
Author: Thomas Pederson, MD (Associate Physician Diplomate of Emergency Medicine and Anesthesiology Critical Care Medicine, UC San Diego Health) // Reviewed by: Jessica Pelletier, DO, MHPE (APD/Assistant Professor of EM/Attending Physician, University of Missouri-Columbia); Alex Koyfman (@EMHighAK); Brit Long, MD (@long_brit)
Case
A 68-year-old man with end-stage heart failure (HF) status post remote HeartMate 3 (HM3) left ventricular assist device (LVAD) implantation presents to the Emergency Department (ED) with several days of exertional shortness of breath. On arrival, he appears edematous, his LVAD is alarming for low flow, his MAP is 115 mmHg, and his chest X-ray shows bilateral symmetric alveolar infiltrates. After initial evaluation and workup, you consult with Cardiology who recommends admission for diuresis and blood pressure control with a nicardipine infusion. Following these interventions, his LVAD flows improve, his work of breathing normalizes, and he no longer requires supplemental oxygen.
This case raises several important questions:
- Why is this clinical presentation common in patients with modern LVADs?
- What LVAD devices are currently used in the U.S.?
- What are common ED presentations for patients with 3rd-generation LVADs?
- Which LVAD device parameters should be assessed to identify complications?
Background
In 2025, what device(s) are we using?
Figure 1. Evolution of LVAD device implant in the U.S. from LVAD conception to present. Adapted from: https://doi.org/10.1016/j.pcad.2024.01.018.1
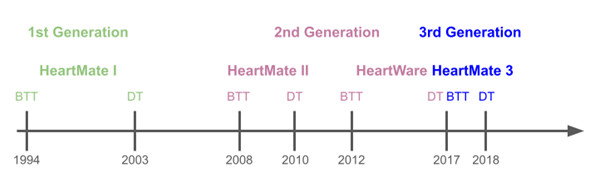
The Abbott HeartMate 3 (HM3), introduced in 2018, is currently the only FDA-approved durable LVAD in the United States. It is a 3rd-generation, continuous-flow, magnetically levitated centrifugal pump. Universal adoption of the HM3 followed the MOMENTUM 3 trial, which demonstrated improved 6-month survival free of disabling stroke or reoperation for device removal compared with axial-flow pumps.2 These outcomes are attributed to design changes that reduce shear stress and minimize stagnant blood flow.
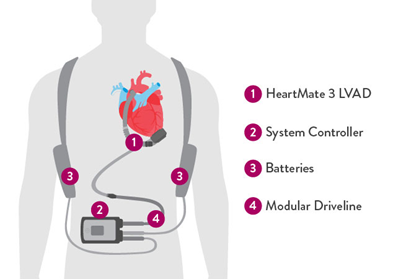
Figure 2. HeartMate 3 LVAD system overview.3 Reproduced with permission from https://www.cardiovascular.abbott/us/en/hcp/products/heart-failure/left-ventricular-assist-devices/heartmate-3/about/system-overview.html.
Who is getting LVADs these days?
Trends you will notice in the ED:
- Destination therapy (DT) now represent 50–80% of implants.4,5
- Most recipients are male (76.5%), reflecting underlying HF epidemiology.6
- Patients aged 60–69 years remain the largest group (30.9%), though implantation in younger patients is increasing common due to excellent survival (92.5% at 1 year; 76.3% at 5 years).6
If you work in any ED that sees advanced cardiac disease, you will increasingly encounter LVAD patients.
What does the latest data suggest about LVAD survival?
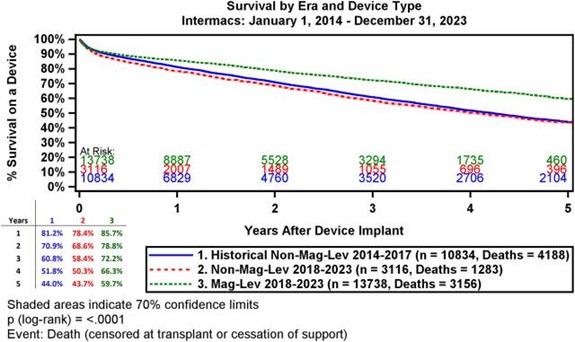
Magnetically levitated pumps have led to significantly improved long-term survival.
- HM3 1-year survival: 85.7%.
