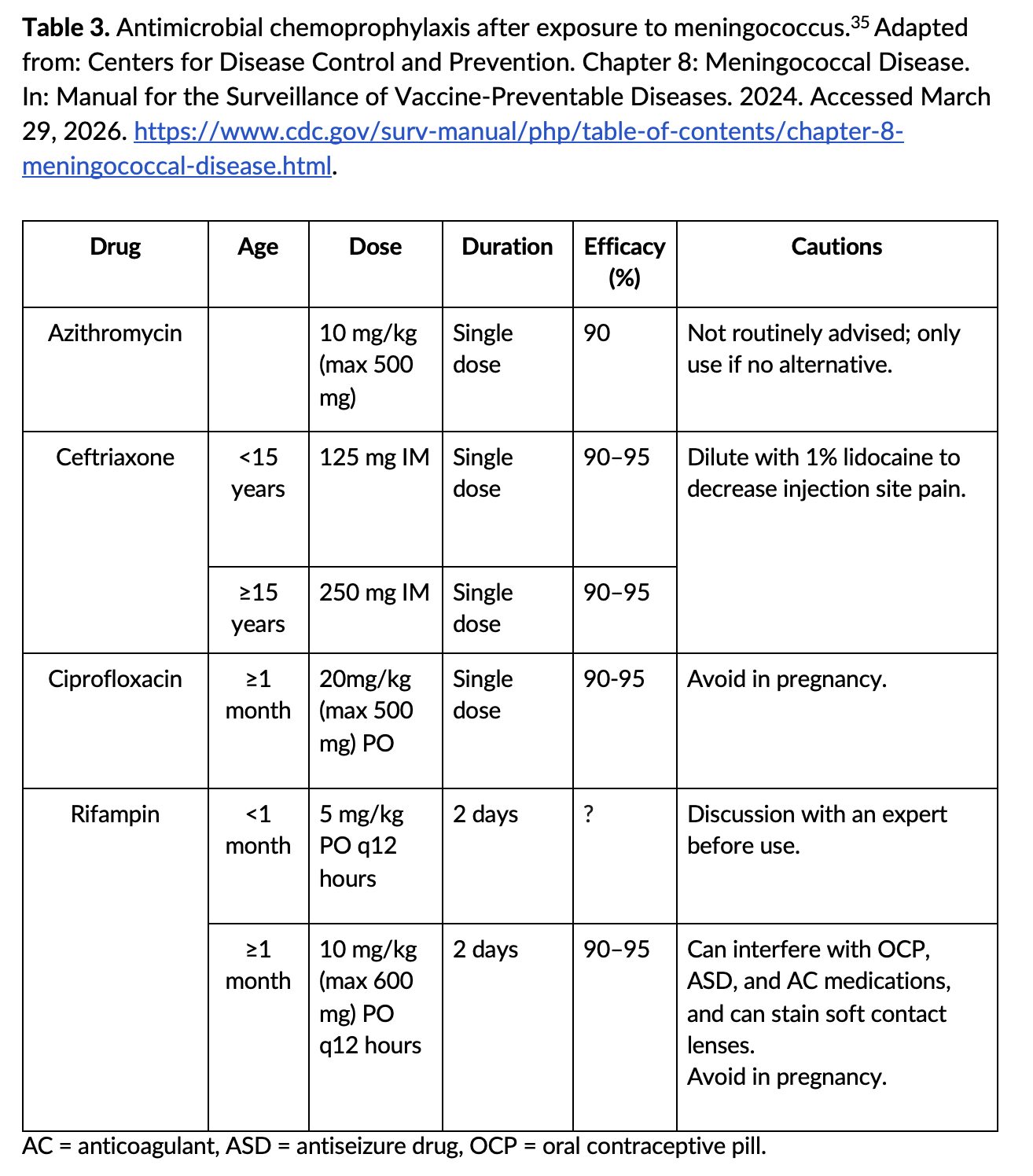
- Rifampicin, ceftriaxone, and ciprofloxacin are the recommended options (Table 3).
- Includes:
- Healthcare worker exposure recommendations:36
- PEP should be given regardless of vaccination status.
- The exposed person should not return to work until 24 hours after starting PEP.
Prevention:
- Healthcare workers should use droplet precautions when working with patients suspected to have meningococcal disease.36
- Vaccines are available to protect against 5 of 6 predominant serogroups.7
- Three of these vaccines are quadrivalent meningococcal conjugate vaccines that confer protection against serogroups A, C, W, and Y.
