Author: Priya Misir, MD (EM Resident Physician, Icahn School of Medicine at Mount Sinai Hospital) // Reviewed By: Anthony DeVivo, DO (@anthony_devivo, EM-Critical Care Fellow, Icahn School of Medicine- Mount Sinai Hospital): Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit); and Manpreet Singh, MD (@MprizzleER)
Welcome back to Unlocking Common ED Procedures! Today, we focus on resuscitative thoracotomy.

Check out our downloadable procedure card with QR code link to the article. Print them out and be ready to go over it with your learners!
Case:
A 30 year-old male presents to the ED after sustaining a gunshot wound to the left anterior chest. On arrival of EMS at the scene, the patient was noted to be groaning with spontaneous eye movement. However, the patient decompensated while en route to the hospital and CPR was initiated. Initial vitals in the field were HR 125, BP 85/40, RR 24, O2 sat 90%. Patient was transported by EMS with total time to hospital less than 10 minutes with continuous CPR. During the next pulse check in the ED, no palpable pulse is felt and the blood pressure is unable to be obtained. The patient is intubated and upon placement of bilateral chest tubes, you notice greater than 1L of blood return from the left chest. An entry wound is observed in the left chest. No signs of head trauma or other injury are identified on secondary and tertiary surveys. FAST is positive for pericardial effusion. What is the next step? Should an emergency thoracotomy be performed? Does it matter if you are in a community ED or a tertiary care center? What if there is no surgeon on site?
Background:1,2
The first successful resuscitative thoracotomy in a trauma patient in cardiac arrest was described by Igelsrud in 1906. Spangaro later described the classic left anterolateral incision approach in 1906, and Beall later pioneered immediate resuscitative thoracotomy in trauma patients in the emergency department or operating room in 1961.1 The physiologic aims of resuscitative thoracotomy include addressing hypovolemic and cardiogenic shock precipitated by significant structural injury and massive hemorrhage. Providers achieve this through