Author: Anthony DeVivo, DO (@anthony_devivo, EM Resident Physician, Mount Sinai St. Luke’s-West) // Edited by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit); and Manpreet Singh, MD (@MprizzleER)
emDocs is proud to introduce a new series focused on emergency medicine procedures! This series will provide key information on procedural steps, indications, contraindications, pearls, and pitfalls. Today, the lumbar puncture!

Check out our new downloadable procedure card with QR code link to the article. Print them out and be ready to go over it with your learners!
Case
A 22-year-old male with no significant past medical history presents to the Emergency Department for 8 hours of a bitemporal headache which woke him from sleep this morning. He says the headache is very severe and the worst he’s had. He affirms the headache has mildly improved from its onset but since then has developed nausea, light sensitivity, and neck stiffness. He denies fever, chills, weakness or numbness of the extremities, or syncope. He has no recent travel, sick contacts, history of headaches in the past, or any history of IV drug use.
Background
This presentation is well known to emergency medicine physicians as a classic story concerning for subarachnoid hemorrhage. The workup generally begins with a noncontrast CT of the head to assess for blood in the subarachnoid space, which is nearly 100% sensitive if performed within 6 hours of symptoms onset. However, after 6 hours, the sensitivity begins to decline and quickly becomes inadequate for ruling out a subarachnoid hemorrhage.1 A CT angio may also be performed order to assess for any venous malformations that might be the potential source of bleeding. However, in cases of high clinical suspicion, a CT angio without evidence of vascular malformation is controversial in its ability to rule out SAH. Inevitably, even with all the technology and current literature at our fingertips, a subarachnoid hemorrhage in a patient with this timeframe and high clinical suspicion must be ruled out with a lumbar puncture.
Lumbar puncture is the primary means by which physicians gain access to the cerebrospinal fluid (CSF) for analysis for a variety of suspected conditions. This procedure is performed by introducing a hollow 20-22 gauge needle into the cerebrospinal space beneath the lower lumbar vertebra.2-3 Below we will further discuss indications, contraindications, performing the procedure, and complications of a lumbar puncture and their management.
Indications:2-3
- Concern for infectious process within the central nervous system
- Concern for various etiologies of encephalitis
- Assessment of the CSF for blood or xanthochromia in order to rule out subarachnoid hemorrhage
- Evaluation for inflammatory processes in the central nervous system such as Guillain-Barré
- Therapeutic lumbar puncture for cerebrospinal fluid pressure reduction in such cases as idiopathic intracranial hypertension (pseudotumor cerebri)
Contraindications:2-3,5-6
- Thrombocytopenia
- It has long been subscribed to that lumbar punctures should not be performed at platelet counts < 50,000 due to the concern for post procedural bleeding and hematoma formation. However, recent studies have shown no bleeding complications with platelet counts > 20,000. While additional randomized control trials would be necessary for more robust support of this practice, there is literature supporting the performance of a lumbar puncture with platelets > 20,000 with no signs of active bleeding.5-7
- Coagulopathy
- In addition to the concern for hematoma formation while performing a lumbar puncture on patients with thrombocytopenia, there is also a similar concern in the setting of coagulopathic patients. There is no current literature supporting a specific PT/INR that is associated with increased risk of post-procedural bleeding after the performance of a lumbar puncture. However, an INR of <1.5 has been considered the standard for the performance of any invasive procedure. This is due to the fact that an INR < 1.5 is associated with a 40% decrease in the function of factor VII; however, factor VII must be decreased by 55% in order to prolong the INR. Thus, an INR of < 1.5 or a factor VII function of > 40% is felt to be safe for invasive procedure with a risk of post-procedural bleeding.8-10 For more, see this emDocs post.
- Signs of cellulitis overlying the region at which the procedure will be performed
- Due to the concern for introduction of bacteria when entering the spinal canal, not only is the region cleansed and the procedure done under sterile conditions, but it is also a contraindication to perform the procedure through an area that is thought to have a superficial or deep space infection.
