Today on the emDOCs cast with Brit Long, MD (@long_brit), we cover asthma exacerbation management. For more on the ED evaluation, take a listen to Part 1.
Episode 106: Asthma Exacerbation Part 2
Please see Part 1 for the ED evaluation.
Management:
- Based on severity: mild, moderate, severe.

- Oxygen supplementation
- Provide for those with hypoxia; target saturation 93-95%. Hyperoxia associated with worse outcomes.
- Bronchodilators
- First line therapies; treat bronchial hyperreactivity and reduce or even reverse airflow obstruction.
- Include short acting beta-2 agonists (SABA) and ipratropium bromide. Delivery can be a metered dose inhaler or gas driven nebulizer; current evidence does not demonstrate a difference in patient centered outcomes between the two routes. MDI recommended if possible. In severe exacerbation, continuous nebulized therapy is recommended.
- SABAs stimulate airway beta-2 receptors; time of onset is within seconds to minutes. The peak effect approaches 30 minutes, with a half-life of 4-6 hours.
- Albuterol is the most common SABA utilized in the ED; for severe asthma exacerbation, provide continuous nebulized albuterol at a dose of 10-20 mg for 1 hour (NNT of 10 to reduce hospitalization).
- Long-acting beta-2 agonists (LABA) include salmeterol and formoterol provide close to 12 hours of bronchodilation. LABAs are typically combined with an inhaled corticosteroid for therapy, and these can be considered for patients as a discharge prescription for maintenance therapy.
- Inhaled epinephrine may assist patients who have not improved with other SABA agents due to its alpha activity reducing airway edema, but current evidence has not demonstrated improved efficacy in comparison against SABA therapy.
- Anticholinergics
- Ipratropium bromide inhibits muscarinic acetylcholine receptors in the pulmonary smooth muscle and results in bronchodilation. The time of onset approximates 15 minutes, and the peak effect is 60-90 minutes with a half-life of 6-8 hours. Ipratropium is administered in doses of 0.5-2 mg for the first hour.
- Use of ipratropium has been associated with reduced exacerbations, hospital admission, and length of stay in asthma; NNT 11 to reduce hospitalization in acute asthma.
- Corticosteroids
- Upregulate beta receptors and reduce airway inflammation.
- Current guidelines recommend corticosteroids in those with moderate or severe exacerbation and those who do not initially respond to SABA therapy. Associated with over a 50% reduction in treatment failure and a NNT 9 to prevent one treatment failure. Reduce relapse rates and hospital length of stay with a NNT 8.
- Administer within first hour.
- Controversy regarding the optimal steroid, dose, administration route, and treatment duration. PO and parenteral steroids demonstrate similar bioavailability and patient outcomes, but PO steroids are less invasive and less expensive. For critically ill patients who cannot tolerate PO administration, parenteral treatment is recommended.
- Inhaled corticosteroids administered with inhaled albuterol can improve smooth muscle relaxation and airway function.
- No benefit with systemic doses over prednisone 2 mg/kg per day or equivalent including treatment failure, need for airway intervention, or length of stay, but higher doses are associated with increased risk of adverse events including myopathy, hyperglycemia, infection, gastrointestinal bleeding, and neurologic effects.
- Magnesium
- IV administration may result in pulmonary smooth relaxation. It may improve pulmonary function and reduce need for hospital admissions.
- GINA guidelines recommend its use in patients with severe exacerbations.
- Dosing is 2g IV administered over 20 minutes; may be repeated twice.
- Possible adverse events include weakness, hypotension, flushing, and changes in heart rate.
- Inhaled administration is controversial, with literature to date suggesting no benefit.
- Parenteral beta agonist therapy
- Include epinephrine and terbutaline; potent bronchodilators and may decrease airway edema, mucous production, and inflammation. No high-quality prospective data supporting their use in severe exacerbation.
- Epinephrine is not recommended for routine use as a first-line therapy but should be considered in doses of 0.3-0.5 mg intramuscular in the anterolateral thigh every 20 minutes for 3 doses in those with severe asthma exacerbation who fail other therapies, or those with anaphylaxis or angioedema. For severe hypotension or refractory to IM administration, epinephrine IV 5-20 micrograms every 2-5 minutes should be considered.
- Terbutaline is a β2 agonist. It may be administered via inhalation or the subcutaneous or IV route. However, literature does not demonstrate improved patient outcomes when terbutaline is compared to standard SABAs.
