Today on the emDOCs cast with Brit Long, MD (@long_brit), we cover asthma exacerbation focusing on the history, examination, and ED evaluation. Part 2 will cover management.
Episode 105: Asthma Exacerbation Part 1
Introduction
- Asthma is an obstructive pulmonary condition with recurrent exacerbations. Over 25 million Americans suffer from asthma, and asthma exacerbation is responsible for over 2 million ED visits annually in the U.S.
- Asthma is more common in adult women compared to men, but in pediatric patients, asthma affects males more than females.
- Over 3,500 patients die from asthma exacerbation every year.
Definition:
- The Global Initiative for Asthma (GINA) defines asthma as an allergic disease that typically begins as a child, marked by bronchial hyperresponsiveness, vascular permeability, bronchial smooth muscle spasm, and inflammatory mediator release.
- Exacerbations are episodic and vary in severity. Most commonly present with coughing, wheezing, chest tightness, and shortness of breath. Triggers include allergens, infection, emotional state, exercise, or exposure to an inhaled agent, but these exacerbations usually resolve completely with therapy or even spontaneously.
Initial ED Evaluation:
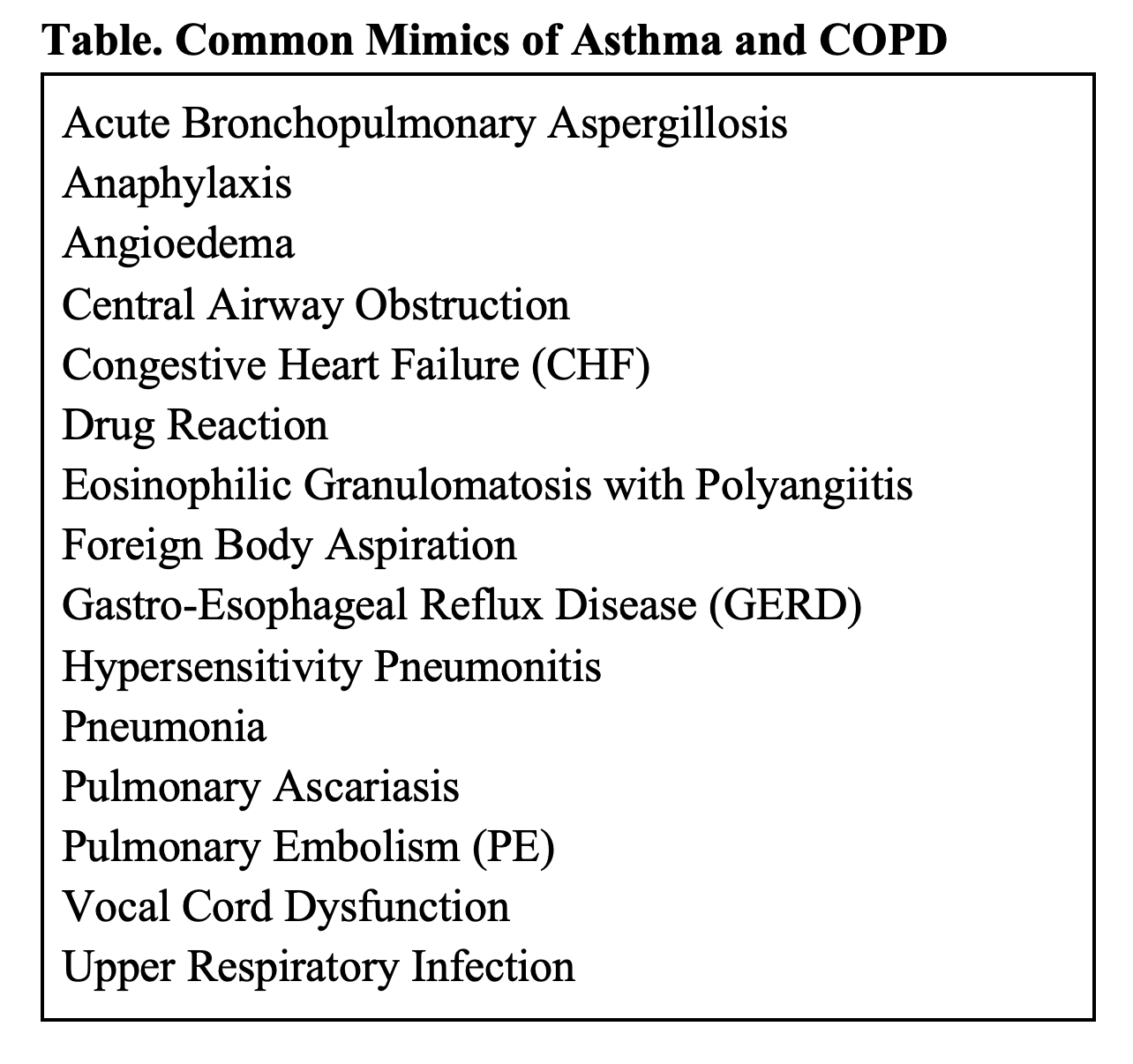
- History and exam focus on assessing severity of exacerbation and evaluating for mimics (not all that wheezes is asthma; many conditions may mimic asthma).
- History: evaluate time of symptom onset, etiology/underlying cause, presence of systemic symptoms (i.e., fevers, chills, rigors), attempted treatments prior to arrival, and prior care for the disease.
- Historical factors including recent ED visits or hospital admissions for obstructive lung disease, increased use of short-acting beta agonist therapy, recent steroid use, recent antibiotic use, previous airway interventions (NIV, endotracheal intubation), and prior ICU admission associated with uncontrolled disease and greater risk of severe exacerbation.
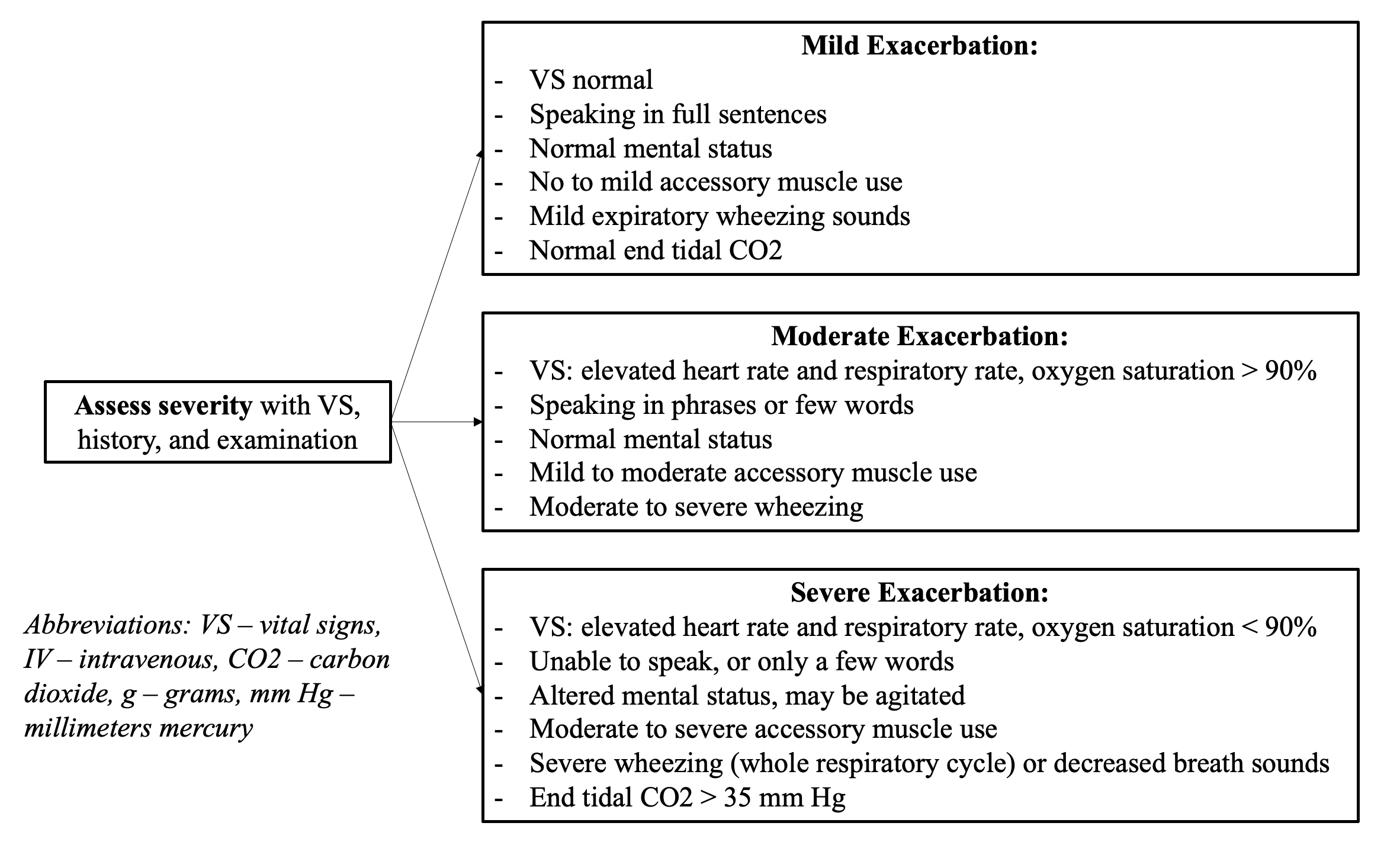
- Presentation: cough, wheezing, dyspnea, and chest tightness. Inability to speak more than a few words, agitation, respiratory distress, and air hunger reflect a severe exacerbation.
- Physical exam: focus on cardiorespiratory status; vital signs (oxygenation, HR, and RR); and the presence of air movement, fevers, wheezing, cyanosis, and mental status.
- Severe exacerbation: tachypnea, tachycardia, hypoxemia, use of accessory muscles, speaking one to two words at a time, tripod position, and inability to lie flat. Absence of these findings cannot exclude severe exacerbation but are suggestive if present.
- Signs suggesting cardiorespiratory distress and imminent arrest: bradycardia, cyanosis, decreased mental status, inability to maintain respiratory effort.
Testing:
- No laboratory test can diagnose asthma, but labs can assist evaluating for other conditions (e.g., BNP/troponin for cardiac, CBC for anemia, viral testing).
- Sputum testing not recommended in the ED setting.
- Blood gas:
- ABG: do not obtain routinely. Risk of aneurysm formation, arterial injury, infection, and even loss of limb. Consider for those requiring prolonged respiratory support, respiratory failure, and mechanical ventilation.
- Obtain VBG for those with severe exacerbation, those who fail to respond to initial therapies, visible respiratory distress/fatigue, or evidence of hypercarbia (i.e., altered mental status, somnolence).
- VBG is an effective screen for pCO2. If over 45 mm Hg, hypercarbia present. pCO2 will be low early in exacerbation. If using VBG and pCO2, trends are most helpful, in combination with clinical evaluation.
- Clinician assessment at the bedside should remain the focus.
