Authors: Michael Andrew Tandlich, MD (EM Resident Physician, Northwestern University) and Timothy M. Loftus, MD, MBA (EM Attending Physician, Northwestern University) // Edited by: Bryant Allen, MD (EM Attending Physician, Carolinas Medical Center): Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case 1:
An 87-year-old male with history significant for chronic obstructive pulmonary disease, myelodysplastic syndrome complicated by anemia of chronic disease, obstructive sleep apnea, coronary artery bypass grafting, and percutaneous coronary interventions for coronary artery disease, with over a one-year history of exertional dyspnea, presented to the ED with one to two weeks of worsening dyspnea on exertion. Patient states he would feel his dyspnea worsen with any movement. In the ED, his vital signs were stable, and there was no hypoxia at rest, but upon standing upright, he was noted to have an abrupt oxygen desaturation on a pulse oximeter to 86% on room air. Laboratory studies were remarkable for a hemoglobin level of 8.2 g/dL, down from 9.6 g/dL two weeks prior. Chest x-ray and ECG showed no acute processes. The patient was transfused one unit of packed red blood cells and admitted to the hospital medicine floor for further management.
Case 2:
A 2-year-old female previously healthy with up-to-date immunizations presents to the ED with two days of lethargy, fever, rhinorrhea, and difficulty breathing. On exam, the patient appeared normal color with no increased work of breathing. Vitals notable for HR 137, RR 23, T 37.8, SpO2 65% on room air, improved to 78% on 15L NRB. Exam was notable for normal breath sounds and respiratory effort, normal heart sounds without auscultated murmurs, and an otherwise normal exam. An arterial blood gas was performed, demonstrating a true oxygen saturation of 96 percent.
What is hypoxia?
Hypoxia is the condition when body tissues receive inadequate oxygen. This leads to disruption in cellular function. There may be a switch to anaerobic metabolism and subsequent lactic acidosis. While low blood oxygen content, also known as hypoxemia, is a major cause of hypoxia, it is not the only cause.
What are the major etiologies of hypoxia?
Hypoxia can best be broken down into four major categories:
- Hypoxemia
- Anemic Hypoxia
- Ischemic/Stagnant Hypoxia
- Histotoxic Hypoxia
Hypoxemia
Hypoxia which refers to the state of low oxygen concentration in the blood itself, and largely depends on five key factors:
- Altitude: As one moves to higher altitudes, the barometric pressure drops, resulting in the amount of oxygen content inspired to be decreased despite a stable FiO2. At the extremes of altitude, an otherwise healthy lung would not see enough oxygen in the inspired air to adequately supply metabolism of the body tissues.
- Ventilation: Ventilation refers to the supply of gases to the alveoli and is directly tied to clearance of CO2. Hypoventilation leads to CO2buildup, decreased CO2 clearance, and subsequent decreased concentration of alveolar oxygen. In many disease processes, an increase in CO2 itself may drive increased work of breathing and is correlated with lung compliance and airway resistance. For example, a patient with acute asthma exacerbation will have high airway resistance which will exacerbate work of breathing.
- Oxygen Diffusion: This is the ability of oxygen to cross the alveoli and surround capillary membranes effectively. Transport may be impaired because of a primary tissue disease process, such as in pulmonary fibrosis.
- Ventilation/Perfusion (V/Q) Matching: There is a balance between oxygenation of alveoli and blood flow through their capillaries. Mismatch between these two factors will occur when blood flows through alveoli with inadequate ventilation, or when blood does not reach alveoli that do have adequate ventilation. Examples of this is include pulmonary embolism, in which perfusion is obstructed, and status asthmaticus, in which airway collapse causes air trapping and ventilation obstruction. Mismatch may be corrected when excess oxygen is inhaled, since even poorly ventilated areas of the lung will receive adequate flow of oxygen. It is important to note that ventilation and perfusion matching is heterogeneous throughout different areas of the lung in normal state and is exacerbated by certain conditions affecting V/Q mismatch (e.g. asthma, pneumonia).
- Blood Shunting: Shunting of blood refers to the bypassing of the process by which blood receives oxygenation. In other words, blood enters systemic circulation before receiving adequate oxygenation. Classic examples of blood shunting occur with anatomic defects such as intracardiac septal defects. Mucus plugging of one mainstem bronchus is another example of shunt physiology. In either case, an increase fraction of inspired oxygen will not fill alveoli which are receiving blood, and classically will not correct hypoxemia.
Anemic hypoxia
Hypoxia may occur if there is a critically low blood oxygen carrying capacity. Acute changes in hemoglobin level (such as from acute blood loss anemia and hypovolemic shock) may result in decreased transport of oxygen to tissues. Hypoxia may also result from changes in the hemoglobin functionality such as during acute carbon monoxide poisoning, where there are plenty of hemoglobin molecules which simply are not able to bind oxygen.
Ischemic/stagnant hypoxia
Hypoxia may result from a critical decrease in the flow of oxygenated blood to peripheral tissues. Systemic conditions such as cardiogenic shock may lead to decrease oxygenation of blood during pulmonary gas exchange as well as inadequate global delivery of blood to central and peripheral organs. Localized conditions may impede cellular diffusion of oxygen (such as with severe tissue edema) or focally impede flow of oxygenated blood (such as with arterial damage or obstruction).