- HM3 5-year survival: 59.7% versus 78.4% and 43.7% for non–magnetically levitated devices.6
Survival rates for the HM3 are approaching that of heart transplantation, and survival is even more pronounced in the younger patient population.6
Figure 3. Comparison of Kaplan-Meier curves for 2nd and 3rd generation LVADs. Green dotted = 3rd generation LVAD curve. Reproduced with permission from https://doi.org/10.1016/j.athoracsur.2024.10.003.6
Common ED Presentations in LVAD Patients
A retrospective analysis of patients receiving HM3 at one center in Germany from 2014 to 2024 demonstrated that 77% of them presented to the ED postoperatively; however, only 8% of visits were related to the LVAD.7 You can expect to diagnose a majority of non-LVAD-related problems in these patients.
Most common chief complaints:8
- Bleeding: 29%
- Chest pain:14%
- Syncope or dizziness: 13%
Most common LVAD-related diagnoses:8–10
- Bleeding: 14 – 29%
- Infection: 15 – 21%
- HF: 11 – 14.5%
About two-thirds of LVAD ED visits result in admission.
HM3 patients have much lower 1-year readmission rates than older devices.6
Initial Approach to the LVAD Patient in the ED
1. Notify the VAD Coordinator Early
- LVAD patients are often well educated about their device and have a VAD-trained caregiver, but they may still present unexpectedly to the ED. Early involvement of the hospital’s LVAD coordinator is essential; if the ED is not linked to an LVAD center, transfer processes should begin early while simultaneously assessing clinical stability. Task your unit clerk, house supervisor, and/or charge nurse with the referral process so that you can focus on the resuscitation.
2. Assess Clinical Stability
- In stable patients, proceed with a standard ED workflow.
- For the unstable patient:
- Assess perfusion: Most LVAD patients have minimal or no palpable pulse, and MAP is the primary blood pressure measure to follow. Capillary refill remains a reliable exam indicator of perfusion.
- With sphygmomanometer assessment, Doppler ultrasound of the opening pressure approximates the MAP.
- An arterial line should ideally be inserted in all LVAD patients considered for admission.
- A MAP of < 60 mmHg is concerning for impaired perfusion.
- Assess perfusion: Most LVAD patients have minimal or no palpable pulse, and MAP is the primary blood pressure measure to follow. Capillary refill remains a reliable exam indicator of perfusion.
-
- In cardiac arrest: perform ACLS (chest compressions are allowed, more on this later).
- Cardiac arrest can be difficult to appreciate in patients with LVAD. In the unresponsive patient, abnormal skin color, prolonged capillary refill, MAP < 50 mmHg, and end-tidal CO2 < 20 mmHg are all highly concerning for cardiac arrest.
- Get an EKG: to identify any life-threatening arrhythmias.
- Rapid LVAD Assessment: follow the driveline externally and inspect connections for damage.
- In cardiac arrest: perform ACLS (chest compressions are allowed, more on this later).
For the HM3 device, the 4 main LVAD controller parameters are all visible on the main screen, and each can be viewed by pressing the “display” button to toggle through the main screens (Figure 4, item D):
- Pump speed (RPM): set by LVAD specialists, rarely adjusted in the ED.
- Pump flow (L/min): influenced by the pump speed, and affected by changes in LV preload and afterload.11
- Preload ↑ = flow ↑
- Afterload ↑ = flow ↓
- Pump power (watts): the amount of energy required to maintain the pump speed.
- Increased power → think pump obstruction, pump thrombosis, or changes in physiologic demand.10
- Pulsatility index (PI): reflects the degree of interaction between the LVAD and the native contractility of the heart.
- High PI = more native LV function.
- Low PI = LVAD is generating the majority of cardiac output.