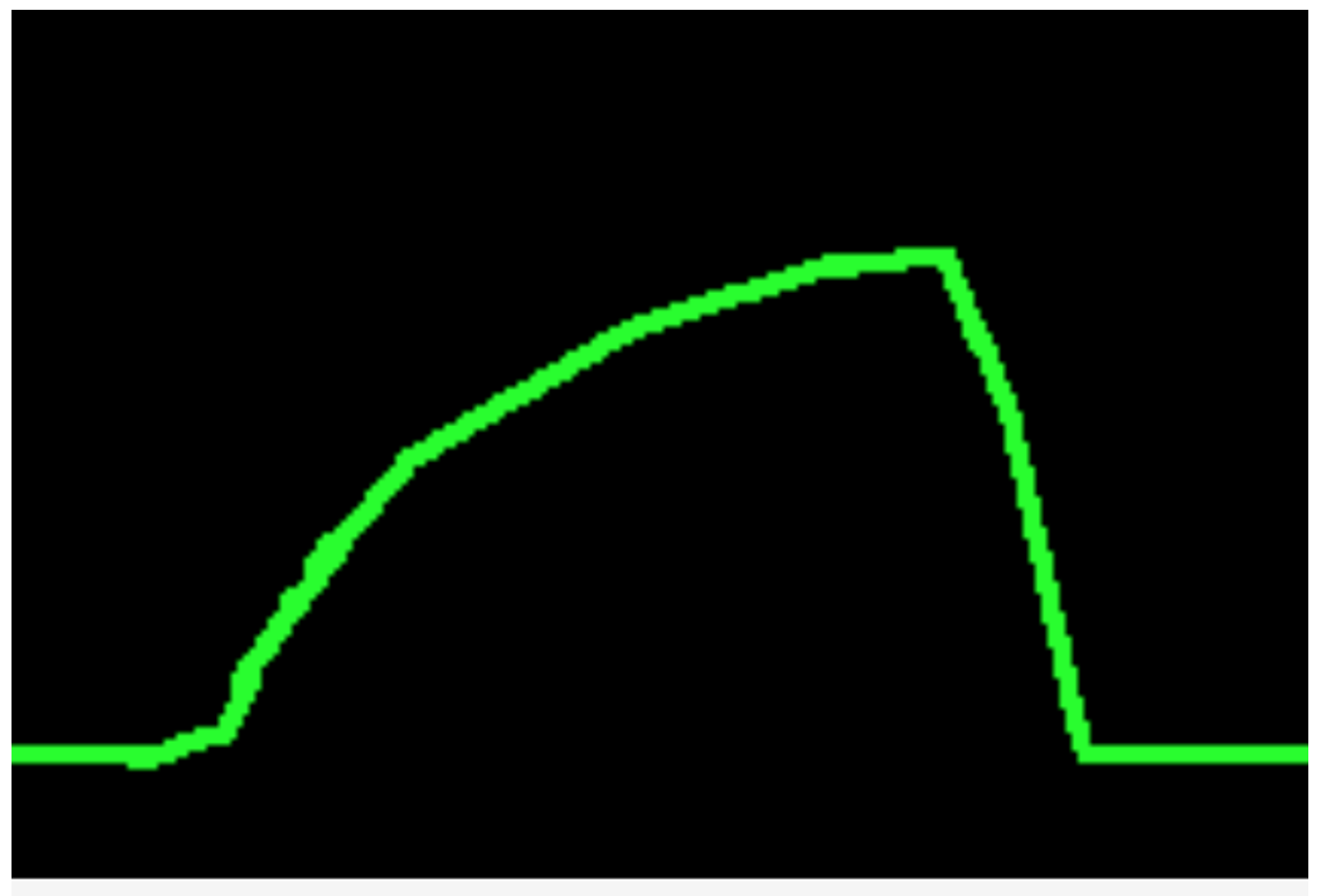
- Capnography: May assist in risk stratification. Lower values early in exacerbation common, but elevated levels suggest hypercarbia. Airway obstruction from bronchospasm can result in increased slope of phase 3 with an increased alpha angle similar to a shark fin.
- Spirometry: Component of GINA guidelines for diagnosis, classification, treatment. May be used by patient at home. Performing spirometry in the ED is challenging, particularly in the undifferentiated patient. Patients with severe exacerbations likely will not be able to cooperate to perform spirometry.