- The remaining two vaccines protect against serogroup B meningococcus.
- Serogroup X does not have vaccine coverage.
Prognosis:
- Current case-mortality rate is around 5% but can still be as high as 10-15% even with prompt antibiotic treatment.12
- Higher mortality, up to 50%, is seen in delayed treatment and untreated disease.12
- Favourable outcomes are seen in:
- Predictors of poor prognosis:
- Age – the elderly and the very young.
- Low Glasgow Coma Scale score.
- Hypotension.
- Low CSF white cell count.
- Leukopenia and thrombocytopenia.
- Altered mental status.10
- Reduced susceptibility to penicillins.39
- Even with treatment and resolution of symptoms, meningococcemia is associated with long-term effects in up to 20% of survivors, predominantly with physical/neurologic manifestations such as:1
Pearls:
- Meningococcal disease is a high morbidity and mortality illness.
- Early recognition and stabilization are critical.
- Have this on the differential for patients with flu-like illness and/or meningitis symptoms associated with lack of vaccination, immunocompromise, living in close quarters, or living/travel to the Meningitis Belt.
- Diagnosis involves blood cultures PLUS LP.
- Perform CT before LP if there are signs and symptoms of increased ICP.
- Treat empirically before LP in patients with signs of increased ICP, meningococcal sepsis, or shock.
- Empiric therapy involves ceftriaxone +/- vancomycin (depending on local S. pneumoniae resistance patterns) +/- ampicillin + dexamethasone.
- All patients in whom this diagnosis is suspected should be admitted.

A 21-year-old patient presents to the emergency department with altered mental status. He has had flu-like symptoms for 2 days. Today, his roommates found him in bed, confused. His HR is 140 bpm, BP is 96/60 mm Hg, RR is 30/min, and SpO2 is 91%. Physical examination shows an ill-appearing patient with a diffuse petechial rash, labored breathing, roving eye movements, and slow bleeding from three peripheral IV sites. Which laboratory value is most likely to be found with this patient’s diagnosis?
A) Anemia
B) Elevated D-dimer
C) Elevated fibrinogen
D) Leukocytosis
E) Thrombocytosis
Answer: B
This patient likely has a meningococcal infection, leading to meningitis based on vital signs suggestive of sepsis, altered mental status, and a petechial rash. Meningococcal illness is typically rapidly progressive, culminating in the early onset of shock. Disseminated intravascular coagulation (DIC) is also extremely common in patients with meningococcal infections. No single laboratory value is diagnostic of DIC.
Thrombocytopenia, prolonged partial thromboplastin time (PT) and activated partial thromboplastin time (aPTT), low fibrinogen, elevated D-dimer, and signs of inappropriate bleeding are all typically present with DIC. Signs of end-organ dysfunction and shock are frequently absent and are not reliable indicators of illness severity. Treatment is focused on resolving the underlying cause while providing supportive care. Platelet transfusion, plasma administration to replace clotting factors, and anticoagulation are only beneficial in patients with severe bleeding, thrombocytopenia, or focal ischemia, respectively.

Anemia (A) is frequently observed in DIC due to diffuse microangiopathy. However, anemia is often absent until later in the course of the disease or is masked by dehydration upon presentation.
Elevated fibrinogen (C) would not be seen with DIC. Fibrinogen levels are low due to the consumption of clotting factors by diffuse clot formation.
Leukocytosis (D) is not a reliable indicator of DIC or severe infection. Severe infection may lead to leukopenia in some patients.
Thrombocytosis (E) would also be atypical in the setting of DIC. Platelet consumption by diffuse clot formation typically results in thrombocytopenia.