control of cardiac and intrathoracic hemorrhage, cardiac massage, and evacuation of massive air embolism. Resuscitative thoracotomy is a resource intensive procedure and clinicians must often assess its potential futility within seconds to minutes. Survival rates are greatest in patients with isolated cardiac injury presenting in shock, but vary greatly across the literature. Survival rates range 2-35% based on injury mechanism and patient condition at initial presentation.2,3
Indications:
Algorithm4
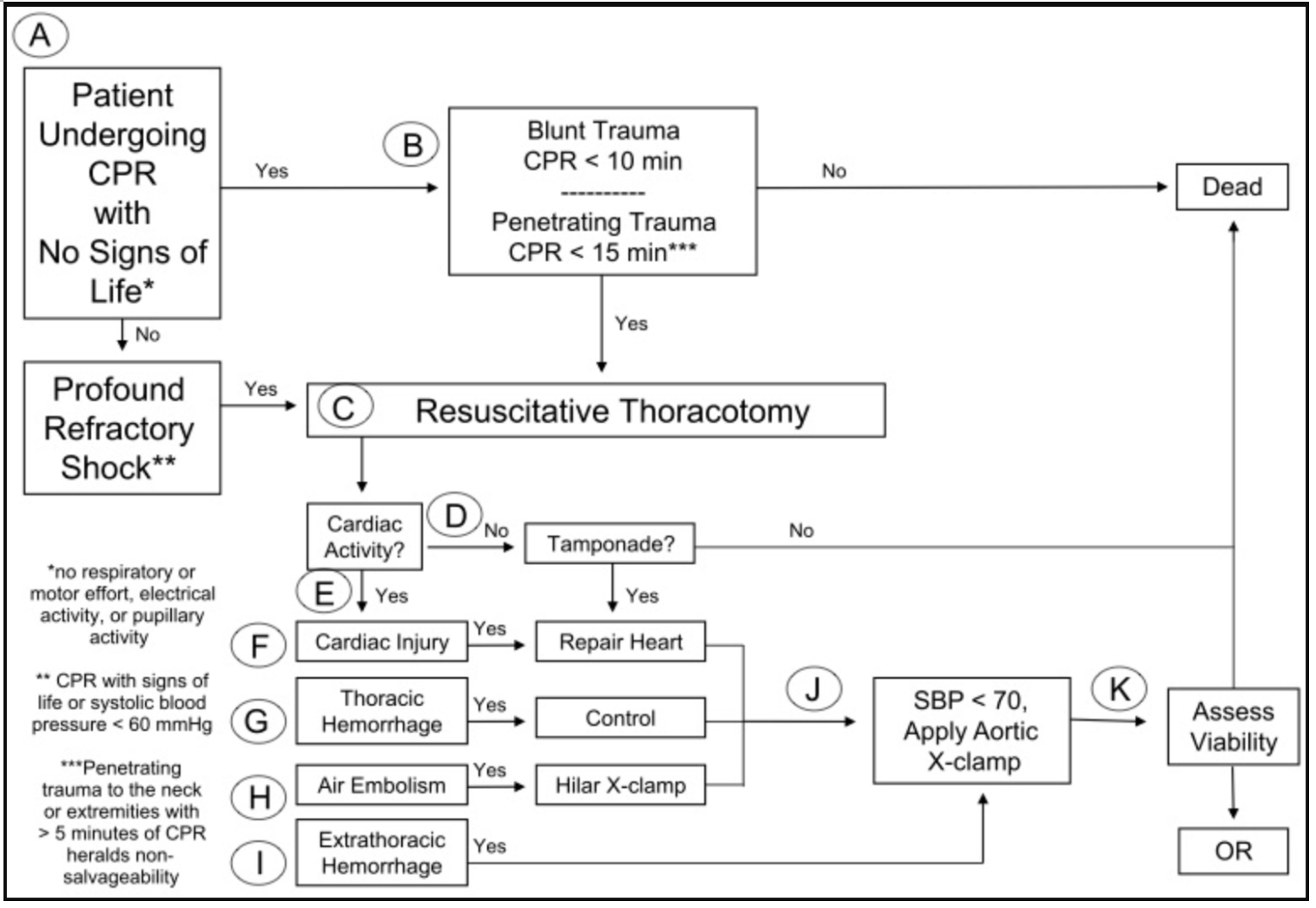
The best candidates for successful ED thoracotomy are patients with penetrating trauma who present with severe hemodynamic instability unresponsive to medical resuscitation, or patients with penetrating trauma who were observed to have signs of life (pulses, organized cardiac rhythm, blood pressure, reactive pupils, respirations, purposeful movement) but lost vital signs subsequently.
Survival rates can be as high as 35% in hypotensive patients with isolated cardiac injuries and are approximately 20% in patients with isolated cardiac injuries presenting without signs of life.2
Contraindications:
General Contraindications include patients with:1
- Nonsurvivable TBI
- Rigor Mortis
- Presence of other non-survivable injuries
- No pulse or blood pressure on EMS arrival in the field
Penetrating Trauma Contraindications:5
- CPR >15 minutes with no signs of life (pupillary response, respiratory effort, motor activity)
Blunt Trauma Contraindications:4
- CPR >10 minutes with no signs of life
- Cardiac rhythm is asystole on arrival with no evidence of pericardial tamponade
Survival rates significantly decrease in patients with blunt trauma, with approximately 2% survival in patients presenting in shock and only 1% survival in patients presenting without vital signs.2 Eastern Trauma guidelines list blunt trauma patients without vital signs on arrival as a relative contraindication to performing ED thoracotomy.3
Procedure:
There are two approaches for thoracotomy. One is to start with a left anterolateral thoracotomy, and the alternate is bilateral finger thoracostomies followed by connection with lateral incision.