Histotoxic hypoxia
Hypoxia may result from low tissue utilization of oxygen. This may occur with direct cellular poison (cyanide, colchicine overdose) or abnormally high tissue oxygen demand (malignancy).
When should hypoxia be suspected?
While there is no single lab value to directly measure hypoxia, it should be suspected in any patient with anxiety, confusion, and restlessness, which may be early signs of hypoxia and may precede changes in vital signs3. Low SpO2 is the hallmark of hypoxemia, one of the main causes of hypoxia, and may be suspected in any patient with oxygen saturation less than 90 percent (or less than 88 percent in patients with chronic lung disease). Lactic acidosis may develop in response to anaerobic metabolism from tissue hypoxia or from increased catecholamine surge and may be detected on blood gas4.
Approach to Hypoxia
1-Patient Stability – check general appearance, ABCs, vital signs
In the assessment of any patient in the ED, it is the cornerstone of our decision making as EM physicians to do a quick yet thorough “sick or not sick” assessment.
General appearance
How does the patient appear? Is the patient comfortable or in acute distress? Does the patient exhibit any behaviors which may be clinical signs however subtle of “badness?”
ABCs
Airway, Breathing, and Circulation assessment is the right place to start in any patient who may be experiencing critical illness, including from hypoxia.
Is the patient protecting her airway? Although rare, hypoxia may result from critical airway narrowing that can be audibly detected as stridor. In pediatric patients, laryngeal stridor should prompt a thorough evaluation of upper airway obstruction5. Hypoxia may be seen with severe smoke inhalation injury, which may present with rales and rhonchi and lead to imminent airway compromise6.
Are breath sounds present bilaterally? While tension pneumothorax is associated with classic symptoms of respiratory distress and tracheal deviation, only half of cases may present with frank hypoxia7. Does the chest rise and fall equally? Patients with significant rib fractures causing an unstable chest wall may become inadequately ventilated and develop hypoxia as well as hypercapnia and acidosis8.
Is the patient tachycardic? Are distal pulses present? Thready pulses may indicate intravascular volume loss. In the patient with blunt trauma, this may be a manifestation of hemorrhagic shock, in whom resuscitation is vital to prevent tissue hypoxia9. In the patient with severe infection, tachycardia may be the manifestation of inflammatory-mediated fluid shifts and subsequent end-organ hypoperfusion and ischemic damage10.
Vital Signs
Especially in any unstable patient, it is crucial to obtain a full set of vitals, which are likely to be abnormal and may help to elucidate an underlying etiology of the patient’s instability. Acute hypoxia is most likely to manifest with increased respiratory rate (RR>24) and increased heart rate (HR>100), but normal respiratory rate and heart rate should not exclude the possibility of hypoxia10. In diseases with hypoxemia and hypercarbia, the body will try to increase tidal volume in addition to respiratory rate, with the goal of increasing alveolar ventilation11. Patients with brisk intravascular volume loss may develop tachycardia and hypotension, and as the hypovolemia worsens, the body compensates for the subsequent tissue hypoxia by increasing respiratory rate12. Patients with hypotension may have hypoxia from malperfusion and warrants a prompt investigation of the underlying cause. Patients hypoxic from septic shock may be hyperthermic or hypothermic, and this may best be identified using core temperature measures such as rectal temperature. Pulse oximetry reading is prone to inaccuracies, especially in the unstable patient, and it should always be considered in a clinical context.
2-History and Physical Exam
In the unstable patient, the history may be limited. Yet, in the stable patient it is important to obtain a thorough history and physical exam. Taking a clear and thorough history is the first important step.
Does the patient have a history of cardiac disease or pulmonary disease? Patients with preexisting cardiovascular disease are more likely to develop dysfunctional perfusion of end organs and a subsequent hypoxic state13. Patients with underlying lung disease are prone to developing physiologic changes that increase the risk of hypoxemia and subsequent hypoxia, including decreased ventilatory drive, airway obstructive processes, intra-alveolar exudates, alveolar septal thickening, inflammation and fibrosis, and alveolar capillary damage14.
Any history of smoking? Cigarette smoking is well known for its detrimental effects on normal body physiology and is associated with increased risk of hypoxia. Carbon monoxide blood levels are often elevated in chronic smokers in whom severe elevations and symptoms of hypoxia have been reported.15
Recent surgeries? Patients in the post-operative period are generally more prone to atelectasis, pneumonia, and pulmonary embolism, all pathologies that may present with hypoxia16.
Review of Systems: Many patients with hypoxia will report dyspnea or increased work of breathing. Patients may also note confusion or feeling sluggish. Headache may the only symptom of hypoxia in patients with acute CO poisoning17.
Physical Exam
General appearance of a patient may give clues to underlying etiology. Cyanosis may first show on lips and distal fingertips and may be a sign of severe hypoxemia. Diffuse, dull, red skin discoloration may be a sign of cyanide toxicity. Pale appearance may be a sign of acute blood loss anemia. Crackles on auscultation of lung parenchyma may point to heart failure if bilateral or a lobar pneumonia if focal and unilateral. Absent breath sounds may point to an effusion or a collapsed lung. Distal extremities may be warm in distributive shock or cold and clammy in a patient with hemorrhage. Cherry red skin and mucous membranes are usual post-mortem findings in carbon monoxide poisoning which are in fact uncommon at presentation18. Patient may be altered and restless on neurologic exam. Rectal exam with gross blood may point to acute blood loss anemia.