- Concern for spinal epidural abscess
- Similar to not performing a lumbar puncture through a cellulitic area, it is also a contraindication to perform one in an area where there are signs or a clinical suspicion for a spinal epidural abscess.10-11
- Trauma
- If there are any signs of recent trauma to the region at which the procedure is performed, traumatic injury must first be ruled out.
CT brain before LP:12-13
- Age >60 years
- Immunocompromised state
- History of previous Central Nervous System disease
- History of seizure within 1 week of presentation
- Presence of neurologic deficit on exam
- Altered mental status
CT findings to defer LP:
- Posterior fossa mass with signs/symptoms of compression of the 4th ventricle
- Acute intracranial hematoma
- Signs of increased intracranial pressure or midline shift
- Brainstem herniation
ED Indications for LP:2-5
- Suspected meningitis
- Suspected for subarachnoid hemorrhage that is unable to be ruled out with CT
- Suspected idiopathic intracranial hypertension
- Reduction of intracranial pressures in the setting of known or suspected idiopathic intracranial hypertension
- Assessment for Guillain Barre syndrome
The Procedure:2-5
- Landmarks
- The intervertebral spaces between L3-L4 and L4-L5 are the desired sites for needle entry since the spinal cord in an adult ends between L1 and L2. Ultrasound can assist with this. See this emDocs post.
- The posterior superior iliac crests correlate to the L4 spinous process in adults.
- The intervertebral spaces between L3-L4 and L4-L5 are the desired sites for needle entry since the spinal cord in an adult ends between L1 and L2. Ultrasound can assist with this. See this emDocs post.
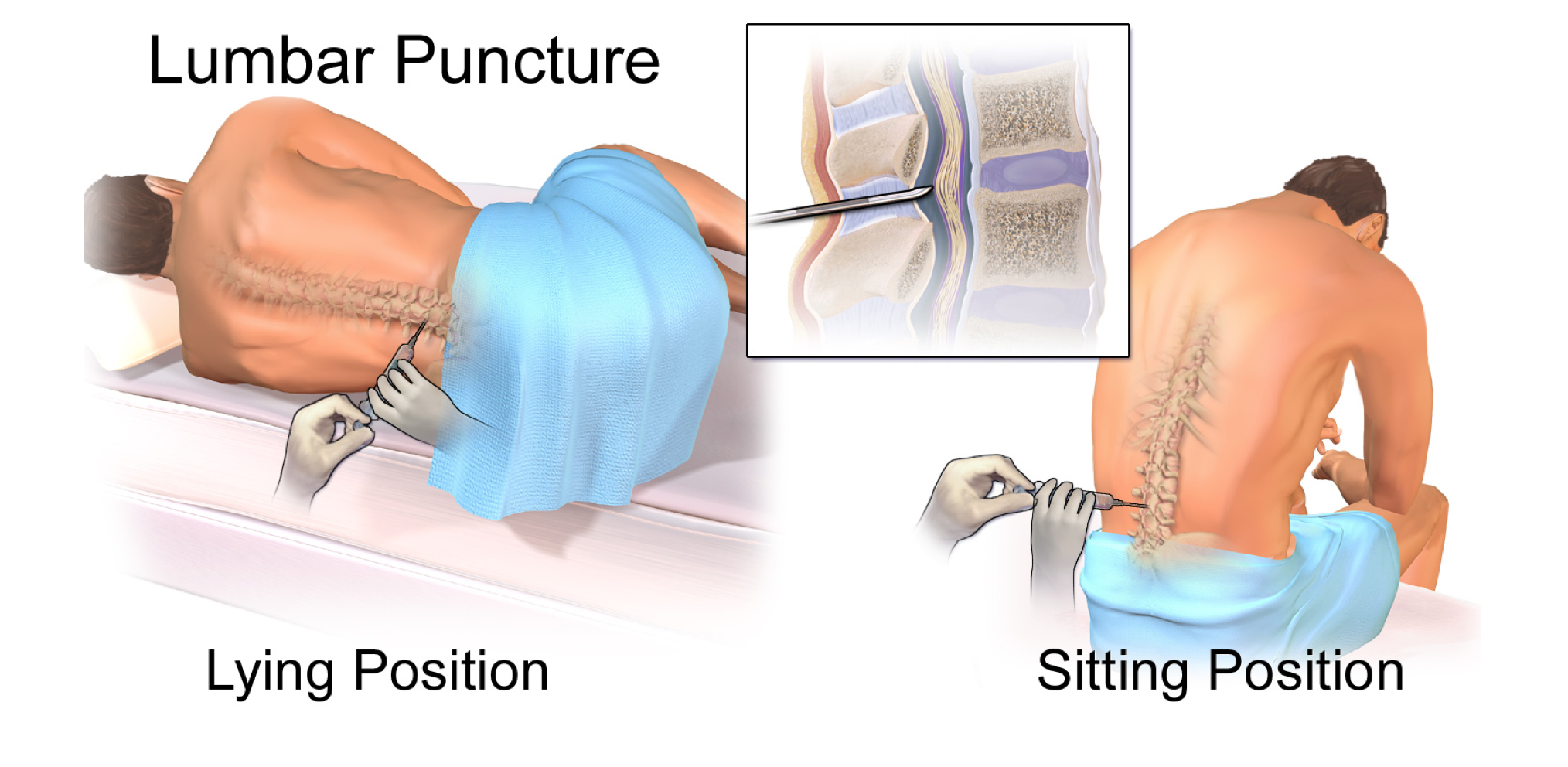
- Positioning
- Lateral recumbent position
- Have the patient lie on their side, with his/her knees tucked into the chest, in an attempt to widen the intervertebral spaces. It may help to have the patient hug a pillow into the chest, as well as have an assistant facilitate holding the patient’s knees into the chest to obtain optimal positioning.
- Seated position
- Have the patient sit forward off the side of the bed with his/her legs dangled over the edge. It may help to have the patient hug a pillow while leaning forward onto a Mayo stand, as well as place a stool under the feet so that the knees are tucked into the chest, in order to widen the intervertebral spaces.