- Radiography: Routine use not recommended. Consider chest x-ray if concern for pneumonia, in extremis, not responding to initial therapies, concern for other diagnosis, or new onset wheezing.
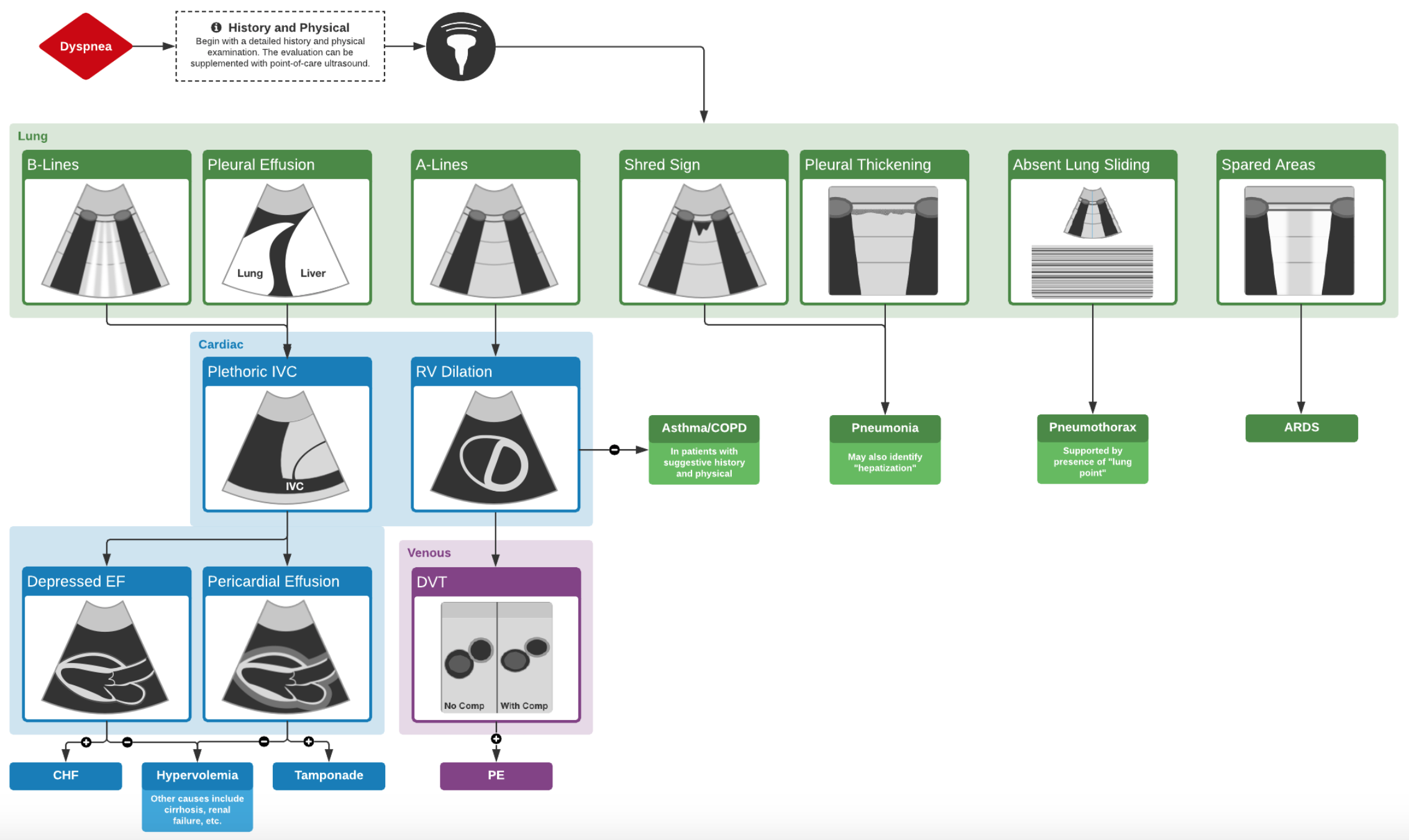
- Ultrasound: Rapid, reliable. Evaluate lungs and heart (pneumothorax, pleural/pericardial effusion, pneumonia, RV strain, etc.).