3-Further Evaluation
Arterial oxygen saturation (SaO2)
SaO2 describes the amount of oxygen bound to hemoglobin, and normal values range between 95 and 100 percent19. A rapid means of evaluating this is with pulse oximetry. Based on the known absorption of light at particular wavelengths of oxygenated and deoxygenated blood, pulse oximetry uses spectrophotometry to calculate an estimated SaO2 (SpO2)20. The accuracy of this measurement relies in part on accurate signal strength, which is demonstrated as a waveform and which should normally be sharp with a clear, dicrotic notch20. Low perfusion states will have sinus wave forms with low amplitude; SpO2 measurements must be taken with caution in these patients (such as those with low cardiac output, peripheral vasoconstriction, or hypothermia)20. SpO2readings should also be taken with caution in patients with nail polish, which may interfere significantly with light absorption at the wavelengths used by pulse oximetry, as well as in patients with darker skin pigmentation21,22. It is also important to note that SpO2 is often inaccurate in patients with carbon monoxide poisoning23. In fact, since oxyhemoglobin and carboxyhemoglobin have similar absorptive properties for red light, pulse oximetry will often estimate true SaO2 as normal or falsely elevated in patients with CO poisoning; this absorptive property is also the reason patients with CO poisoning would appear cherry red24. Methemoglobinemia is another disease in which its absorptive properties of red light will make pulse oximetry unreliable and is the reason significant toxicity will often shift pulse oximetry estimations of SaO2 toward approximately 85 percent24. Also be cautious when using pulse oximetry to trend oxygen saturation in critically ill patients, in whom the effects of acidosis and amenia have been shown to interfere with the correlation of pulse ox estimates and true SaO225. New, multi-wavelength pulse oximeters designed to measure methemoglobin and carboxyhemoglobin may improve future oxygen monitoring capabilities26.
Arterial Blood Gas (ABG)
Blood gas analysis provides information on alveolar ventilation, oxygenation, and acid-base balance27. In the evaluation of these key physiologic processes, ABG analysis measures arterial partial pressure of oxygen (PaO2) and carbon dioxide (PaCO2), and compared with pulse oximetry, it is a more definitive tool in evaluating oxygenation and ventilation28,29. Normal PaO2is considered 80-100 mmHg, and lower values may indicate hypoxemia as the cause of hypoxia. Knowledge of its value also is useful in managing patients on ventilatory support30. Normal PaCO2 is considered 35-45 mmHg, and its levels may be elevated in either situations of increased metabolism or decreased ventilation; in either case, acuity of the hypercapnia can be evaluated by assessing for any concurrent change in HCO330. Elevations from baseline of PaCO2 in respiratory distress with increased work of breathing may signal respiratory failure and serve as an indication for ventilatory support31. While most ABG analyses measures pH and PaCO2 directly, HCO3 and base changes are indirectly calculated; especially in critically ill patients, these latter calculations may be highly variable and should be interpreted with caution32. This prompt direct measurement of pH may be critical in patients with metabolic derangements, such as in severe sepsis, diabetic and alcoholic ketoacidosis, trauma, acute respiratory failure, cardiac arrest, and COPD; in these situations, venous blood gas (VBG) analysis, one which may be clinically preferred for numerous reasons, is also reliable33.
It is imperative to always interpret ABG within the clinical context of the patient. Accuracy of the data collected with an ABG sample is particularly susceptible to errors, and care must be taken to confirm the blood sample is truly arterial in nature (and not venous), completely and promptly rid of any air bubbles, inspected for any clots, and analyzed within thirty minutes of the collection time34. ABG samples are even more prone to error in patients with high PaO2 such as those with high levels of supplemental oxygen or in whom shunt physiology is suspected, as well patients with leukocytosis or thrombocytosis, and should have ABG analysis performed within five minutes34.
Venous Blood Gas (VBG)
Compared with ABG, the VBG puncture is often quicker to perform, less painful, and carries a lower risk of complications such as arterial injury and arterial thrombosis35,36. Given these potential benefits, VBG should be considered in establishing acid-base state and assessing respiratory function, two key purposes for which blood gas analysis is used in the ED. VBG is noninferior in its ability to screen for acid-base abnormalities in critical illnesses such as DKA and acute COPD exacerbations34,35. Numerous studies and meta-analyses have confirmed this35,37,38. Caution should be taken in severe hemodynamic compromise such as in severe shock or cardiac arrest, when VBG analysis of lactate and pH has been shown to be less reliable38,39. Furthermore, while VBG may be helpful in screening for arterial hypercarbia, it has poor correlation with ABG results in pO2 and pCO2 analysis and is too clinically unpredictable39.
