
Authors: Nick Hadley, DO (Transition Year Resident, San Antonio, TX) and Jacob Powell, DO (EM Attending Physician, San Antonio, TX) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
Your first patient of the day is a 45-year-old, Caucasian male with complaint of “sinus infection with cough”. Vitals are BP 138/85, HR 93, RR 22, T 99.8F, O2 saturation 93% on 2L. He looks uncomfortable and is working much harder to breathe than someone with a “sinus infection”. Upon questioning, he complains of rhinorrhea, a productive cough with new blood tinged sputum, and worsening shortness of breath and fatigue. History reveals he has been seen in various EDs over the past 2 months. He was treated with multiple antibiotic and steroid courses with progressive worsening of symptoms. He reports that his mother has history of autoimmune disease. He cannot remember the name, but it involved his lungs. On review of systems, he mentions occasional hematuria. You think, “I remember reading about something like this in medical school”.
Background
Granulomatosis with Polyangiitis (GPA, formerly Wegener’s granulomatosis) is a rare vasculitis affecting both arterial and venous small vessels. Incidence is estimated at 12 cases per 1 million individuals per year (1). GPA, along with microscopic polyangiitis and Churg-Strauss syndrome, is a vasculitis associated with antineutrophil cytoplasmic antibodies. GPA, as the name indicates, is characterized by granulomatous formation of lesions in the upper and lower respiratory tract along with glomerular nephritis (1, 2, 4). Onset of disease is usually gradual over the course of 4-12 months (1). The disease affects men and women equally, has a Caucasian predominance, and almost never affects African American males (1). It most commonly occurs in the 4th and 5th decade (1,4), but the disease may occur at any age with 15% of patients diagnosed <19 years of age (4). Prior to development of effective treatment, GPA was universally fatal from a couple months to a year after diagnosis. (1,4). GPA is also associated with a 7% annual risk for venous thromboembolism (6).
Clinical Manifestations
Most common complaints include: fatigue, fever, weight loss, arthralgias, rhinosinusitis, cough, dyspnea, urinary abnormalities (with or without renal insufficiency), purpura, and neurologic dysfunction (2).
Many of these complaints are common and generalized. Due to this, GPA is often not suspected until symptoms are refractory to treatment with antibiotics and/or steroids, or systemic symptoms develop (1). This post will evaluate several organ systems and their common complaints found in this disease.
Eyes
Ocular complaints are less common occurring in 52% of patients (4) compared to pulmonary and renal in 80-90% and 77% of patients, respectively (4). If present, a clinician should at least consider GPA when found in combination with upper/lower airway disease or renal disease. Unilateral proptosis is most common, followed by scleritis, episcleritis, and anterior uveitis (4).

Ear, Nose, Throat
Recurrent sinusitis is a frequent and the most common presenting complaint for GPA (2). In combination with sinusitis, nasal crusting, and persistent rhinorrhea leading to ulceration of nasal mucosa is also commonly found (1). In fact, involvement of the upper airways occurs in 95% of cases (4). Otitis media may be serous in nature, representative of the chronic inflammatory state. The persistent course of inflammation may eventually lead to degradation and destruction of midline facial structures, resulting in saddle nose deformity (2). This is a late finding, however.