- Ketamine
- Dissociative analgesic that may be used in patients who are refractory to other therapies. Rapid onset of action within 60 seconds and a distribution of 7 to 11 minutes. Ketamine is an N-methyl-D-aspartic acid (NMDA) receptor antagonist in the lung parenchyma, which can reduce pulmonary edema and bronchoconstriction; may reduce reduce production of nitric oxide, which reduces bronchospasm.
- Ultimately, ketamine can reduce airway hyperinflammation and hyperreactivity while decreased bronchospasm, with studies finding improved pulmonary function, reduced oxygen requirement, and decreased requirement for invasive ventilation.
- Administer only with appropriate monitoring.
- Two dosing strategies: sub-dissociative dose ketamine (0.05-0.4 mg/kg/hr) is used to reduce bronchospasm and improve pulmonary function while not sedating the patient, and dissociative dosed ketamine (0.5-2.0 mg/kg) can be used for delayed sequence intubation (DSI) or induction for rapid sequence intubation.
- Ketamine can also increase bronchial secretions and relieve mucous plugs.
- Heliox
- Mixture of helium and oxygen that can reduce airflow turbulence through narrow airways. It may also improve ventilation/perfusion matching and improve elimination of carbon dioxide.
- Controversial studies suggest that heliox-driven bronchodilation increases forced expiratory volume, forced vital capacity, and expiratory flow rate, with reduced ED admissions.
- If utilized, should be considered as an adjunct early in the patient course prior to increased oxygen requirements.
- Do not use routinely.
- Antibiotics
- Studies have evaluated azithromycin and other antibiotics; no benefit compared to placebo.
- Reserve for patients with evidence of bacterial infection (systemic symptoms of pneumonia such as fever, consolidation on x-ray).
- NIPPV
- NIPPV may be effective in those with severe asthma exacerbation and respiratory distress by reducing the work of breathing and improving alveolar recruitment.
- Limited prospective data demonstrating benefit; a large retrospective study of patients admitted to the critical care setting found NIPPV reduced intubation and mortality.
- Consider NIPPV in those with severe respiratory distress who do not respond to other therapies, as NIPPV can improve ventilation, and there is little harm.
- Close monitoring of the patient is necessary to ensure improvement.
- Absolute contraindications include cardiac or respiratory arrest, while relative contraindications include the patient who is uncooperative, has copious secretions, has a deformity of the face or upper airway, and recent esophageal trauma or surgery. Altered mental status, pH < 7.25, and hypercarbia are not contraindications if the clinician can closely monitor the patient. NIV can improve mental status in patients with hypercarbia, as NIPPV improves ventilation.
- BPAP provides an inspiratory pressure and expiratory pressure, which likely is more beneficial compared to CPAP in obstructive lung disease (problem with ventilation rather than oxygenation except in those with respiratory failure).
- Initial settings should include an inspiratory pressure support of 5-10 mm Hg and PEEP of 3-5 mm Hg. If titrating, the inspiratory pressure should be increased while maintaining PEEP.
- HFNC may assist in those unable to tolerate a face mask or with contraindications to NIPPV.
- Endotracheal Intubation
- Endotracheal intubation and mechanical ventilation are reserved for those with progressing respiratory distress who fail typical therapies and NIV, those with respiratory or cardiac arrest, and those with altered mental status/coma.
- Airway manipulation may worsen bronchospasm and result in laryngospasm. Mortality rates reach 20% in patients intubated with obstructive lung disease.
- Consider as a difficult airway, with the most experienced operator performing the procedure.
- Maximal preoxygenation and rapid sequence intubation are recommended.
- Ketamine is an optimal induction agent (1-2 mg/kg IV), as it relaxes bronchial smooth muscle and has analgesic and sedative properties. Propofol possesses some bronchodilating effects but can result in hypotension.
- Paralysis recommended to include first pass success (rocuronium 1.2 mg/kg IV).
- Optimize prior to intubation; administer fluid bolus and have vasopressors ready.
- Mechanical Ventilation
- Settings must prevent hyperinflation and auto-PEEP, which may result in hemodynamic collapse and barotrauma.
- Ventilator settings should utilized a reduced respiratory rate and tidal volume, shortened inspiratory and lengthened exhalation times, resulting in permissive hypercapnia.
- VC, RR 6-10 breaths per minute, TV 6-8cc/kg ideal body weight, inspiratory flow rate 80-120 L/min, inspiration-to-expiration ratio of > 1:4
- Administer scheduled inline, inhaled bronchodilator therapy.