Imaging
Imaging studies of the chest can aid in determining the underlying cause of hypoxia. Chest x-ray can be useful in diagnosing focal airway abnormalities, such as pneumonia, acute respiratory distress syndrome, lung hyperinflation, and pulmonary edema. An initial chest x-ray may not always elucidate an underlying etiology. Chest computed tomography (CT) can be useful in giving more detail. Evidence of smoke inhalation injury may be absence on initial chest x ray imaging but nonetheless will serve as a baseline evaluation in such cases40.
Differential Diagnosis of Hypoxia
HYPOXEMIC:
– High altitude: high altitude, high altitude pulmonary edema
– Hypoventilation: central nervous system depressants (opioids), hypothyroidism, neuromuscular (myasthenia gravis, Guillain-Barre syndrome), nerve disease (cervical spine injuries, phrenic nerve injuries), chest wall injury (flail chest)
– Low Diffusion: pulmonary edema, pulmonary contusion, chronic obstructive pulmonary disease, interstitial lung disease
– V/Q Mismatch: pulmonary embolism, chronic obstructive pulmonary disease, asthma, mucus plugging, pulmonary hypertension
– Shunt: Intracardiac, arteriovenous malformation, pneumonia, atelectasis, acute respiratory distress syndrome
ANEMIC:
acute blood loss anemia, hemorrhagic shock, carbon monoxide poisoning, methemoglobinemia
ISCHEMIC:
global: cardiogenic shock (STEMI, ADHF), distributive shock (anaphylaxis, severe sepsis), obstructive shock (tamponade, tension pneumothorax), increased demand (seizure, shivering)
local: arterial obstruction, interstitial edema
HISTOTOXIC:
cyanide poisoning, hydrogen sulfide
4-Management
Maintain Patent Airway
The first step in managing an airway is to evaluate whether the airway is patent. Hypoxic patients with respiratory failure or altered consciousness may not be able to protect their airway patency in which endotracheal intubation may be warranted41. Patients in respiratory failure exhibiting signs of fatigue (such as lethargy, increasing use of accessory muscles, decreased rate and depth of respiration) may decompensate without ventilatory support in whom intubation may also be warranted42. Airway management is particularly important in inhalation injuries and thorough evaluation and risk stratification for impending airway compromise may be performed with fiberoptic bronchoscopy43.
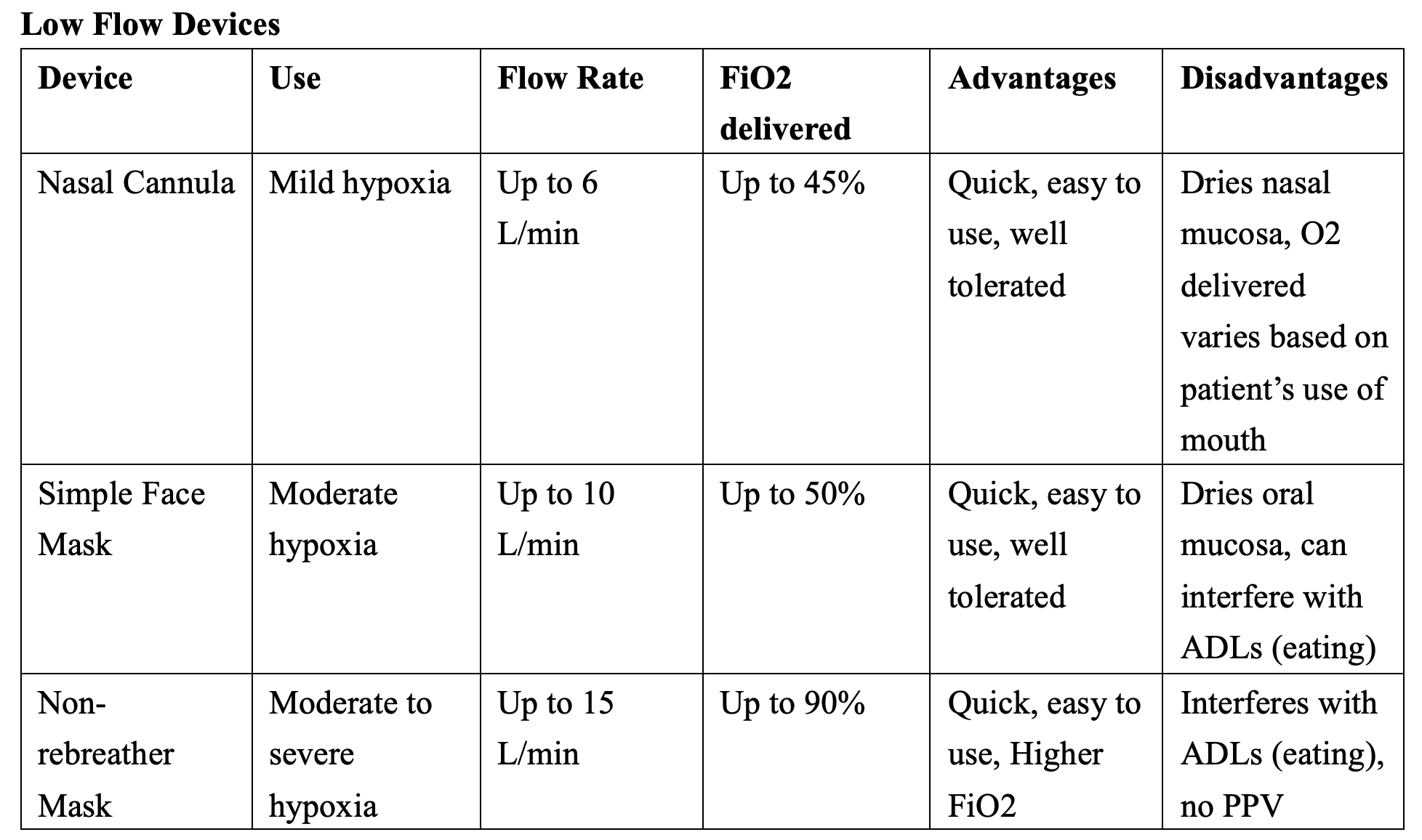
Increase Oxygen Content of Inspired Air
Supplemental oxygen is the cornerstone of therapy for many cases of hypoxia and can be divided into devices which provided low flow of oxygen, high flow of oxygen, and positive pressure ventilation. Supplemental oxygen at 100% FiO2 should be administered to any patient with suspected inhalation injury in whom the physiologic goal is to quickly reverse and displace carbon monoxide from hemoglobin binding sites44.