- This technique requires the patient to be able to hold themselves up and be comfortable staying in a seated position throughout the procedure. It is advisable to have an assistant stand in front of the patient in case they begin to feel lightheaded during the procedure and fall forward.
- Of note, you can not measure an opening pressure when performing a lumbar puncture in the seated position.
- Preparation
- Once the patient is positioned to both the provider and patient’s satisfaction, a 10cm circumferential area around the intended procedure site should be sterilized with chlorhexidine or betadine. At this point, the provider should be wearing sterile gloves, mask, and cap in order to preserve the sterile field.
- The sterile drape should be applied within the confines of the initially sterilized region.
- The collecting tubes should be opened and set up in the numerical order in which you intend to collect your samples.
- Procedure
- Using 1% or 2% lidocaine for local anesthesia, inject the skin forming a small wheel of anesthetic over the area of intended entry, and then slowly insert into the desired tract leading to the intervertebral space demarcated by your landmarks.
- If you are performing this procedure without assistance, and lidocaine is not stored in your sterile, pre-packaged lumbar puncture kit, you may opt to tape the bottle of lidocaine to the wall nearest you in order to sterilely draw it up into a syringe.
- When utilizing a traditional spinal needle, insert the needle along the anesthetized tract with the bevel facing upwards and directing your needle midline, towards the umbilicus. When utilizing an atraumatic needle, it is important to take into consideration that this type of needle will not penetrate skin. Thus, a traditional introducer needle or anesthetic cutting needle must first be used to puncture the skin, after which the atraumatic needle may be utilized for the remainder of the procedure. While recent literature support the use of atraumatic needles as a means of significantly reducing the risk of post-procedural headache, many standardized lumbar puncture kits remain stocked with traditional cutting needles. If you prefer to utilize the atraumatic needle, you may need to obtain that outside the pre-set lumbar puncture kit.