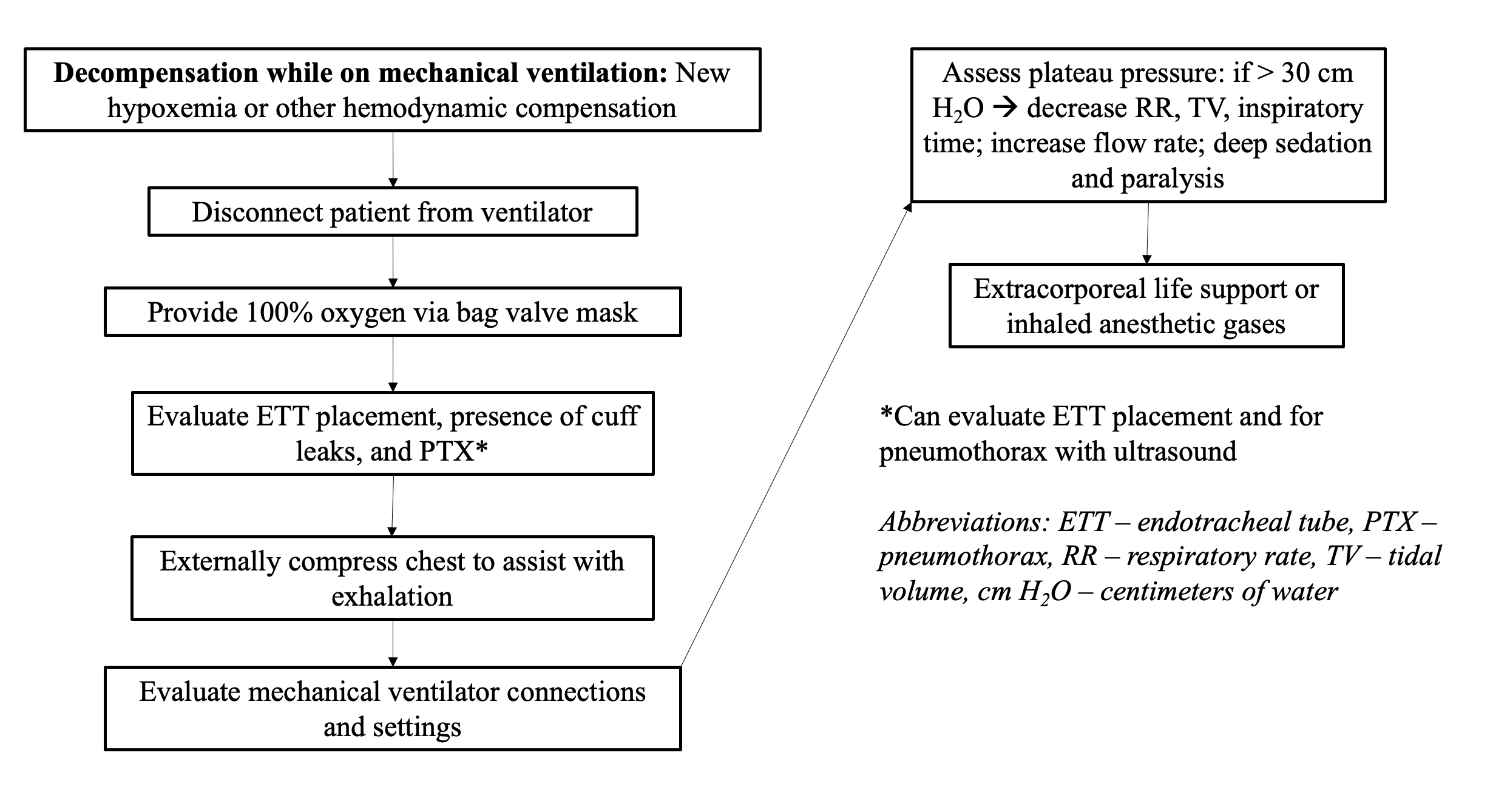
- Deep sedation is recommended to improve patient lung mechanics. If decompensates, use DOPES/DOTTS.
- Extracorporeal Membrane Oxygenation
- Final option in treatment-refractory patients.
- Consider in patients on mechanical ventilation with inadequate oxygenation or acidosis.
- Requires significant resources and support staff present in select centers.
Disposition
- Based on treatment response, clinical course, and ability to follow-up.
- Patients who improve, have no evidence of respiratory distress, and have follow-up can be discharged with oral steroids for a 5-day course, along with a SABA MDI with spacer (4 puffs every 3-4 hours).