Positive Pressure Ventilation
Noninvasive positive-pressure ventilation has well-studied indications for exacerbations of COPD, acute asthma exacerbations, acute cardiogenic pulmonary edema, weaning off mechanical ventilation, respiratory failure, and prevention of its worsening, and in patients with an order for Do Not Intubate45. In these cases, the positive ventilatory pressure functions physiologically to augment cardiac output, improve oxygen delivery, improve respiratory mechanics, and reduce the effort of breathing46. Endotracheal intubation should be considered in cases when noninvasive ventilation is contraindicated, such as in patients with altered mental status, vomiting, copious secretions, inability to protect their airway, upper airway obstruction45.

Improve Diffusion Capacity
In acute cases of hypoxia from underlying lung pathology, the overarching goal is to treat the underlying cause, which in some cases may involve improving oxygen diffusion across the alveolar-capillary membranes. Diuretics and pulmonary vasodilators can be considered in cases of pulmonary edema, and steroids can be considered in cases of interstitial lung disease. Extracorporeal Membrane Oxygenation (ECMO) is the most invasive means of increasing diffusion capacity of oxygen and its use is indicated in a subset of refractory cases of hypoxia47.
Adjunctive therapies
Acute cases of hypoxia ultimately require treatment of the underlying cause. Altitude sickness may require treatment with steroids and hyperbaric oxygen48. Patients with severe hypoxia from ARDS may be placed in prone positioning to improve V/Q mismatch, improve oxygenation and decrease mortality49.The mainstay of therapy for cases of severe septic shock may include fluids, antibiotics, and blood pressure augmenting medications. Patients with acute gastrointestinal blood loss and hemodynamic changes may require blood transfusion, particularly when hemoglobin levels reach 7 to 8 g/dL50. In addition to oxygenation and ventilation assistance, patients with hypoxia from cardiogenic shock may need aggressive fluid management, vasopressor support, or mechanical circulatory support device placement51. Hypoxia from arterial ischemia and obstruction may require surgical consultation for percutaneous intravascular therapy52. Hydroxocobalamin, a precursor to vitamin b-12, should be considered a first-line agent in the patient with suspected cyanide toxicity in whom the treatment binds to toxic cyanide and forms a stable compound excreted in the urine53.
Case Studies
Case 1: This patient had platypnea-orthodexia syndrome (POS), a disease characterized by positional dyspnea (platypnea) and hypoxemia in the setting of being in the upright position (orthodexia). As opposed to orthopnea, it is relieved by lying flat. His underlying cause was shunting of blood through a patent foramen ovale (PFO), which is the most common cause of POS. Generally, POS presents in an elderly patient with underlying cardiac anatomic defects who later in life has developed new secondary anatomic or functional abnormalities which lead to clinically significant shunt physiology and subsequent hypoxemia54. This case highlights the need for maintaining a high level of suspicion in cases which remain refractory to standard treatment.
Case 2: This patient had congenital methemoglobinemia, which was not apparent at birth due to hemoglobin switching phenomenon. Otherwise healthy individuals have a small amount of methemoglobin in the body; this disease is characterized by a deficiency in cytochrome b5 reductase (b5R), disrupting the biochemical pathway responsible for reducing methemoglobin back to normal hemoglobin in the blood. The patient on further history was noted to have a father with a similar disease. Methemoglobinemia should be suspected in any patient with cyanosis and abnormal SpO2 that does not respond to supplemental oxygen. It is not always detected by pulse oximetry and requires ABG analysis, which demonstrated a methemoglobin concentration of 10.6 percent in this patient. Formal diagnosis is made with DNA sequencing. The primary treatment of methemoglobinemia is methylene blue and should be given 1-2 mg/kg IV.
Pearls & Pitfalls
– Hypoxia is inadequate oxygen delivery to tissue, and hypoxemia is only one of the many causes.
– In any patient with hypoxia who appears generally unstable, it is important to assess the patient’s ABCs and vital signs.
– There are many pitfalls to using pulse oximetry, and blood gas analysis is a more definitive tool in the evaluation and management of a patient’s hypoxia.