Further Reading:
Further FOAMed:
- https://emcrit.org/ibcc/id/
- https://www.emdocs.net/meningitis-why-do-we-miss-it-how-do-we-improve/
- https://www.emdocs.net/emdocs-podcast-episode-115-adult-meningitis/
- https://www.emdocs.net/the-em-educator-series-meningitis-unusual-headache-and-fever/
- https://www.emdocs.net/em3am-bacterial-meningitis/
- https://www.emdocs.net/medical-malpractice-insights-missed-meningococcemia-in-the-midst-of-a-meningitis-outbreak/
- https://www.emdocs.net/bacterial-meningitis-in-children/
- https://www.emdocs.net/the-sick-meningitis-patient-from-bad-to-worse/
- https://www.emdocs.net/pediatric-meningitis-pearls-and-pitfalls/
- https://www.emdocs.net/meningitis-clinical-pearls-pitfalls/
References:
- Vaz LE. Meningococcal Disease. Pediatr Rev. 2017;38(4):158-169. doi:10.1542/pir.2016-0131
- Schaffer DeRoo S, Torres RG, Fu LY. Meningococcal disease and vaccination in college students. Hum Vaccines Immunother. 2021;17(11):4675-4688. doi:10.1080/21645515.2021.1973881
- Stephens DS. Global Control of Meningococcal Disease. N Engl J Med. 2023;388(21):2003-2005. doi:10.1056/NEJMe2301698
- Centers for Disease Control and Prevention. Meningococcal Disease. In: Yellow Book. 2025. https://www.cdc.gov/yellow-book/hcp/travel-associated-infections-diseases/meningococcal-disease.html
- van de Beek D, Brouwer MC, Koedel U, Wall EC. Community-acquired bacterial meningitis. Lancet. 2021;398(10306):1171-1183. doi:10.1016/S0140-6736(21)00883-7
- Jafri RZ, Ali A, Messonnier NE, et al. Global epidemiology of invasive meningococcal disease. Popul Health Metr. 2013;11(1):17. doi:10.1186/1478-7954-11-17
- Burman C, Serra L, Nuttens C, Presa J, Balmer P, York L. Meningococcal disease in adolescents and young adults: a review of the rationale for prevention through vaccination. Hum Vaccines Immunother. 2019;15(2):459-469. doi:10.1080/21645515.2018.1528831
- Harrison LH, Pelton SI, Wilder-Smith A, et al. The Global Meningococcal Initiative: Recommendations for reducing the global burden of meningococcal disease. Vaccine. 2011;29(18):3363-3371. doi:10.1016/j.vaccine.2011.02.058
- Cejin MC, Koyfman A, Long B. High risk and low incidence diseases: Meningococcal disease. Am J Emerg Med. 2026;99:114-122. doi:10.1016/j.ajem.2025.09.031
- Van De Beek D, De Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M. Clinical Features and Prognostic Factors in Adults with Bacterial Meningitis. N Engl J Med. 2004;351(18):1849-1859. doi:10.1056/NEJMoa040845
- Rosenstein NE, Perkins BA, Stephens DS, Popovic T, Hughes JM. Meningococcal Disease. N Engl J Med. 2001;344(18):1378-1388. doi:10.1056/NEJM200105033441807
- Nadel S. Treatment of Meningococcal Disease. J Adolesc Health Off Publ Soc Adolesc Med. 2016;59(2 Suppl):S21-28. doi:10.1016/j.jadohealth.2016.04.013
- McGill F, Heyderman RS, Panagiotou S, Tunkel AR, Solomon T. Acute bacterial meningitis in adults. The Lancet. 2016;388(10063):3036-3047. doi:10.1016/S0140-6736(16)30654-7
- Iguchi M, Noguchi Y, Yamamoto S, Tanaka Y, Tsujimoto H. Diagnostic test accuracy of jolt accentuation for headache in acute meningitis in the emergency setting. Cochrane Acute Respiratory Infections Group, ed. Cochrane Database Syst Rev. Published online October 13, 2017. doi:10.1002/14651858.CD012824
- Hasbun R. Progress and Challenges in Bacterial Meningitis: A Review. JAMA. 2022;328(21):2147. doi:10.1001/jama.2022.20521
- Shahan B, Choi EY, Nieves G. Cerebrospinal Fluid Analysis. Am Fam Physician. 2021;103(7):422-428.