- Upon entrance into the space, you may or may not feel a small pop. Once you have entered the space, remove the stylet and begin collecting CSF in the numerical order the tubes are labelled.
- Each tube requires at least 1cc of CSF.
- You may consider collecting an additional tube with 5-6cc of extra CSF for any further testing the inpatient or critical care team may want to order.
- Deep breaths may facilitate CSF flow once the spinal needle is in the intervertebral space.
- If the patient is in the lateral recumbent position, an opening pressure may be obtained prior to collection of CSF.
- Post-Procedural Care2-4,15-18
- Once the last tube is collected, reinsert the spinal needle stylet, remove the needle, and place a bandage over the insertion site.
- Classically, it is thought patients should lie supine for an hour after the LP to decrease the risk of post LP headache. While there is no substantial literature to support this as a definitive mechanism to avoid post-procedural headache, it theoretically may reduce post-procedural headaches.15-16
- Patients should be reassessed for post-procedure headache, as well as wound site assessment to assure no signs of hematoma formation.
- Post-Procedural Complications: One of the most common complications of a lumbar puncture is a post-procedural headache. While 90% of patient who experience this complication will affirm onset within 3 days of the procedure, it has been documented to have onset up to 14 days post-lumbar puncture. The headache is most commonly described as a pressure-like frontal or temporal headache that is postural, with improvement of symptoms while lying supine.15-18 The headache is often more severe and prolonged when beginning within 24 hours of the procedure. The incidence of a post-lumbar puncture headache varies between 5-20% in the outpatient setting.15-17 It has been shown that the use of smaller needles for puncture decrease the rate of post-procedural headaches.16-18 In addition, when using a beveled cannula, the bevel should be oriented in parallel with the spine in order to decrease trauma to the dural fibers, lending to a lower rate of post-dural puncture headaches.16 The initial mainstay approach to treatment of a post-lumbar puncture headache consists of fluid hydration and symptomatic control with nonsteroidal anti-inflammatory agents and acetaminophen for pain, as well as antiemetics for nausea and/or vomiting.16-19 In addition to traditional analgesics, oral and intravenous caffeine have been utilized in the treatment of post-dural puncture headaches with studies showing temporary symptom improvement utilizing intravenous caffeine.20 In the case of persistent headache or severe headache with intractable symptoms, an epidural blood patch should be performed in order to correct any CSF leak. A blood patch, commonly performed by anesthesiologists, is both a diagnostic and therapeutic procedure that should alleviate the patient of symptoms if the etiology of the headache is due to CSF leakage from the previous dural puncture.21 For more, see this emDocs post.
- Using 1% or 2% lidocaine for local anesthesia, inject the skin forming a small wheel of anesthetic over the area of intended entry, and then slowly insert into the desired tract leading to the intervertebral space demarcated by your landmarks.
- Lateral recumbent position
Pearls and Pitfalls
Positioning is vital to the success of any procedure, but particularly in the performance of a lumbar puncture. Both the patient and provider must be appropriately positioned and comfortable before starting.
- Take as much time as needed to become comfortable with the anatomic landmarks of the patient. If you are unable to consistently find an adequate space for the procedure, try using a marking pen.
- Having an assistant hold the patient in position during the needle insertion can help maintain ideal procedure conditions and assuring the patient stays adequately flexed in an attempt to widen the intervertebral spaces.
- If your first attempt is unsuccessful, reassess your plan, and try something different. This may be as simple as a slight repositioning of the patient, or attempting the procedure at a different intervertebral space.
- If you feel as if you are hitting bone, slightly withdraw the needle and redirect superiorly towards the umbilicus, as you’re likely hitting the vertebral spinous process.
- If there is any concern for elevated ICP, space occupying intracranial lesion, or abnormalities in the neurologic exam, a CT scan of the brain should be performed first.