- Large PI changes → volume shifts, arrhythmia, or suction events (when the inflow cannula becomes occluded by the LV lateral or septal walls).11
Table 1. Typical settings of the three LVADs likely to be encountered. HeartMate 3 is the only currently FDA-approved device for implantation. Adapted from https://doi.org/10.1016/j.ccc.2023.06.004.5
| Characteristic | HeartMate II (HMII) | HeartWare (HVAD) | HeartMate 3 (HM3) |
| Pump Type | Axial Flow Pump | Centrifugal Flow Pump | Centrifugal Flow Pump |
| Speed (RPM) | 8,000–10,000 | 2,400–3,200 | 4,800–6,500 |
| Flow (LPM) | 4–7 | 4–6 | 4–6 |
| Power (watts) | 5–8 | 3–7 | 4.5–6.5 |
| Pulsatility Index | 5–8 | 2–4 | 3.5–5.5 |
Figure 4. HeartMate 3 system controller schematic. Open access image reproduced from: https://doi.org/10.1016/j.jemermed.2025.10.041.11
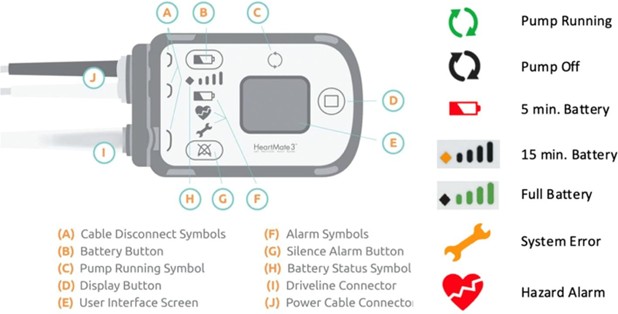
Table 2. LVAD alarm interrogation pathway. Table adapted from https://doi.org/10.1016/j.ccc.2023.06.004 (Table 1) and https://doi.org/10.1016/j.jemermed.2025.10.041 (Figure 2).5,11
| Complication | LVAD Hum | LVAD Alarm | Initial Investigation | Management/Treatment |
| Pump Failure | Absent | Low flow, no alarm in complete device failure | Evaluate all power sources (batteries, connections). | Attempt to restart device, re-establish power. Prepare for potential device replacement. Treat cardiogenic shock. |
| Power Disruption | Absent | Connect power and backup battery | Thoroughly check all driveline and power connections for integrity/disconnection. | Reconnect power source. Attempt to restart. Possible device replacement if hardware is damaged. Treat cardiogenic shock. |
| Driveline Problem/Damage | Absent | Connect driveline | Visually inspect driveline for bends, kinks, or signs of damage. | Secure connections. Treat cardiogenic shock. |
| High Flow State | Present | No alarm | Assess for systemic vasodilatory/distributive shock (e.g., sepsis, anaphylaxis). | Vasopressors, appropriate fluid resuscitation, targeted antibiotics if septic. |
| Low Flow State | Present | Low flow | Evaluate for: hypovolemia, dysrhythmia, tamponade, systemic hypertension (HTN), outflow stenosis, or suction events. | Management is highly dependent on the underlying cause (e.g., fluid bolus for hypovolemia, rhythm control, pericardiocentesis). |
| High Power Consumption | Present | Low flow, possibly no alarm | High suspicion for pump thrombosis. | Optimize anticoagulation. Consider thrombolytics in select cases. Urgent pump replacement for refractory cases. |
| High Pulsatility Index (PI) | Present | No alarm | Assess for suction event*, or early signs of systemic illness (e.g., sepsis). May also represent genuine LV recovery. | Administer fluid bolus for suspected suction. Serial assessment of LV morphology and function. |
| Low Pulsatility Index (PI) | Present | No alarm | Evaluate for low volume status/hypovolemia. | Treat with fluid bolus. |
Suction event = occlusion of the inflow cannula by the LV lateral or septal walls.
3. Focused HPI and Physical Examination
Key exam elements:
-
- Neuro: assessment of mental status and for focal deficits (maintain a high suspicion for ischemic and hemorrhagic strokes)
- Cardiac: confirm device hum, assess for HF signs (JVD, edema, dyspnea).
- GI: perform rectal exam if suspicion of bleeding.
- Skin: inspect the driveline exit site.
Assessment of Volume Status and Afterload
Centrifugal-flow devices, particularly HM3, are sensitive to preload, afterload, and volume status. LVAD flow, PI, and MAP together help identify hemodynamic abnormalities.
Table 3. Volume status and afterload assessment using LVAD parameters. Adapted from https://pmc.ncbi.nlm.nih.gov/articles/PMC9100630/.12
| Condition | Flow | PI | MAP | ||
| Hypovolemia | Mild | Normal to low | Low | Unchanged | Hypovolemia causes decreased LV filling which in mild cases causes decreased contractility. In extreme cases, suction events will occur and cause high pulsatility. |
| Severe | Low | Very high | Low | ||
| Hypervolemia | Mild | Normal to high | High | Unchanged | Increased LV pressure causes increased filling and contractility. If severe, will lead to RV failure and RV/LV interdependence, which will impair LV contractility. |
| Severe | Low | Low | Possibly low | ||
| Afterload
(HTN) |
Low | High | High | Increased afterload causes a disproportionate decrease in flow during diastole, which increases PI. | |
Key Patterns:
- Severe hypovolemia → low flow, very high PI, low MAP
- Severe hypervolemia → RV failure, low flow, low PI
- Hypertension → low flow, high PI, high MAP
Ultrasound Assessment
Point-of-care ultrasound (POCUS) is essential for evaluating suspected LVAD dysfunction. Standard cardiac views (PSLA, PSSA, A4C, subxiphoid) can assess:
- LV and RV morphology
- Inflow and outflow cannula position
- Pericardial effusion
- Global cardiac function
Advanced views can be used to identify inflow/outflow cannulas, RV function, tricuspid regurgitation, and aortic valve competency.