- Dyckhoff-Shen S, Koedel U, Pfister HW, Klein M. SOP: emergency workup in patients with suspected acute bacterial meningitis. Neurol Res Pract. 2021;3(1):2. doi:10.1186/s42466-020-00098-6
- Glimåker M, Sjölin J, Åkesson S, Naucler P. Lumbar Puncture Performed Promptly or After Neuroimaging in Acute Bacterial Meningitis in Adults: A Prospective National Cohort Study Evaluating Different Guidelines. Clin Infect Dis. 2018;66(3):321-328. doi:10.1093/cid/cix806
- Miller JM, Binnicker MJ, Campbell S, et al. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). Clin Infect Dis. Published online March 5, 2024:ciae104. doi:10.1093/cid/ciae104
- Singh N. Inside the Brain: Cerebrospinal Fluid Insights in Meningitis. Cureus. Published online August 16, 2024. doi:10.7759/cureus.67008
- Alam M, Bastakoti B. Therapeutic Guidelines: Antibiotic. Version 15. Aust Prescr. 2015;38(4):137-137. doi:10.18773/austprescr.2015.049
- Young N, Thomas M. Meningitis in adults: diagnosis and management. Intern Med J. 2018;48(11):1294-1307. doi:10.1111/imj.14102
- Centers for Disease Control and Prevention. Standard Precautions for All Patient Care. 2024. Accessed March 29, 2026. https://www.cdc.gov/infection-control/hcp/basics/standard-precautions.html
- Thim T, Krarup NHV, Grove EL, Rohde CV, Løfgren B. Initial assessment and treatment with the Airway, Breathing, Circulation, Disability, Exposure (ABCDE) approach. Int J Gen Med. 2012;5:117-121. doi:10.2147/IJGM.S28478
- Sarfatti A, Nadel S. Management of meningococcal disease. Paediatr Child Health. 2019;29(5):197-204. doi:10.1016/j.paed.2019.02.001
- Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021;49(11):e1063-e1143. doi:10.1097/CCM.0000000000005337
- McGill F, Heyderman RS, Michael BD, et al. The UK joint specialist societies guideline on the diagnosis and management of acute meningitis and meningococcal sepsis in immunocompetent adults. J Infect. 2016;72(4):405-438. doi:10.1016/j.jinf.2016.01.007
- World Health Organization (WHO). WHO Guidelines on Meningitis Diagnosis, Treatment and Care. 2025. Accessed May 6, 2026. https://www.ncbi.nlm.nih.gov/books/NBK614847/pdf/Bookshelf_NBK614847.pdf
- Costerus JM, Brouwer MC, Van De Beek D. Technological advances and changing indications for lumbar puncture in neurological disorders. Lancet Neurol. 2018;17(3):268-278. doi:10.1016/S1474-4422(18)30033-4
- Sucher A, Heinrich A, Ramsey S. Treatment and Prevention of Community-Acquired Bacterial Meningitis. US Pharm. Published online January 19, 2021. Accessed March 27, 2026. https://www.uspharmacist.com/article/treatment-and-prevention-of-communityacquired-bacterial-meningitis
- Tunkel AR, Hasbun R, Bhimraj A, et al. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis*. Clin Infect Dis. 2017;64(6):e34-e65. doi:10.1093/cid/ciw861
- Van De Beek D, Cabellos C, Dzupova O, et al. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clin Microbiol Infect. 2016;22:S37-S62. doi:10.1016/j.cmi.2016.01.007
- Brouwer MC, McIntyre P, De Gans J, Prasad K, Van De Beek D. Corticosteroids for acute bacterial meningitis. In: The Cochrane Collaboration, ed. Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd; 2010:CD004405.pub3. doi:10.1002/14651858.CD004405.pub3
- Brady RC. Meningococcal Infections in Children and Adolescents. Adv Pediatr. 2020;67:29-46. doi:10.1016/j.yapd.2020.03.007
- Centers for Disease Control and Prevention. Chapter 8: Meningococcal Disease. In: Manual for the Surveillance of Vaccine-Preventable Diseases. 2024. Accessed March 29, 2026. https://www.cdc.gov/surv-manual/php/table-of-contents/chapter-8-meningococcal-disease.html
- Centers for Disease Control and Prevention. Meningococcal Disease. 2024. Accessed May 6, 2026. https://www.cdc.gov/infection-control/hcp/healthcare-personnel-epidemiology-control/meningococcal-disease.html
- Soeters HM, Diallo AO, Bicaba BW, et al. Bacterial Meningitis Epidemiology in Five Countries in the Meningitis Belt of Sub-Saharan Africa, 2015–2017. J Infect Dis. 2019;220(Supplement_4):S165-S174. doi:10.1093/infdis/jiz358
- Diallo F, Haidara FC, Tapia MD, et al. Safety and immunogenicity of a pentavalent meningococcal conjugate vaccine targeting serogroups A, C, W, Y, and X when co-administered with routine childhood vaccines at ages 9 months and 15 months in Mali: a single-centre, double-blind, randomised, controlled, phase 3, non-inferiority trial. The Lancet. 2025;405(10484):1069-1080. doi:10.1016/S0140-6736(25)00046-7
- Cubells CL, García JG, Martinez JR, Otin CL. Clinical data in children with meningococcal meningitis in a Spanish hospital. Acta Paediatr. 1997;86(1):26-29. doi:10.1111/j.1651-2227.1997.tb08826.x