Tracheal and Pulmonary
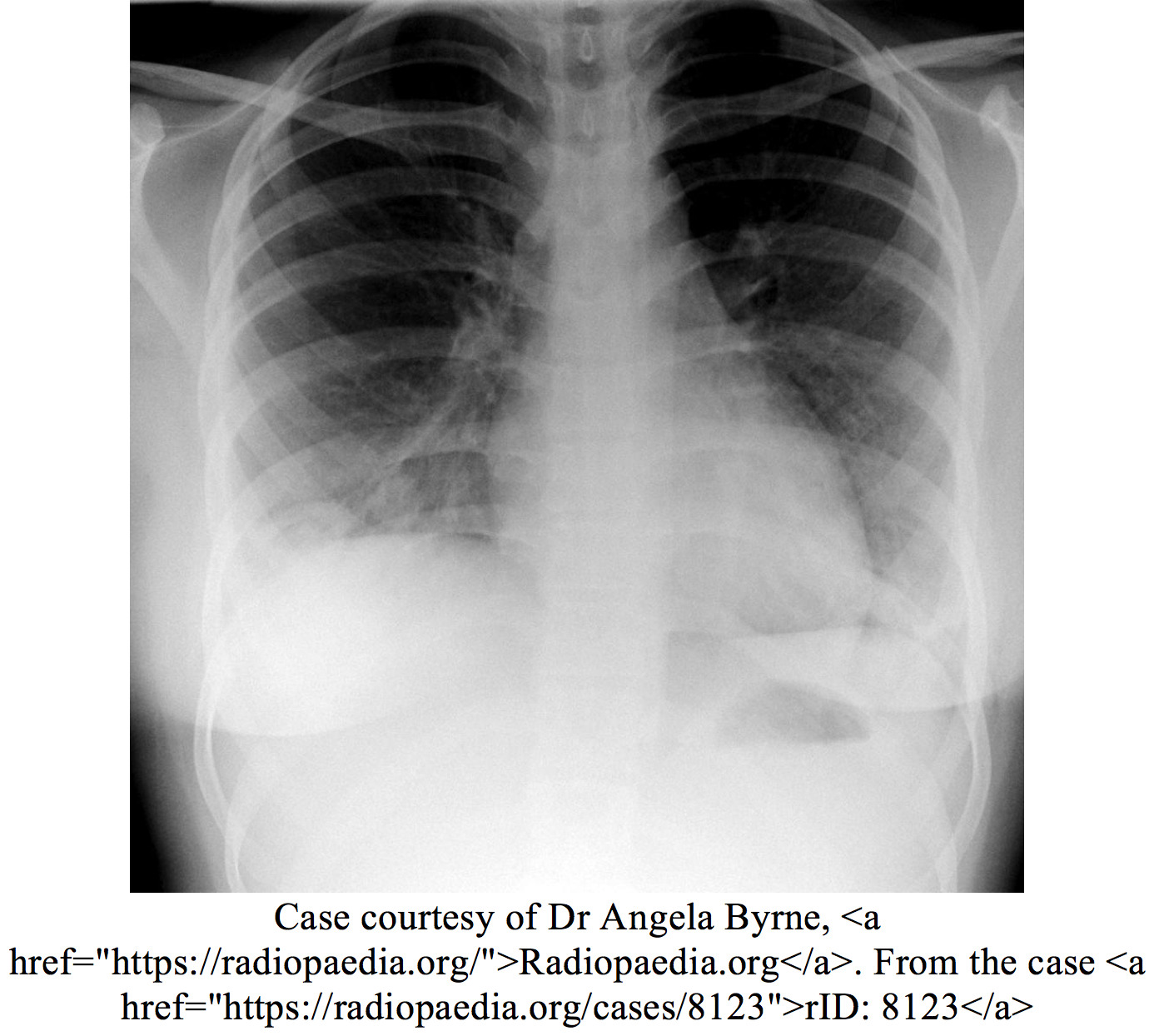
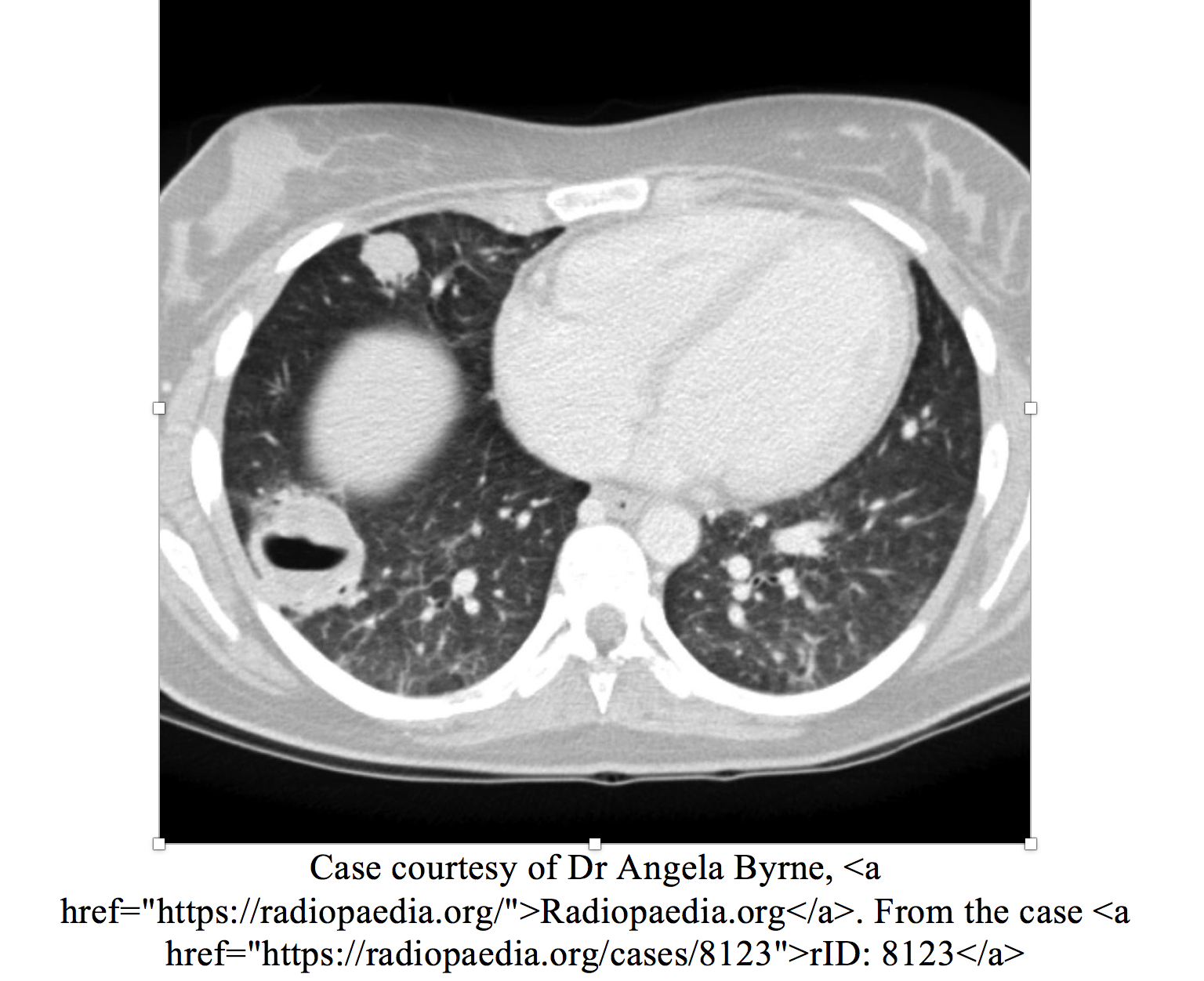
Lungs are initially affected in 40% of cases with cough, dyspnea, and hemoptysis most commonly (1). If not present initially, pulmonary symptoms develop later in 80% of cases (1), with some sources citing up to 85-90% (4). Symptoms of hoarseness, stridor, wheezing, and pleuritic pain also occur less commonly (2). Chest radiographic and CT finding vary but commonly include nodules, patchy of diffuse opacities, and hilar adenopathy (2). On presentation, lung complaints can range from dyspnea to respiratory collapse and the need for intubation.
Renal
Renal involvement develops in 75% of clinical cases but remain subclinical, frequently manifested as symptomatic hematuria until the disease is advanced (1,2). Patient may complain of hematuria that relapses and remits. Urinalysis may display proteinuria in the subnephrotic range (<3 g/day), with hematuria and cell casts (2).
Diagnosis
GPA is not a common disease. The diagnosis is dependent on the clinician keeping it on the differential for refractory pulmonary complaints, especially with renal involvement. Frequently, patients will have a mild anemia, mild leukocytosis, and elevated acute-phase reactants (CRP, ESR, platelets) (2). Unfortunately, these findings do not possess the necessary sensitivity and specificity for diagnosis alone. If there is renal involvement, UA may show proteinuria, hematuria, and cell casts (1). A renal function panel will also show a decreased GFR and increased BUN and creatinine (2). For the pulmonary system, CT is more specific and sensitive than CXR (2). However, CXR will frequently be performed first. Findings on chest radiography are abnormal in two thirds of adults with GPA (5). The most common radiologic findings are single or multiple nodules and masses (5). Nodules are typically diffuse, and approximately 50% are cavitated (5). Definitive diagnosis will not be achieved in the ED, as biopsy is required (2). A presumptive diagnosis may be reached if there is already a positive test for c-ANCA, high suspicion exists based on clinical findings, and a different etiology is not likely (2).
Recommended testing in the ED: CBC, BMP/CMP, ESR/CRP, UA, CXR or CT thoracic.
Do not forget, previous GPA diagnosis is associated with 7% annual risk for VTE. Keep this in mind in patients with history of GPA (6). This occurs because GPA affects veins in addition to arteries (1), and the chronic inflammatory state results in hypercoagulability. Your patient’s SOB may be due to a pulmonary embolism!