Table 4. Advanced Views of Point-of-Care Ultrasound for Patients with Left Ventricular Assist Device. Adapted from https://doi.org/10.1016/j.jemermed.2021.10.018.13
| POCUS Examination | Features | Views | Interpretation |
| Cardiac | RV size and function | PSLA, PSSA, and A4C | RV failure: increased size, reduced systolic function (TAPSE < 17 mm)
Tricuspid regurgitation: regurgitation flow on color-flow Doppler |
| Inflow cannula: position, flow, clot presence | PSLA, PSSA, and A4C | Thrombosis: presence of clots
Misalignment: inflow cannula not aligned with the mitral valve, or angulated toward or in contact with the walls of the left ventricle Suction event: deviation of septum to the left from usual flat and neutral position Cannula obstruction: turbulent flow on color-flow Doppler Pump malfunction: regurgitant flow on color-flow Doppler |
|
| Outflow cannula: position, flow, clot presence | High left PSLA or right parasternal | Thrombosis: presence of clots
Misalignment: end-to-end anastomosis of the outflow cannula to the mid-ascending aorta not aligned Cannula obstruction: turbulent flow on color-flow Doppler Pump malfunction: regurgitant flow on color-flow Doppler |
|
| Aortic Valve competency | PSLA | Aortic regurgitation: regurgitant flow on color flow-Doppler |
A4C = apical four chamber; PSLA = parasternal long axis; PSSA = parasternal short axis; RV = right ventricle; TAPSE = tricuspid annular plane systolic excursion.
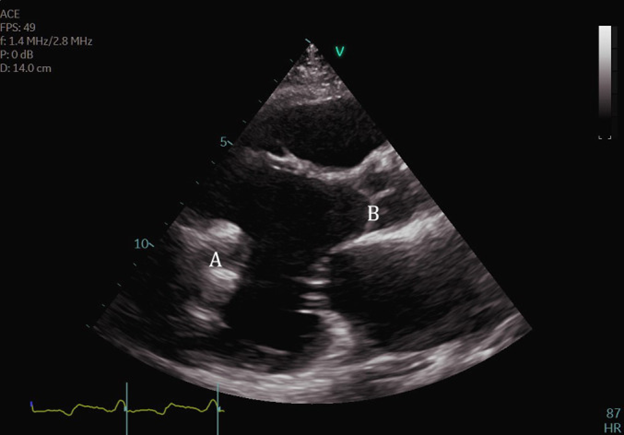
In practice, obtaining transthoracic ultrasound views of the LVAD inflow and outflow cannulas can be challenging due to distorted cardiac anatomy, poor acoustic windows, and imaging artifacts from the device itself. The inflow cannula position can sometimes be visualized in the PSLA (Figure 5) or PSSA views.
Figure 5. Transthoracic echocardiogram PLAX view demonstrating normal appearing inflow cannula at LV apex (A). Open access image reproduced from: https://pubmed.ncbi.nlm.nih.gov/39076924/.14
You can learn more about cardiac POCUS in LVAD patients here: https://www.youtube.com/watch?v=6OkbKawv0jo
4. Additional Diagnostic Workup
Useful adjunct tests include:
- EKG
- Chest X-ray
- CBC, CMP, BNP
- Coagulation studies: INR goal for most HM3 patients is 2.0-3.0
- Hemolysis labs: plasma-free hemoglobin, lactate dehydrogenase, haptoglobin
Management of LVAD-specific events
Suction Event
Overview: Inflow cannula becomes occluded by the LV lateral or septal walls.
Possible causes: hypovolemia, dysrhythmia, RV failure, cardiac tamponade.
Indicators:
- LVAD low flow alarm, fluctuating PI
- Leftward bowing of interventricular septum on TTE (hypovolemia or RV dilation)
- External compression of LV (tamponade)
Workup:
- Volume status assessment
- LVAD controller review
- TTE
Management:
- Hypovolemia: fluids (blood, crystalloid, colloid)
- RV failure: inotropic support (milrinone, dobutamine), volume optimization
- Tamponade (rare): pericardiocentesis
Pump thrombosis
Overview: Incidence is low since universal HM3 implantation (1.1% at 2 years).2
Possible causes: Often related to medication non-adherence or prolonged low flow state.