– While there is a range of therapies to support and improve a patient’s oxygenation and ventilation, it is important to thoroughly investigate and treat the underlying cause in any patient with acute hypoxia.
– Consider a broad differential diagnosis in cases of hypoxia which remain refractory to standard treatment.
References
[1] Mirwais S, Mirwais M, Altaf A, Collins J. Patent Foramen Ovale With Platypnea – Orthodeoxia Syndrome: A Case Report. Cureus. 2020;12(10):e10958. Published 2020 Oct 15. doi:10.7759/cureus.10958.
[2] Hodges S, Carter T. Curious case of unexplained hypoxia. J Paediatr Child Health. 2020 Mar;56(3):478-479. doi: 10.1111/jpc.14620. Epub 2019 Sep 3. PMID: 31482607 https://onlinelibrary-wiley-com.ezproxy.galter.northwestern.edu/doi/epdf/10.1111/jpc.14620.
[3] Jardins, T., & Burton, G. G. (2011). Clinical manifestations and assessment of respiratory diseases (6th ed.). St Louis; MO: Elsevier-Mosby.
[4] Shannon TM, Celli B. Oxygen therapy. Emerg Med 1991;23(21): 63-70.
[5] Adamczuk D, Krzemień G, Szmigielska A, Pierzchlewicz A, Roszkowska-Blaim M, Biejat A, Dębska M, Jabłońska-Jesionowska M. Wrodzony stridor krtaniowy– problem interdisciplinary [Congenital laryngeal stridor – an interdisciplinary problem]. Med WiekuRozwoj. 2013 Apr-Jun;17(2):174-8. Polish. PMID: 23988376.
[6] Mlcak RP, Suman OE, Herndon DN. Respiratory management of inhalation injury. Burns. 2007;33(1):2–13.
[7] Roberts DJ, Leigh-Smith S, Faris PD, Blackmore C, Ball CG, Robertson HL, Dixon E, James MT, Kirkpatrick AW, Kortbeek JB, Stelfox HT. Clinical Presentation of Patients With Tension Pneumothorax: A Systematic Review. Ann Surg. 2015 Jun;261(6):1068-78. doi: 10.1097/SLA.0000000000001073. PMID: 25563887.
[8] Reška M, Čapov I, Peštál A, Konečný J, Chovanec Z, Prudius V, Benej M, Páral M, Veverková L. Naše zkušenosti se stabilizacíhrudníku [Our experience with chest wall stabilization]. Rozhl Chir. 2017 Fall;96(11):469-474. Czech. PMID: 29318889.
[9] Gutierrez G, Reines HD, Wulf-Gutierrez ME. Clinical review: hemorrhagic shock. Crit Care. 2004 Oct;8(5):373-81. doi: 10.1186/cc2851. Epub 2004 Apr 2. PMID: 15469601; PMCID: PMC1065003.
[10] Samuel J., Franklin C. (2008) Hypoxemia and Hypoxia. In: Myers J.A., Millikan K.W., Saclarides T.J. (eds) Common Surgical Diseases. Springer, New York, NY. https://doi.org/10.1007/978-0-387-75246-4_97.
[11] Steichen O, Grateau G, Bouvard E. Respiratory rate: the neglected vital sign. Med J Aust. 2008 Nov 3;189(9):531-2. doi: 10.5694/j.1326-5377.2008.tb02164.x. PMID: 19051386.
[12] Lelubre C, Vincent JL. Mechanisms and treatment of organ failure in sepsis. Nat Rev Nephrol. 2018 Jul;14(7):417-427. doi: 10.1038/s41581-018-0005-7. PMID: 29691495.
[13] Lucero García Rojas EY, Villanueva C, Bond RA. Hypoxia Inducible Factors as Central Players in the Pathogenesis and Pathophysiology of Cardiovascular Diseases. Front Cardiovasc Med. 2021 Aug 10;8:709509. doi: 10.3389/fcvm.2021.709509. PMID: 34447792; PMCID: PMC8382733.
[14] Tuder RM, Yun JH, Bhunia A, Fijalkowska I. Hypoxia and chronic lung disease. J Mol Med (Berl). 2007 Dec;85(12):1317-24. doi: 10.1007/s00109-007-0280-4. Epub 2007 Nov 27. PMID: 18040654.
[15] Dorey A, Scheerlinck P, Nguyen H, Albertson T. Acute and Chronic Carbon Monoxide Toxicity from Tobacco Smoking. Mil Med. 2020 Feb 12;185(1-2):e61-e67. doi: 10.1093/milmed/usz280. PMID: 31670370.
[16] Sellery GR. A review of the causes of postoperative hypoxia. Can Anaesth Soc J. 1968 Mar;15(2):142-51. doi: 10.1007/BF03005721. PMID: 4874784.
[17] Kealey GP. Carbon monoxide toxicity. J Burn Care Res. 2009 Jan-Feb;30(1):146-7. doi: 10.1097/BCR.0b013e3181923b81. PMID: 19060737.