Confirmatory testing after admission (but not in ED) includes ANCA, PR3 or c-ANCA (positive in 90%), MPO or p-ANCA, and pulmonary or renal biopsy.
Treatment
Treatment in the ED is supportive, while monitoring and managing the airway and pulmonary system as needed. This may range from O2 via nasal cannula to intubation for acute respiratory distress. This is very important to keep in mind as the necrotizing granulomas of the upper and lower respiratory tract may quickly (days to weeks) lead to respiratory failure, which may be during the patient stay in your ED, (or shortly after if discharged) depending on where the patient is in the progression of the disease. If a high clinical suspicion is present, treatment with prednisone 1 mg/kg can be initiated.
After admission, there are 2 treatment options for achieving remission (1):
Prednisone 1 mg/kg/day with cyclophosphamide 2 mg/kg/day for 3-6 months
Or
Prednisone 1 mg/kg/day with rituximab 375 mg IV/week
Cyclophosphamide (in addition to prednisone) treatment leads to symptom improvement in >90% of patients, complete remission in 75% of patients, and a 5 year survival of over 80% (4).
Despite the ability to successfully induce remission, 50–70% of remissions are later associated with one or more relapses (4). This is important to keep in mind that those with previous GPA frequently have relapses.
Case Conclusion
The patient was mildly anemic with leukocytosis of 13.2. His C-reactive protein was 45 mg/L, ESR 63 mm/hr, and CXR demonstrated perihilar nodules. He is admitted and started on prednisone 1 mg/kg PO daily. Over the course of 24 hours, his oxygen demand increases to the point he is electively intubated and transferred to the ICU. A few days later his ANCA result is positive for c-ANCA. He is begun on cyclophosphamide 2 mg/kg/day IV and extubated 2 days later. Through the continued treatment with prednisone and cyclophosphamide, he left the hospital 4 days later and achieved remission 6 months later.
Summary
- Granulomatosis with polyangiitis is classically a triad of:
- Upper respiratory symptoms
- Lower respiratory symptoms
- Renal involvement
- Complaints are commonly non-specific so look for refractory upper and lower respiratory symptoms with or without renal involvement
- Most common in 4th and 5th decade but can occur at any age
- Respiratory collapse can occur quickly
- GPA associated with 7% annual risk for VTE
- Previous GPA frequently have relapses
References/Further Reading
1. Hellmann DB, Imboden Jr. JB. Rheumatologic, Immunologic, & Allergic Disorders. In: Papadakis MA, McPhee SJ, Rabow MW. eds. Current Medical Diagnosis & Treatment 2017 New York, NY: McGraw-Hill; http://accessmedicine.mhmedical.com/content.aspx?bookid=1843§ionid=135713619. Accessed August 11, 2017.
2. FALK RJ, Merkel PA, KING TE. Clinical manifestations and diagnosis of granulomatosis with polyangiitis and microscopic polyangiitis. UpToDate. http://www.uptodate.com/home. Published November 15, 2016. Accessed August 11, 2017.
3. Sims T. Hemoptysis. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds.Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016; http://accessmedicine.mhmedical.com/content.aspx?bookid=1658§ionid=109439227.Accessed August 11, 2017.
4. Langford CA, Fauci AS. The Vasculitis Syndromes. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J. eds.Harrison’s Principles of Internal Medicine, 19e New York, NY: McGraw-Hill; 2014. http://accessmedicine.mhmedical.com/content.aspx?bookid=1130§ionid=79750480.Accessed August 11, 2017.
5. Tracy, Christopher L, and Herbert S Diamond. “Granulomatosis with Polyangiitis (Wegener Granulomatosis) Workup.” Granulomatosis with Polyangiitis (Wegener Granulomatosis) Workup: Approach Considerations, ANCA Detection, Radiography and CT Scanning, 9 Dec. 2016, emedicine.medscape.com/article/332622-workup#c8. Accessed 2 Sept. 2017.
6. Granulomatosis with polyangiitis. (n.d.). Retrieved September 02, 2017, from http://www.dynamed.com.proxy.rvu.edu/topics/dmp~AN~T115969/Granulomatosis-with-polyangiitis#Complications-and-Prognosis
Disclaimer: The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Air Force, the Department of the Army or the Department of Defense or the U.S. Government.