Indicators:
- Exam: evaluate for acute HF symptoms.
- LVAD may show power increase.
Workup:
- Labs: evidence of hemolysis.
- Imaging assessment of LVAD inflow and outflow (TTE is best, CXR, CTA).
- Cardiac catheterization with pump angiography for definitive diagnosis.
Management:
- Start a therapeutic heparin continuous infusion.
- Consider thrombolysis in select cases only after discussion with an LVAD expert.
- Pump exchange may be necessary in refractory cases.
Hypertension-Induced Low Flow
Overview: The HM3 is fairly susceptible to increased afterload, and MAP > 110 mmHg often causes low flow.
Possible causes: volume overload, pain, medication non-adherence.
Indicators:
- LVAD low flow alarm.
- Elevated MAP on invasive monitoring.
- LV dilation and rightward bowing of intraventricular septum on TTE.
- Possible arrhythmias due to subendocardial ischemia resulting from high afterload.
Workup:
- Assess blood pressure.
- Perform TTE: dilated LV, diminished aortic valve opening.
Management:
- Start antihypertensives and diuretics to target MAP < 90 mmHg.15
- IV vasodilators (nitroprusside, nitroglycerin, hydralazine, nicardipine) are recommended for acute ED management.15
Complete Device Failure
Overview: If no device hum is audible, assume the pump is off.
Possible causes: battery malfunction, driveline malfunction, actual pump failure.
Indicators:
- Exam: no audible device hum on auscultation, acute HF symptoms.
- Possible controller alarm (low flow, connect power, or connect driveline).
Workup:
- Reconnect power.
- Complete device inspection for disconnections or damage.
- Obtain TTE.
Management:
- Emergent consultation with the VAD team.
- Supportive care of HF physiology with inotropes, vasopressors.
- Start ACLS if indicated.
Aortic insufficiency
Overview: An increasingly recognized complication, with ~25% incidence in the first year after LVAD transplantation.16
Possible causes: Aortic valve fusion from chronic closure due to LV unloading, shear stress on the aortic valve due to LVAD outflow.
Indicators:
- Exam: acute HF symptoms.
- LVAD controller showing increased power and increased flow.
Workup:
- TTE: Aortic valve and LV function and morphology.
Management:
- LVAD speed adjustment in consultation with VAD specialist.
- Possible aortic valve replacement.
RV Failure
Overview: Can develop in 20-30% of LVAD recipients.17
Possible causes: systemic hypotension → RV hypoperfusion, leftward septal bowing due to changes in LVAD flow.
Workup:
- Exam: JVD, edema, ascites .
- Labs: for markers of hepatic or renal congestion.
- TTE: ↓ RV function, ↑ RV/LV ratio (> 0.75), ↓ tricuspid annulus S’, ↓RV strain index.
- PA catheter insertion remains the gold standard for assessment of right heart hemodynamics.
Management:
- Target euvolemia via diuresis or dialysis.
- Start an inotropic agent (dobutamine, epinephrine).
- Consider inhaled pulmonary vasodilators.
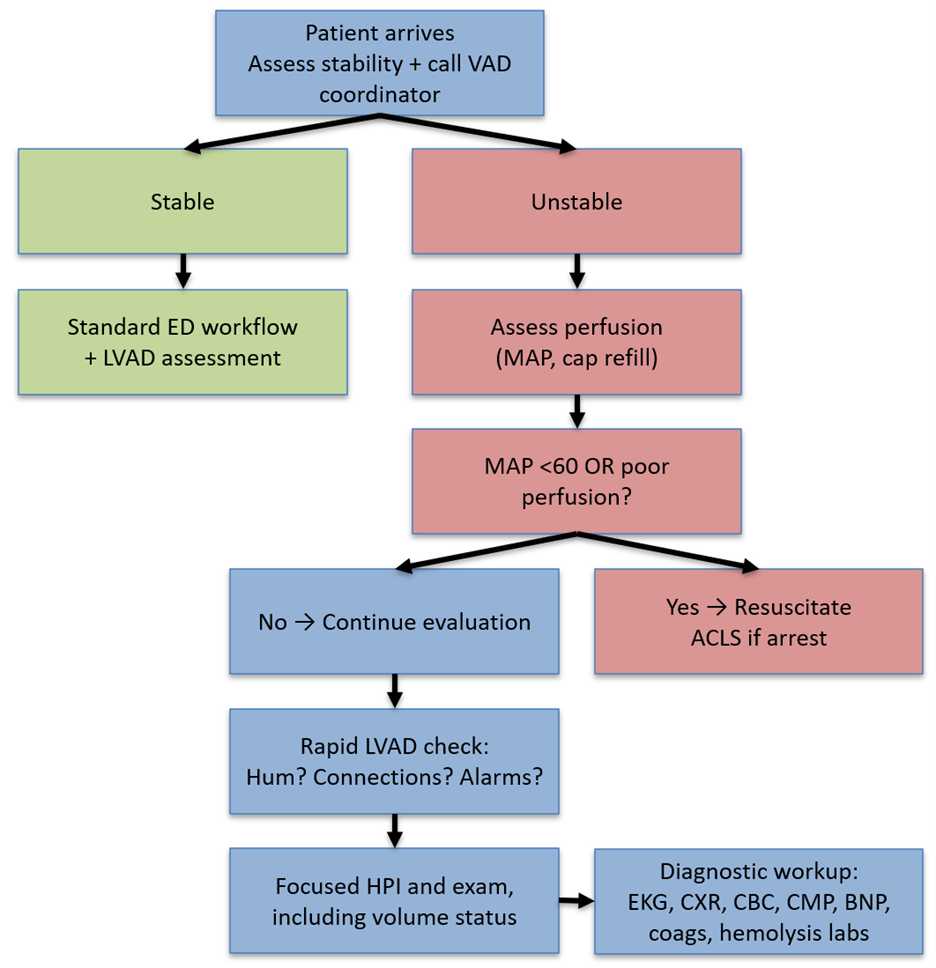
Figure 6. Initial approach to the LVAD patient in the ED.
Management of LVAD-associated events