[18] Hanley ME, Patel PH. Carbon Monoxide Toxicity. [Updated 2021 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430740/
[19] Zuzana Kovacsova, Gemma Bale, Ilias Tachtsidis, Medical Utility of NIR Monitoring, Editor(s): Roger Narayan, Encyclopedia of Biomedical Engineering, Elsevier, 2019, Pages 415-431, ISBN 9780128051443, https://doi.org/10.1016/B978-0-12-801238-3.64141-7.
[20] Jubran A. Pulse oximetry. Crit Care. 2015 Jul 16;19(1):272. doi: 10.1186/s13054-015-0984-8. PMID: 26179876; PMCID: PMC4504215.
[21] Coté CJ, Goldstein EA, Fuchsman WH, Hoaglin DC. The effect of nail polish on pulse oximetry. Anesth Analg. 1988 Jul;67(7):683-6. PMID: 3382042.
[22] Hinkelbein J, Genzwuerker HV, Sogl R, Fiedler F. Effect of nail polish on oxygen saturation determined by pulse oximetry in critically ill patients. Resuscitation. 2007 Jan;72(1):82-91. doi: 10.1016/j.resuscitation.2006.06.024. Epub 2006 Nov 13. PMID: 17098347.
[23] Buckley RG, Aks SE, Eshom JL, Rydman R, Schaider J, Shayne P. The pulse oximetry gap in carbon monoxide intoxication. Ann Emerg Med. 1994 Aug;24(2):252-5. doi: 10.1016/s0196-0644(94)70137-7. PMID: 8037391.
[24] Chan ED, Chan MM, Chan MM. Pulse oximetry: understanding its basic principles facilitates appreciation of its limitations. Respir Med. 2013 Jun;107(6):789-99. doi: 10.1016/j.rmed.2013.02.004. Epub 2013 Mar 13. PMID: 23490227.
[25] Perkins GD, McAuley DF, Giles S, Routledge H, Gao F. Do changes in pulse oximeter oxygen saturation predict equivalent changes in arterial oxygen saturation? Crit Care. 2003 Aug;7(4):R67. doi: 10.1186/cc2339. Epub 2003 Jun 11. PMID: 12930558; PMCID: PMC270702.
[26] Barker SJ, Curry J, Redford D, Morgan S. Measurement of carboxyhemoglobin and methemoglobin by pulse oximetry: a human volunteer study. Anesthesiology. 2006 Nov;105(5):892-7. doi: 10.1097/00000542-200611000-00008. Erratum in: Anesthesiology. 2007 Nov;107(5):863. PMID: 17065881.
[27] Thurnheer R. Stolpersteine bei der Beurteilung der arteriellen Blutgase [Fallacies in arterial blood gas interpretation]. Ther Umsch. 2013 Aug;70(8):473-9. German. doi: 10.1024/0040-5930/a000434. PMID: 23876754.
[28] Castro D, Patil SM, Keenaghan M. Arterial Blood Gas. 2021 Jul 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearlsPublishing; 2021 Jan–. PMID: 30725604.
[29] Al Ashry HS, Richards JB, Fisher DF, Sankoff J, Seigel TA, Angotti LB, Wilcox SR. Emergency Department Blood Gas Utilization and Changes in Ventilator Settings. Respir Care. 2018 Jan;63(1):36-42. doi: 10.4187/respcare.05590. Epub 2017 Sep 26. PMID: 28951466.
[30] Rawat D, Modi P, Sharma S. Hypercapnea. 2021 Jul 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID: 29763188.
[31] Mountain RD, Sahn SA. Clinical features and outcome in patients with acute asthma presenting with hypercapnia. Am Rev Respir Dis. 1988 Sep;138(3):535-9.
[32] Kim Y, Massie L, Murata GH, Tzamaloukas AH. Discrepancy between Measured Serum Total Carbon Dioxide Content and Bicarbonate Concentration Calculated from Arterial Blood Gases. Cureus. 2015 Dec 07;7(12):e398.
[33] White HD, Vazquez-Sandoval A, Quiroga PF, Song J, Jones SF, Arroliga AC. Utility of venous blood gases in severe sepsis and septic shock. Proc (Bayl Univ Med Cent). 2018 May 9;31(3):269-275. doi: 10.1080/08998280.2018.1460133. PMID: 29904286; PMCID: PMC5997042.
[34] Sood P, Paul G, Puri S. Interpretation of arterial blood gas. Indian J Crit Care Med. 2010 Apr;14(2):57-64. doi: 10.4103/0972-5229.68215. PMID: 20859488; PMCID: PMC2936733.
[35] van Exsel JA, Simons SO, Kramers C, Heijdra YF. Wanneer volstaat een veneuze bloedgas op de SEH? [When is a venous blood gas analysis sufficient in the emergency department?]. Ned Tijdschr Geneeskd. 2017;161:D785. Dutch. PMID: 28145212.
[36] AARC clinical practice guideline. Sampling for arterial blood gas analysis. American Association for Respiratory Care.RespirCare1992;37:913–917
[37] Shirani F, Salehi R, Naini AE, Azizkhani R, Gholamrezaei A. The effects of hypotension on differences between the results of simultaneous venous and arterial blood gas analysis. J Res Med Sci. 2011 Feb;16(2):188-94. PMID: 22091230; PMCID: PMC3214302.