1.) Patient’s undergoing thoracotomy should be intubated; however, this should not delay starting the procedure and can be performed by another member of the trauma team. On arrival bilateral chest tubes should be placed. Placement of a right sided chest tube enables clinicians to identify potential injuries in the right thorax. In order to expose the heart and lungs, a left anterolateral thoracotomy is performed regardless of site of penetrating trauma. The incision begins at the 4thor 5th intercostal space and extends from the posterior axillary line to the sternum. Retractors are inserted to expose the left thorax for evacuation of blood and clamping of vasculature to achieve hemostasis. The pericardium is then exposed by moving the left lung, and a pericardiotomy is performed through incision of the pericardial sac extending from apex to aortic root. The heart can then be exposed with evacuation of pericardial blood or clots and inspection for myocardial defects or lacerations. These injuries can be repaired with sutures or staples, and larger defects may be tamponaded off with a foley balloon. The aorta is then cross clamped and cardiac massage is initiated. Presence of hemothorax often makes it difficult to distinguish the aorta from the esophagus. To locate the aorta, the anterior aspect of the spinal column should be palpated and the parietal pleura overlying the aorta will then be located and can be digitally opened.1 Placement of a nasogastric tube or bougie into the esophagus can help distinguish the aorta from the esophagus through palpation.1,6If no etiology of hemodynamic collapse is identified, the incision can be extended to the right side of the chest for inspection of the right thorax and better visualization of the right atrium and ventricle. The most common injuries that can be intervened upon involve the right ventricle, due to its anterior location in the chest cavity. If return of spontaneous circulation is achieved, the patient should be transported to the operating room for definitive intervention.
2.) In an alternate approach, bilateral finger thoracostomies can be made initially and then connected through a lateral incision to complete the thoracotomy, which may provide faster exposure of the thoraces, pericardium, and great vessels. Studies have shown that there is no significant difference in the time required to make the full clamshell incision (2.33 minutes) compared to the left anterior thoracotomy incision (2.39 minutes).7 Additionally, the clamshell incision (bilateral anterior thoracotomy) provides superior visualization and facilitates significantly faster control of cardiac defects (1.85 minutes) compared to left anterior thoracotomy (4.16 minutes).7,8 This data suggests that clamshell incision may be the better approach in ED thoracotomies, as superior visualization with reduced time to intervention is imperative in users who are not routinely visualizing intrathoracic structures.
Positioning
The patient should be in supine position with arms placed above the head.
Anatomy9

Incision should begin in the posterior mid axillary line at 5th intercostal space, which lies one rib space below the nipple line in males and the inframammary fold in females.

Clamshell incision with open chest after rip spreader placement, enabling full visualization of heart, bilateral lung fields. Pericardium displaced (T shaped incision should be made), aorta can be cross clamped or compressed with a hand by entering field posterior to left lung (depicted above).
Stepwise Review:9
Left Anterior Thoracotomy
The classic left anterior thoracotomy steps are as follows:
- Rapid application of skin preparation should be applied over the entire chest and abdomen (ie. Betadine, chlorhexidine). However, this should not delay the start of the thoracotomy.
- Identify the 4th or 5th intercostal space (one rib space below the nipple line in males or below the inframammary fold in females), and make an anterolateral incision beginning at the sternum following the rib curvature to the left posterior axillary line.
- The lung should be held away from the chest wall while the rest of the layers of the chest wall (musculature, parietal pleura) are cut through using mayo scissors. These layers should not be cut with the scalpel due to risk of lacerating the heart and lungs.
- The incision is opened using a Finochietto retractor or rib spreaders to maximal expansion for sufficient exposure. The rib spreaders should be inserted such that the hand crank and long metal bar are lateral to the incision made with the bar pointing towards the feet to enable maximal exposure.
- A pericardiotomy is performed next by lifting the pericardium with forceps and making a midline, longitudinal incision through the pericardial sac using scissors. During this step is important to avoid damaging the phrenic nerves, which are located in the lateral walls of the pericardial sac.
- Next the heart is exposed and all blood and clot should be evacuated from the pericardial sac.