GI Bleeding
Overview: Still the most common overall complication, but less frequent with HM3.6
Reasons:
- Inherent need for anticoagulation.
- Non-pulsatile blood flow → angiodysplasias such as AVMs.
- Acquired von Willebrand syndrome from shear stress on red blood cells from the LVAD pump.
Workup:
- Exam: melena, hematochezia
- CT angiography
Management:
- Consider blood transfusion.
- Initiate proton pump inhibitor or histamine-2 receptor blocker.
- Consult with GI and/or IR.
- Discuss with the admitting team about antiplatelet and anticoagulation strategy (patients with HM3 have a relatively lower risk for pump thrombosis than earlier devices).
CVA (Ischemic and Hemorrhagic):
Overview: HM3 significantly lowers stroke risk, but both ischemic and hemorrhagic events still occur, with roughly equal incidence of each.2,6,18
Reasons:
- Ischemic: LVAD or valvular thromboembolism
- Hemorrhagic: from systemic anticoagulation
Workup:
- Exam: stroke symptoms on standard assessment
- CT and CT angiography head and neck
Management:
- Neurology and neurosurgical consultation is critical due to nuanced management.
- Hemorrhagic stroke management depends on the type of bleed:19
- Intraparenchymal: poor outcomes regardless of surgical intervention or anticoagulation reversal.
- Subdural: good outcomes with both surgical intervention and anticoagulation reversal.
- Subarachnoid: generally good outcomes regardless of surgical management or anticoagulation reversal.
- Anticoagulation reversal does not appear to increase pump thrombosis in the HM3 cohort.
- Thrombolytics are usually contraindicated.20
- Thrombectomy remains the treatment of choice for LVO.
Infection
Overview: There has been no significant reduction in infection rates with HM3, and infection remains the most common complication within the first 3 months post-LVAD insertion.6 Possible causes: Driveline infections are most common, followed by pump pocket infection. These infections can provoke bacteremia, endocarditis, and mediastinitis.21
Workup:
- Exam: may reveal cellulitis at driveline exit site
- SIRS positive vitals and labs
Management:
- Start broad-spectrum antibiotics.
- Obtain cultures (driveline exit site, blood).
- Obtain CT chest, abdomen, and pelvis with IV contrast.
Arrhythmia
Overview: ventricular fibrillation (VF), ventricular tachycardia (VT), and atrial fibrillation are most common, followed by atrial flutter and AV nodal reentry tachycardia (AVNRT).
Workup:
- EKG
- Labs: assess for electrolyte aberrancies.
Management:
- Treat arrhythmias as you normally would.
- Unstable VT/VF → cardioversion/ defibrillation
- Atrial fibrillation and flutter → rate/ rhythm control
Management of the Unresponsive LVAD Patient
An unresponsive LVAD patient can crash for all the usual ED reasons, plus a handful of LVAD-specific problems. The first decision-making branch point hinges on the question: Is the patient perfusing?
- Auscultate for device hum.
- Obtain MAP with manual BP and Doppler.
- Perform a bedside ultrasound to assess cardiac function.