[38] Bloom BM, Grundlingh J, Bestwick JP, Harris T. The role of venous blood gas in the emergency department: a systematic review and meta-analysis. Eur J Emerg Med. 2014 Apr;21(2):81-8. doi: 10.1097/MEJ.0b013e32836437cf. PMID: 23903783.
[39] Adrogué HJ, Rashad MN, Gorin AB, Yacoub J, Madias NE. Assessing acid-base status in circulatory failure. Differences between arterial and central venous blood. N Engl J Med. 1989 May 18;320(20):1312-6. doi: 10.1056/NEJM198905183202004. PMID: 2535633.
[40] Putman CE, Loke J, Matthay RA, Ravin CE. Radiographic manifestations of acute smoke inhalation. AJR Am J Roentgenol. 1977;129(5):865–870.
[41]. Avva U, Lata JM, Kiel J. Airway Management. [Updated 2021 Jul 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470403/
[42] Siddiqui S, Gonem S, Wardlaw AJ. Advances in the management of severe asthma. Semin Respir Crit Care Med. 2012 Dec;33(6):666-84
[43] Muehlberger T, Kunar D, Munster A, Couch A. Efficacy of fiberoptic laryngoscopy in the diagnosis of inhalation injuries. Arch Otolaryngol Head Neck Surg. 1998;124(9):1003–1007.
[44] Weaver LK, Howe S, Hopkins R, Chan KJ. Carboxyhemoglobin half-life in carbon monoxide-poisoned patients treated with 100% oxygen at atmospheric pressure. Chest. 2000;117(3):801–808
[45] Peñuelas O, Frutos-Vivar F, Esteban A. Noninvasive positive-pressure ventilation in acute respiratory failure. CMAJ. 2007 Nov 6;177(10):1211-8. doi: 10.1503/cmaj.060147. PMID: 17984471; PMCID: PMC2043058.
[46] Lin M, Yang YF, Chiang HT, Chang MS, Chiang BN, Cheitlin MD. Reappraisal of continuous positive airway pressure therapy in acute cardiogenic pulmonary edema. Short-term results and long-term follow-up. Chest. 1995 May;107(5):1379-86. doi: 10.1378/chest.107.5.1379. PMID: 7750335.
[47] Karagiannidis C, Bein T, Weber-Carstens S. Indikationen und Grenzen der ECMO-Therapie: Überlegungen zur Evidenz, Therapieentscheidung und ethischen Herausforderung [Indications and limitations of ECMO therapy: Considerations on evidence, treatment decisions and ethical challenges]. Med Klin Intensivmed Notfmed. 2019 Apr;114(3):207-213. German. doi: 10.1007/s00063-019-0533-3. Epub 2019 Feb 5. PMID: 30721332.
[48] Luks AM, Swenson ER, Bärtsch P. Acute high-altitude sickness. Eur Respir Rev. 2017 Jan 31;26(143):160096. doi: 10.1183/16000617.0096-2016. PMID: 28143879.
[49] Guérin C, Albert RK, Beitler J, Gattinoni L, Jaber S, Marini JJ, Munshi L, Papazian L, Pesenti A, Vieillard-Baron A, Mancebo J. Prone position in ARDS patients: why, when, how and for whom. Intensive Care Med. 2020 Dec;46(12):2385-2396. doi: 10.1007/s00134-020-06306-w. Epub 2020 Nov 10. PMID: 33169218; PMCID: PMC7652705.
[50] Odutayo A, Desborough MJ, Trivella M, Stanley AJ, Dorée C, Collins GS, Hopewell S, Brunskill SJ, Kahan BC, Logan RF, Barkun AN, Murphy MF, Jairath V. Restrictive versus liberal blood transfusion for gastrointestinal bleeding: a systematic review and meta-analysis of randomised controlled trials. Lancet Gastroenterol Hepatol. 2017 May;2(5):354-360. doi: 10.1016/S2468-1253(17)30054-7. Epub 2017 Mar 23. PMID: 28397699.
[51] Vahdatpour C, Collins D, Goldberg S. Cardiogenic Shock. J Am Heart Assoc. 2019 Apr 16;8(8):e011991. doi: 10.1161/JAHA.119.011991. PMID: 30947630; PMCID: PMC6507212.
[52] Mahmud E, Cavendish JJ, Salami A. Current treatment of peripheral arterial disease: role of percutaneous interventional therapies. J Am Coll Cardiol. 2007 Aug 7;50(6):473-90. doi: 10.1016/j.jacc.2007.03.056. Epub 2007 Jul 23. PMID: 17678729.
[53] Dumestre D, Nickerson D. Use of cyanide antidotes in burn patients with suspected inhalation injuries in North America: a cross-sectional survey. J Burn Care Res. 2014;35(2):e112–e117
[54] Agrawal A, Palkar A, Talwar A. The multiple dimensions of Platypnea-Orthodeoxia syndrome: A review. Respir Med. 2017 Aug;129:31-38. doi: 10.1016/j.rmed.2017.05.016. Epub 2017 May 31. PMID: 28732833.





1 thought on “Hypoxia in the ED Setting: Systematic Approach and Management”
Pingback: Hipoxia en las urgencias - Gerontogeriatría