- Inhaled steroids should be strongly considered for patients with asthma as a daily therapy, which is associated with greater symptom control and reduced asthma exacerbations, ED visits, and need for hospitalization. Current guidelines recommend use of inhaled steroids in asthma.
- Patients with continued symptoms or cardiorespiratory distress should be admitted.
- Asthma care plans are key parts of outpatient therapy. They improved patient outcomes and medication adherence while reducing exacerbation recurrence.
- Ensure follow-up within one week if discharging.
Part 2 Summary:
- ED management includes supplemental oxygen if oxygen saturation < 90%. Inhaled SABAs and SAMAs should be administered with MDI or nebulization. In moderate to severe exacerbation, continuous nebulization with SABAs and SAMAs for 1 hour is recommended.
- Systemic steroids should be administered within 1 hour of presentation via the oral route if able or intravenous route in patients with moderate or severe exacerbation. Inhaled steroids are a key component of outpatient management.
- Magnesium IV should be considered in those with severe exacerbation. Parenteral β2 agonists including epinephrine or terbutaline can also be considered in patients who fail to respond to standard therapies.
- Ketamine may be useful in select cases.
- Antibiotics such as azithromycin and inhaled magnesium are not associated with improved patient outcomes during an acute asthma exacerbation.
- Noninvasive positive pressure ventilation can be used in those with significant respiratory distress; endotracheal intubation and mechanical ventilation are necessary for those with respiratory failure.
- Ventilator settings must prevent hyperinflation and auto-PEEP, which may result in hemodynamic collapse and barotrauma.
- Disposition is based on treatment response, clinical course, and ability to follow-up.
References:
- Global Initiative for Asthma (GINA). 2022 GINA Report, Global Strategy for Asthma Management and Prevention. 2022. Available at: https://ginasthma.org/gina-reports/. Accessed June 12, 2023.
- Long B, Lentz S, Koyfman A, Gottlieb M. Evaluation and management of the critically ill adult asthmatic in the emergency department setting. Am J Emerg Med. 2021 Jun;44:441-451.
- Rowe BH. Continuous versus intermittent beta-agonists for acute asthma. Cochrane Database Syst Rev. 2011;(4):CD001115.
- Stoodley RG, Aaron SD, Dales RE. The role of ipratropium bromide in the emergency management of acute asthma exacerbation: a metaanalysis of randomized clinical trials. Ann Emerg Med. 1999 Jul;34(1):8-18.
- Rodrigo G, Rodrigo C, Burschtin O. A meta-analysis of the effects of ipratropium bromide in adults with acute asthma. Am J Med. 1999 Oct;107(4):363-70.
- Kirkland SW, Vandenberghe C, Voaklander B, et al. Combined inhaled beta-agonist and anticholinergic agents for emergency management in adults with asthma. Cochrane Database Syst Rev. 2017 Jan 11;1(1):CD001284.
- Rowe BH, Spooner C, Ducharme FM, et al. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002178.
- Crossingham I, Turner S, Ramakrishnan S, et al. Combination fixed-dose beta agonist and steroid inhaler as required for adults or children with mild asthma. Cochrane Database Syst Rev. 2021 May 4;5(5):CD013518.
- Kew KM, Kirtchuk L, Michell CI. Intravenous magnesium sulfate for treating adults with acute asthma in the emergency department. Cochrane Database Syst Rev. 2014 May 28;(5):CD010909.
- Goodacre S, Cohen J, Bradburn M, et al; 3Mg Research Team. Intravenous or nebulised magnesium sulphate versus standard therapy for severe acute asthma (3Mg trial). Lancet Respir Med. 2013;1(4):293-300.
- Knightly R, Milan SJ, Hughes R, et al. Inhaled magnesium sulfate in the treatment of acute asthma. Cochrane Database Syst Rev. 2017;11:Cd003898.
- Travers AH, Milan SJ, Jones AP, et al. Addition of intravenous beta(2)-agonists to inhaled beta(2)-agonists for acute asthma. Cochrane Database Syst Rev. 2012 Dec 12;12:CD010179.
- Johnston SL, Szigeti M, Cross M, et al; AZALEA Trial Team. Azithromycin for acute exacerbations of asthma: the AZALEA randomized clinical trial. JAMA Intern Med. 2016;176(11):1630-1637.
- Althoff MD, Holguin F, Yang F, et al. Noninvasive Ventilation Use in Critically Ill Patients with Acute Asthma Exacerbations. Am J Respir Crit Care 2020 Dec 1;202(11):1520-1530.