If perfusion is adequate, search for non-cardiac causes (hypoglycemia, stroke, intoxication, sepsis, hypoxia, etc.) If perfusion is inadequate, initiate standard ACLS. The risk of dislodging the LVAD during chest compressions is low and is absolutely worth the benefit of providing CPR.22 The American Heart Association guidelines (found here) provide a useful framework for assessing the unresponsive LVAD patient.22
Disposition
- Most LVAD-related ED visits require admission for evaluation by a multidisciplinary team, which may include cardiology, cardiothoracic surgery, and critical care.
- Patients presenting to non-LVAD centers should be transferred to an LVAD program.
What Is Next for LVAD Technology?
The universal adoption of HM3 has already led to significant reduction in morbidity and improved quality of life. Solutions to many persistent challenges are under actively being developed.
- Remote monitoring with automated speed adjustment: advancements in the integration of LVAD technology with other implantable cardiac monitoring devices (CardioMEMs) will allow for active adjustment in LVAD speed in response to the patient’s hemodynamics.1
- Infection reduction: fully implantable, wirelessly powered devices are in development.23
- Lower intensity anticoagulation strategies: HM3 patients may have lower target INR (1.5-1.9) and may not need daily aspirin as previously thought.24,25
- Automated embolism detection: integrated automated systems are in development to detect clots and initiate therapy earlier.23
Take-Home Points
- The HM3 device is currently the only FDA-approved durable LVAD in the U.S., and 1-and 5-year survival rates are approaching heart transplantation outcomes.
- With the increase in LVAD as destination therapy and improved survival, EM clinicians should expect to manage LVAD patients.
- While the rates of complications are improving, bleeding, infection, and HF are still the most common ED presentations.
- When managing the unstable LVAD patient, prioritize treating the underlying physiology (inotropes for HF, volume optimization, antibiotics for infection, anticoagulation for strokes), perform CPR when needed, and involve the LVAD team early.
- Point-of-care TTE and interrogation of the LVAD controller remain key steps in identifying life-threatening complications.
References
- Moeller CM, Valledor AF, Oren D, Rubinstein G, Sayer GT, Uriel N. Evolution of Mechanical Circulatory Support for advanced heart failure. Progress in Cardiovascular Diseases. 2024;82:135-146. doi:10.1016/j.pcad.2024.01.018
- Mehra MR, Uriel N, Naka Y, et al. A Fully Magnetically Levitated Left Ventricular Assist Device — Final Report. New England Journal of Medicine. 2019;380(17):1618-1627. doi:10.1056/NEJMoa1900486
- HeartMate 3 LVAD System Information | Abbott. Accessed November 11, 2025. https://www.cardiovascular.abbott/us/en/hcp/products/heart-failure/left-ventricular-assist-devices/heartmate-3/about/system-overview.html
- Yuzefpolskaya M, Schroeder SE, Houston BA, et al. The Society of Thoracic Surgeons Intermacs 2022 Annual Report: Focus on the 2018 Heart Transplant Allocation System. The Annals of Thoracic Surgery. 2023;115(2):311-327. doi:10.1016/j.athoracsur.2022.11.023
- Sennhauser S, Sridharan L. Left Ventricular Assist Device Emergencies: Diagnosis and Management. Critical Care Clinics. 2024;40(1):159-177. doi:10.1016/j.ccc.2023.06.004
- Meyer DM, Nayak A, Wood KL, et al. The Society of Thoracic Surgeons Intermacs 2024 Annual Report: Focus on Outcomes in Younger Patients. The Annals of Thoracic Surgery. 2025;119(1):34-58. doi:10.1016/j.athoracsur.2024.10.003
- Salewski C, Rustenbach CJ, Marinos SL, Sandoval Boburg R, Schlensak C, Radwan M. Left Ventricular Assist Device (LVAD)-Related Major Adverse Events Account for a Low Number of Emergency Room Admissions in HeartMate 3TM Patients—A 10-Year Retrospective Study. Biomedicines. 2025;13(7):1702. doi:10.3390/biomedicines13071702
- Tainter CR, Braun OÖ, Teran F, et al. Emergency department visits among patients with left ventricular assist devices. Intern Emerg Med. 2018;13(6):907-913. doi:10.1007/s11739-017-1776-8
