Here’s another case from Medical Malpractice Insights – Learning from Lawsuits, a monthly email newsletter for ED physicians. The goal of MMI-LFL is to improve patient safety, educate physicians and reduce the cost and stress of medical malpractice lawsuits. To opt in to the free subscriber list, click here.
Chuck Pilcher, MD, FACEP
Editor, Med Mal Insights
Don’t be FOOL-ed by FOOSH
Wrist injuries are scaphoid fractures until proven otherwise
Proper management and patient teaching avoid a lawsuit
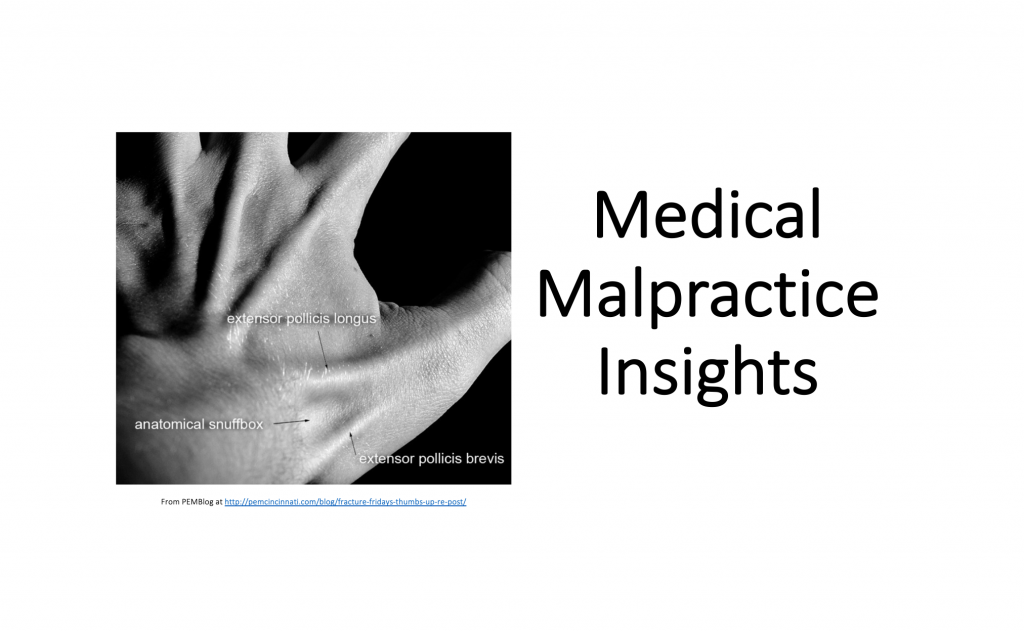
Facts: An adult male falls on his outstretched hand (FOOSH). He seeks care in the ED where he is seen by a PA who documents pain, swelling, decreased mobility/range of motion, and ecchymosis of the wrist. “Snuff box” tenderness is not mentioned. An x-ray is reported as normal but not viewed  by the PA. The PA diagnoses a wrist sprain, the wrist is wrapped with an Ace bandage, and he is advised to follow up with his PCP if not improving. He does so, but no further action is taken. He continues to have pain and is eventually diagnosed with a scaphoid fracture and non-union requiring surgery, resulting in permanent decreased range of motion. The PA’s supervising physician’s only evidence of involvement is his “clicktation” that created a macro in support of the PA’s care.
by the PA. The PA diagnoses a wrist sprain, the wrist is wrapped with an Ace bandage, and he is advised to follow up with his PCP if not improving. He does so, but no further action is taken. He continues to have pain and is eventually diagnosed with a scaphoid fracture and non-union requiring surgery, resulting in permanent decreased range of motion. The PA’s supervising physician’s only evidence of involvement is his “clicktation” that created a macro in support of the PA’s care.
Plaintiff: You didn’t document how I hurt my wrist. You should have checked me for “snuff-box” tenderness. FOOSH injuries are high-risk for scaphoid fractures, even when the x-ray is negative. You told me nothing about that possibility. An Ace wrap was inadequate. You should have put me in a splint and recommended a repeat x-ray if I did not improve. You never consulted your supervising physician, who should have informed me that I needed closer follow-up.
Defense: We told you to seek follow-up. You did. If you thought you weren’t improving quickly enough, you should have returned to the ED or sought further care on your own in a more timely fashion. Immobilization does not guarantee that a scaphoid fracture will heal.
Result: Defense verdict at trial, most likely due to appropriate instructions not being followed.
Takeaways:
- Think scaphoid fracture first. It’s easier to make a diagnosis that’s in our differential.
- Documenting the absence of “snuff box” tenderness is a valuable defense against a missed diagnosis.
- A scaphoid fracture is often occult, almost defining the word “occult.” If present, repeat films 10-20 days later for reevaluation.
- A scaphoid fracture is a common miss in radiology. Viewing the x-rays yourself with the knowledge of the clinical situation is a worthwhile practice.
- If snuff-box tenderness is present, x-rays are negative, and a scaphoid fracture is strongly suspected, an MRI is more sensitive than a CT scan for diagnosis.
- Non-union is common, more often with fractures in the proximal 1/3 of the scaphoid, which is dependent upon intra-osseous blood flow.
- Immobilization in a thumb spica splint if snuff box tenderness is equivocal is the best approach.
- Unless the diagnosis of a “sprain” is certain, tell patients about the possibility of an occult fracture and the importance of follow-up.
- When signing off on the work of a mid-level provider, remain aware of the most common “misses” that any of us can make.
References:
Scaphoid Fractures. Queens University School of Medicine, Kingston, Ontario, Canada.
OrthoBullets– Scaphoid Fractures
emDocs– Wrist Injuries
WikEM– Scaphoid Fractures
Good judgment comes from experience, and experience comes from bad judgment.
Variously attributed