- The heart is inspected systematically for cardiac defects. Bleeding should be controlled through temporary occlusion with gauze or overlying pressure held by a finger.
- Defects greater than 1cm can be temporarily tamponaded by a foley balloon. If these measures do not achieve hemostasis, a minimal amount of sutures (non-absorbable size 0/0 or 1/0 monofilament or braided) can be used. It is important to avoid ligating the coronary arteries during this step.
- If the heart does not resume beating spontaneously, cardiac massage should be initiated with two handed technique directing blood towards the aortic route at approximately 80 bpm.
- The fascia surrounding the aorta should be bluntly dissected for optimal visualization of aortic structure, then a vascular clamp should be applied for temporary cross clamping.
- If after performing left anterior thoracotomy no injury is identified, poor visualization is present, or there is high suspicion of injury causing hemodynamic collapse in the right chest, the incision should be extended to the right side.
- Another anterolateral incision should be made beginning at the sternum extending to the right posterior axillary line along the 4th or 5th rib curvature to complete the bilateral thoracotomy.
- The remaining layers of the chest wall (musculature, parietal pleura) are cut through using mayo scissors.
- The sternum must be transected using a Gigli saw, Lebsche knife, trauma shears, or mayo scissors to gain full exposure.
- The incision is opened using a Finochietto retractor or rib spreaders to maximal expansion for sufficient exposure.
- The right thorax can then be inspected for inspected for injury and bleeding vasculature which can be clamped.
- If return of spontaneous circulation occurs, bleeding through the internal mammary arteries will occur, and the patient can be taken to the operating room for definitive management.
Bilateral Anterior Thoracotomy (Clamshell Incision)
- Rapid application of skin preparation should be applied over the entire chest and abdomen (ie. Betadine, chlorhexidine). However, this should not delay the start of the thoracotomy.
- Bilateral 4 cm incisions should be made in the mid axillary line at the 5th intercostal space using a 10 blade scalpel with the same technique used for tube thoracostomy placement.
- The thoracostomies are connected with a deep skin incision following the curvature of the ribs.
- The lung should be held away from the chest wall bilaterally while the rest of the layers of the chest wall (musculature, parietal pleura) are cut through using mayo scissors. These layers should not be cut with the scalpel due to risk of lacerating the heart and lungs.
- The sternum is then transected with a Gigli saw by passing forceps or a large clamp under the sternum. The Gigli saw is then grasped with the clamp or forceps and pulled under the sternum. If no Gigli saw is available, transect the sternum using a Lebsche knife, mayo scissors, or trauma shears.
- Long strokes are used to cut through the sternum from inside out
- The incisions are opened using a Finochietto retractor or rib spreaders to maximal expansion for sufficient exposure. The rib spreaders should be inserted such that the hand crank and long metal bar are lateral to the incision made with the bar pointing towards the feet to enable maximal exposure.
- The thorax should be inspected for injury and bleeding vasculature which can be clamped
- A pericardiotomy is performed next by lifting the pericardium with forceps and making a midline, longitudinal incision through the pericardial sac using scissors. During this step is important to avoid damaging the phrenic nerves, which are located in the lateral walls of the pericardial sac.
- Next the heart is exposed and all blood and clot should be evacuated from the pericardial sac.
- The heart is inspected systematically for cardiac defects. Bleeding should be controlled through temporary occlusion with gauze or overlying pressure held by a finger. Defects greater than 1cm can be temporarily tamponaded by a foley balloon. If these measures do not achieve hemostasis, a minimal amount of sutures (non-absorbable size 0/0 or 1/0 monofilament or braided) can be used. It is important to avoid ligating the coronary arteries during this step.
- If the heart does not resume beating spontaneously, cardiac massage should be initiated with two handed technique directing blood towards the aortic route at approximately 80 bpm.
- The fascia surrounding the aorta should be bluntly dissected for optimal visualization of aortic structure, then a vascular clamp should be applied for temporary cross clamping.