- Cai J, Xia W, Greenberg P, Okwuosa I, Setoguchi S, Akhabue E. Relation of Sociodemographic Factors With Primary Cause of Hospitalization Among Patients With Left Ventricular Assist Devices (from the National Inpatient Sample 2012 to 2017). The American Journal of Cardiology. 2022;180:81-90. doi:10.1016/j.amjcard.2022.06.047
- McKillip RP, Gopalsami A, Montoya M, et al. Analysis of Patients with Ventricular Assist Devices Presenting to an Urban Emergency Department. Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health. 2018;19(6). doi:10.5811/westjem.2018.8.38851
- Lee P, Ghobrial M, Greider K, et al. No Pulse? No Problem. Navigating LVAD Emergencies in the Department. The Journal of Emergency Medicine. Published online November 2, 2025. doi:10.1016/j.jemermed.2025.10.041
- Troutman GS, Genuardi MV. Left Ventricular Assist Devices: A Primer for the Non-Mechanical Circulatory Support Provider. J Clin Med. 2022;11(9):2575. doi:10.3390/jcm11092575
- Pek JH, Teo LYL. Point-of-Care Ultrasound in the Evaluation of Patients with Left Ventricular Assist Devices at the Emergency Department. The Journal of Emergency Medicine. 2022;62(3):348-355. doi:10.1016/j.jemermed.2021.10.018
- Anand S, Barry T, Arsanjani R, LeMond L. Echocardiography in Cardiac Assist Devices. Rev Cardiovasc Med. 2022;23(7):253. doi:10.31083/j.rcm2307253
- Management of Hypertension in Patients With Ventricular Assist Devices: A Scientific Statement From the American Heart Association | Circulation: Heart Failure. Accessed November 15, 2025. https://www.ahajournals.org/doi/full/10.1161/HHF.0000000000000074?rfr_dat=cr_pub++0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org
- Bouabdallaoui N, El-Hamamsy I, Pham M, et al. Aortic regurgitation in patients with a left ventricular assist device: A contemporary review. The Journal of Heart and Lung Transplantation. 2018;37(11):1289-1297. doi:10.1016/j.healun.2018.07.002
- Rich JD, Gosev I, Patel CB, et al. The incidence, risk factors, and outcomes associated with late right-sided heart failure in patients supported with an axial-flow left ventricular assist device. J Heart Lung Transplant. 2017;36(1):50-58. doi:10.1016/j.healun.2016.08.010
- Kirklin JK, Naftel DC, Myers SL, Pagani FD, Colombo PC. Quantifying the impact from stroke during support with continuous flow ventricular assist devices: An STS INTERMACS analysis. The Journal of Heart and Lung Transplantation. 2020;39(8):782-794. doi:10.1016/j.healun.2020.04.006
- Lai GY, Devlin PJ, Kesavabhotla K, et al. Management and outcome of intracranial hemorrhage in patients with left ventricular assist devices. Journal of Neurosurgery. 2019;132(4):1133-1139. doi:10.3171/2018.12.JNS182467
- Rettenmaier LA, Garg A, Limaye K, Leira EC, Adams HP, Shaban A. Management of Ischemic Stroke Following Left Ventricular Assist Device. Journal of Stroke and Cerebrovascular Diseases. 2020;29(12):105384. doi:10.1016/j.jstrokecerebrovasdis.2020.105384
- Blanco-Guzman MO, Wang X, Vader JM, Olsen MA, Dubberke ER. Epidemiology of Left Ventricular Assist Device Infections: Findings From a Large Nonregistry Cohort. Clinical Infectious Diseases. 2021;72(2):190-197. doi:10.1093/cid/ciaa011
- Givertz MM, DeFilippis EM, Colvin M, et al. HFSA/SAEM/ISHLT clinical expert consensus document on the emergency management of patients with ventricular assist devices. The Journal of Heart and Lung Transplantation. 2019;38(7):677-698. doi:10.1016/j.healun.2019.05.004
- Kozakov K, Provaznik Z, Schmid C, Camboni D. Advancing LVAD Technology: Overcoming Challenges and Shaping the Future of Mechanical Circulatory Support. J Clin Med. 2024;13(24):7813. doi:10.3390/jcm13247813
- Netuka I, Ivák P, Tučanová Z, et al. Evaluation of low-intensity anti-coagulation with a fully magnetically levitated centrifugal-flow circulatory pump—the MAGENTUM 1 study. The Journal of Heart and Lung Transplantation. 2018;37(5):579-586. doi:10.1016/j.healun.2018.03.002
- 25. Mehra MR, Netuka I, Uriel N, et al. Aspirin and Hemocompatibility Events With a Left Ventricular Assist Device in Advanced Heart Failure: The ARIES-HM3 Randomized Clinical Trial. JAMA. 2023;330(22):2171-2181. doi:10.1001/jama.2023.23204




