
Not Your Typical Chest Pain Case…
A illuminating case of chest pain and the importance of short PR on ECG.
Not Your Typical Chest Pain Case… Read More »
A illuminating case of chest pain and the importance of short PR on ECG.
Not Your Typical Chest Pain Case… Read More »
The sick MI patient: What are the scary complications, and what can you do?
The Sick MI Patient Read More »
“I’ve got a pulse,” you hear the nurse shout. Finally, a sigh of relief comes over the crowded resuscitation room and you take a moment to reflect on what just happened… but, your work is just now about to truly begin. It is up to you to determine why the patient died in the first place and determine which crucial steps need to be initiated to increase your patient’s chance of survival.
I’ve got a pulse… now what? – Post-Arrest Care in the Acute Setting Read More »
Editor’s note: This article was listed in the LITFL Review 154’s “Best of #FOAMed” section.
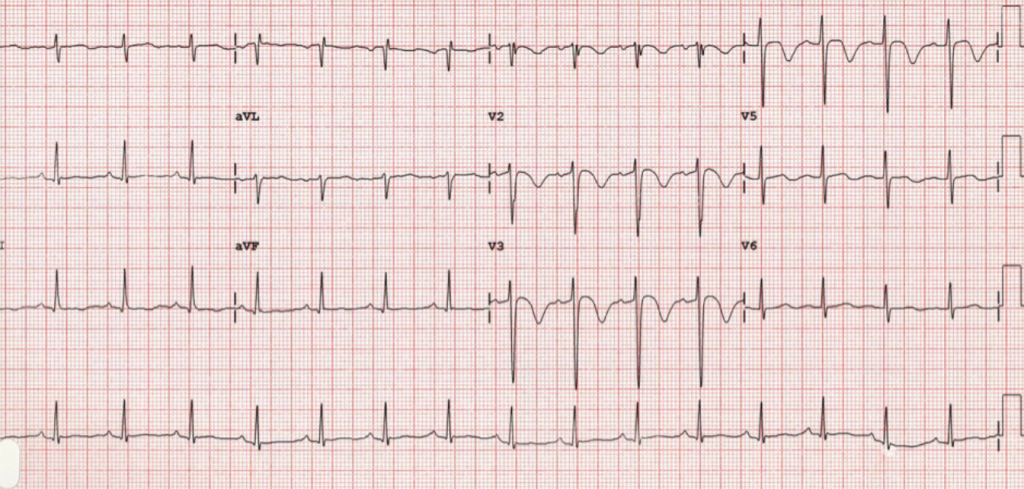
The left bundle branch arises from the Bundle of His, and subsequently is divided into the anterior and posterior fascicles. The anterior fascicle is usually supplied by septal perforators from the Left Anterior Descending artery, and the posterior fascicle typically has a dual supply from septal perforators from the Left Anterior Descending artery and the Posterior Descending artery (arising from the Right Coronary).Electrocardiographically, a LBBB is defined as QRS duration greater than or equal to 120 ms; a broad-notched or slurred R wave in leads I, aVL, V5, and V6; absent Q waves in leads I, V5, and V6; and an R peak time >60 ms in leads V5 and V6 but normal in leads V1 to V3 (1). LBBB can be transient and/or rate-related (1). These morphologic changes make it difficult to discern whether or not a patient presenting to the emergency department with chest pain is experiencing a STEMI. […]
Left Bundle Branch Block in Myocardial Infarction: An Update Read More »
“We should only intervene under very specific circumstances”
Asymptomatic hypertension in the ED: Should we be screening for end-organ damage? Should we intervene? Joshua Bucher, MD covers the 2013 ACEP Clinical Policy addressing these common questions.
Asymptomatic Hypertension Read More »

“Untoward patient-centered effects had not definitively been demonstrated until recently”
Nick Johnson, MD (@NickJohnsonMD) discusses the recent evidence comparing isotonic saline with balanced fluids for resuscitation of septic patients.
Fluid Resuscitation: Isotonic Saline vs Balanced Fluids Read More »

“Higher d-dimer levels correlate with more segments of the aorta involved, with false lumen type dissections, and with higher mortality rates”
D-dimer has great sensitivity for aortic dissection, but its true clinical utility in the workup of this high-risk diagnosis remains undefined. Tim Schaefer, MD reviews diagnosis and management, as well as the recent literature on the role of the d-dimer.
D-Dimer in Aortic Dissection Workup Read More »
“Significant cause of strokes in young/middle aged patients”
Olabiyi Akala, MD summarizes the signs, symptoms, and imaging options for making the diagnosis of carotid artery dissection, and discusses current controversies in management.
Carotid Artery Dissection Read More »
“One of the essential instant recognition abnormalities on ECG”
Knowing how to spot Wellens’ morphology is crucial, but knowing when to expect those ECG changes is the other half of the battle. In this excellent article, Brendon Browning, DO covers the intricacies of this deadly entity, including diagnostic criteria, management pitfalls, and how to identify mimics.

“Some will not have a palpable pulse, and unfortunately, manual BP cannot be obtained. In addition, pulse oximetry is unreliable”
No pulse? No problem! Manpreet Singh, MD covers a stepwise approach to troubleshooting ventricular assist device complications in the emergency department.
Ventricular Assist Device Management Read More »