- If return of spontaneous circulation occurs, bleeding through the internal mammary arteries will occur.
- The patient should be taken to the operating room for definitive management.
Pearls/Pitfalls:4,10–12
-The incision made should be curvilinear, following the curvature of the ribs. This is imperative to avoid transecting the ribs, creating sharp edges, which leads to inadequate exposure.
-Avoid using the scalpel to cut through intercostal muscles and parietal pleura. Use of mayo scissors will help reduce the likelihood of iatrogenic laceration to the heart and lungs.
-In order to minimize lung volume obscuring view of the pericardium, right mainstem intubation can be performed.
-Initial hemostasis in cardiac defects can be achieved through pressure from a finger. Finger should be placed directly on top of defect and not through the defect, as to not extend borders of laceration.
– A foley balloon can be used as a temporizing measure to achieve hemostasis in cardiac wall defects >1cm. Purse string sutures should be placed around the foley balloon, allowing removal of balloon and rapid closure of defect through pulling the ends together.
-Ensure a vascular clamp is used to cross clamp the aorta instead of a regular clamp to avoid crush injuries.
-Tranexamic Acid (1g IV) given within 3 hours of injury to great vessels may improve survival outcomes through controlling severe hemorrhage.10–12
Complications:
Structural Damage
Complications from ED thoracotomy include potential damage to virtually all structures present in the chest cavity. These include lacerations to the heart, coronary arteries, aorta, phrenic nerves, esophagus, lungs, and avulsion of aortic branches to mediastinal components. Ligation of coronary arteries resulting in infarction of myocardial tissue can occur during repair of myocardial defects. These types of injury require definitive surgical management.
Post-operative Complications
Post-operative complications for patients that survive the procedure include recurrent hemorrhage from the chest, and infection of the pericardium, pleural space, or chest wall. Management of these complications include blood transfusion, antibiotics, and potential return to the OR for washout or for exploration and hemostatic measures. Additionally, dense pleural adhesions often form after this type of procedure, rendering difficult future procedures that may require sternotomy (ie Coronary Artery Bypass Graft).
Risk of Infection Transmission to Healthcare Personnel2
Healthcare workers are at increased risk of exposure to needlesticks or injury from sharps due to rapid incisions and the tools used during this procedure. Studies have shown that patients requiring thoracotomy often have a higher exposure to infections with bloodborne transmission including HIV, Hepatitis B, and Hepatitis C. Proper PPE and adequate precautions should be taken to prevent sharps injury and exposure.
Community ED Considerations
The Eastern Trauma guidelines were formulated through review of data exclusively from Level 1 Trauma Centers. Therefore, these recommendations of when ED thoracotomy is indicated may not be applicable to community hospitals or single coverage EDs. In these cases, the time to definitive management (how quickly a surgeon can arrive at the site, time to prepare the operating room etc) must be considered, as this is necessary for ultimate patient survival and prevention of prolonged ischemia. If the trauma patient must remain in the ED for a significant amount of time, there is a high likelihood of sudden decompensation. However, even under circumstances where significant delays to definitive management may be present, studies have shown as high as an 11% long-term survival rate post ED thoracotomy.13Clinical judgement should be used regarding the potential futility of this resource extensive procedure in ill-equipped environments due to lack of immediate surgical intervention. Alternatives such as ultrasound guided aortic compression while continuing administration of blood products and external CPR may be useful if it is feasible to obtain rapid transfer to a Level 1 Trauma Center for definitive management.14
Rapid Procedure Review:
–Position patient in supine orientation with arms above head.
-Make bilateral thoracostomy incisions in posterior mid axillary lines at 5th rib space.
-Extend thoracostomy incision from left anterior chest wall to sternum, repeat on right side.
-Use mayo scissors to cut through remaining layers of chest wall.
-Use Gigli saw to transect the sternum.
-Use retractors or rib spreaders to maximum expansion to visualize chest cavity, inspect for hemorrhage/clot.