- Several protocols available: BLUE, FULL, LUCI.
- Reliable in assessing for cause of dyspnea/respiratory complaints.
Stay tuned for part 2 on management!
Part 1 Summary:
- Asthma is a chronic obstructive airway disease with recurrent exacerbations ranging in severity.
- Diagnosis is based on the history and examination, which also determine the severity of the exacerbation.
- Not all that wheezes is asthma. Consider mimics.
- VBG is an effective screen for pCO2. ABG is not routinely necessary.
- End tidal CO2 monitoring can detect the severity of airway obstruction and assess treatment response.
- Chest x-ray may be used in those with severe respiratory distress and those who fail to respond to standard therapies to evaluate for other conditions including pneumonia or pneumothorax. US can assist.
References:
- Global Initiative for Asthma (GINA). 2022 GINA Report, Global Strategy for Asthma Management and Prevention. 2022. Available at: https://ginasthma.org/gina-reports/. Accessed June 12, 2023.
- Long B, Lentz S, Koyfman A, Gottlieb M. Evaluation and management of the critically ill adult asthmatic in the emergency department setting. Am J Emerg Med. 2021 Jun;44:441-451.
- Rowe BH. Continuous versus intermittent beta-agonists for acute asthma. Cochrane Database Syst Rev. 2011;(4):CD001115.
- Stoodley RG, Aaron SD, Dales RE. The role of ipratropium bromide in the emergency management of acute asthma exacerbation: a metaanalysis of randomized clinical trials. Ann Emerg Med. 1999 Jul;34(1):8-18.
- Rodrigo G, Rodrigo C, Burschtin O. A meta-analysis of the effects of ipratropium bromide in adults with acute asthma. Am J Med. 1999 Oct;107(4):363-70.
- Kirkland SW, Vandenberghe C, Voaklander B, et al. Combined inhaled beta-agonist and anticholinergic agents for emergency management in adults with asthma. Cochrane Database Syst Rev. 2017 Jan 11;1(1):CD001284.
- Rowe BH, Spooner C, Ducharme FM, et al. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002178.
- Crossingham I, Turner S, Ramakrishnan S, et al. Combination fixed-dose beta agonist and steroid inhaler as required for adults or children with mild asthma. Cochrane Database Syst Rev. 2021 May 4;5(5):CD013518.
- Kew KM, Kirtchuk L, Michell CI. Intravenous magnesium sulfate for treating adults with acute asthma in the emergency department. Cochrane Database Syst Rev. 2014 May 28;(5):CD010909.
- Goodacre S, Cohen J, Bradburn M, et al; 3Mg Research Team. Intravenous or nebulised magnesium sulphate versus standard therapy for severe acute asthma (3Mg trial). Lancet Respir Med. 2013;1(4):293-300.
- Knightly R, Milan SJ, Hughes R, et al. Inhaled magnesium sulfate in the treatment of acute asthma. Cochrane Database Syst Rev. 2017;11:Cd003898.
- Travers AH, Milan SJ, Jones AP, et al. Addition of intravenous beta(2)-agonists to inhaled beta(2)-agonists for acute asthma. Cochrane Database Syst Rev. 2012 Dec 12;12:CD010179.
- Johnston SL, Szigeti M, Cross M, et al; AZALEA Trial Team. Azithromycin for acute exacerbations of asthma: the AZALEA randomized clinical trial. JAMA Intern Med. 2016;176(11):1630-1637.
- Althoff MD, Holguin F, Yang F, et al. Noninvasive Ventilation Use in Critically Ill Patients with Acute Asthma Exacerbations. Am J Respir Crit Care 2020 Dec 1;202(11):1520-1530.