-Perform pericardiotomy using scissors to make a midline incision extending from apex to aortic root.
-Evacuate pericardium of clot, blood.
-Inspect heart for defects or laceration, attempt to achieve hemostasis.
-Cross clamp the aorta.
-Begin cardiac massage as necessary.
-If ROSC achieved, take patient to OR for definitive management.
References:
- Pust GD, Namias N. Resuscitative thoracotomy. International Journal of Surgery. 2016;33(Part B):202-208. doi:10.1016/j.ijsu.2016.04.006
- Cothren CC, Moore EE. Emergency department thoracotomy for the critically injured patient: Objectives, indications, and outcomes. World Journal of Emergency Surgery. 2006;1(1):4. doi:10.1186/1749-7922-1-4
- Seamon MJ, Haut ER, van Arendonk K, et al. An evidence-based approach to patient selection for emergency department thoracotomy. Journal of Trauma and Acute Care Surgery. 2015;79(1):159-173. doi:10.1097/TA.0000000000000648
- Suliburk JW. Complications of emergency center thoracotomy. Texas Heart Institute journal. 2012;39(6):876-877. Accessed August 16, 2020. http://www.ncbi.nlm.nih.gov/pubmed/23304043
- Burlew CC, Moore EE, Moore FA, et al. Western Trauma Association Critical Decisions in Trauma. Journal of Trauma and Acute Care Surgery. 2012;73(6):1359-1363. doi:10.1097/TA.0b013e318270d2df
- Sudarshan M, Cassivi SD. Management of traumatic esophageal injuries. Journal of Thoracic Disease. 2019;11(Suppl 2):S172-S176. doi:10.21037/jtd.2018.10.86
- Flaris AN, Simms ER, Prat N, Reynard F, Caillot JL, Voiglio EJ. Clamshell incision versus left anterolateral thoracotomy. Which one is faster when performing a resuscitative thoracotomy? the tortoise and the hare revisited. World Journal of Surgery. 2015;39(5):1306-1311. doi:10.1007/s00268-014-2924-1
- Simms ER, Flaris AN, Franchino X, Thomas MS, Caillot JL, Voiglio EJ. Bilateral anterior thoracotomy (Clamshell Incision) is the ideal emergency thoracotomy incision: An anatomic study. World Journal of Surgery. 2013;37(6):1277-1285. doi:10.1007/s00268-013-1961-5
- Wise D, Davies G, Coats T, Lockey D, Hyde J, Good A. Emergency thoracotomy: “How to do it.” Emergency Medicine Journal. 2005;22(1):22-24. doi:10.1136/emj.2003.012963
- Olldashi F, Kerçi M, Zhurda T, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): A randomised, placebo-controlled trial. The Lancet. 2010;376(9734):23-32. doi:10.1016/S0140-6736(10)60835-5
- Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military application of tranexamic acid in trauma emergency resuscitation (MATTERs) study. Archives of Surgery. 2012;147(2):113-119. doi:10.1001/archsurg.2011.287
- Ker K, Edwards P, Perel P, Shakur H, Roberts I. Effect of tranexamic acid on surgical bleeding: Systematic review and cumulative meta-analysis. BMJ (Online). 2012;344(7858). doi:10.1136/bmj.e3054
- MacDonald JR, McDowell RM. Emergency department thoracotomies in a community hospital. Journal of the American College of Emergency Physicians. 1978;7(12):423-428. doi:10.1016/S0361-1124(78)80126-9
- Michel WB, Lachance A, Turcotte AS, Morris J. Point-of Care Ultrasonographically Guided Proximal External Aortic Compression in the Emergency Department. Annals of Emergency Medicine. 2019;74(5):706-710. doi:10.1016/j.annemergmed.2019.06.007
- Tintinalli J. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide (8th Ed.). Faculty Bookshelf. Published online January 1, 2016. Accessed August 16, 2020. https://hsrc.himmelfarb.gwu.edu/books/68