- When a lumbar puncture is being performed due to concern for meningitis, a CT and/or lumbar puncture should not delay antibiotic administration.
References / Further Reading
- Perry, J. J., et al. “Sensitivity of Computed Tomography Performed within Six Hours of Onset of Headache for Diagnosis of Subarachnoid Haemorrhage: Prospective Cohort Study.” Bmj, vol. 343, no. jul18 1, 2011, pp. d4277–d4277. doi:10.1136/bmj.d4277.
- Rosen, Peter, et al. Rosen’s Emergency Medicine: Concepts and Clinical Practice. Elsevier, 2018.
- Fuller, Geraint, and Mark Manford. “Cerebrospinal Fluid and Lumbar Puncture.” Neurology, 2010, pp. 38–39., doi:10.1016/b978-0-7020-3224-0.00021-5. Ganti, Latha. Atlas of Emergency Medicine Procedures.
- Boon, J.m., et al. “Lumbar Puncture: Anatomical Review of a Clinical Skill.” Clinical Anatomy, vol. 17, no. 7, 2004, pp. 544–553., doi:10.1002/ca.10250.
- Holdgate, Anna, and Karyn Cuthbert. “Perils and Pitfalls of Lumbar Puncture in the Emergency Department.” Emergency Medicine Australasia, vol. 13, no. 3, 2001, pp. 351–358., doi:10.1046/j.1035-6851.2001.00239.x.
- Engelborghs, Sebastiaan, et al. “Consensus Guidelines for Lumbar Puncture in Patients with Neurological Diseases.” Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring, vol. 8, 2017, pp. 111–126., doi:10.1016/j.dadm.2017.04.007.
- Estcourt, Lise J, et al. “Use of Platelet Transfusions Prior to Lumbar Punctures or Epidural Anaesthesia for the Prevention of Complications in People with Thrombocytopenia.” Cochrane Database of Systematic Reviews, 2015, doi:10.1002/14651858.cd011980.
- Howard, Scott C. “Safety of Lumbar Puncture for Children With Acute Lymphoblastic Leukemia and Thrombocytopenia.” Jama, vol. 284, no. 17, 2000, p. 2222., doi:10.1001/jama.284.17.2222.
- Ning, S., et al. “Safety of Lumbar Punctures in Patients with Thrombocytopenia.” Vox Sanguinis, vol. 110, no. 4, 2016, pp. 393–400., doi:10.1111/vox.12381.
- Engelborghs, Sebastiaan, et al. “Consensus Guidelines for Lumbar Puncture in Patients with Neurological Diseases.” Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring, vol. 8, 2017, pp. 111–126., doi:10.1016/j.dadm.2017.04.007.
- Seydoux, C., and P. Francioli. “Bacterial Brain Abscesses: Factors Influencing Mortality and Sequelae.” Clinical Infectious Diseases, vol. 15, no. 3, 1992, pp. 394–401., doi:10.1093/clind/15.3.394.
- Hasbun, R. “Computed Tomography Of The Head Before Lumbar Puncture In Adults With Suspected Meningitis.” Infectious Diseases in Clinical Practice, vol. 11, no. 1, 2002, pp. 35–36., doi:10.1097/00019048-200201000-00015.
- Crevel, H. Van, et al. “Lumbar Puncture and the Risk of Herniation: When Should We First Perform CT?” Journal of Neurology, vol. 249, no. 2, 2002, pp. 129–137., doi:10.1007/pl00007855.
- Thomas, S R. “Randomised Controlled Trial of Atraumatic versus Standard Needles for Diagnostic Lumbar Puncture.” Bmj, vol. 321, no. 7267, 2000, pp. 986–990., doi:10.1136/bmj.321.7267.986.
- Sudlow, Cathie Lm, and Charles P Warlow. “Posture and Fluids for Preventing Post-Dural Puncture Headache.” Cochrane Database of Systematic Reviews, 2001, doi:10.1002/14651858.cd001790.
- Leibold, Robert A, et al. “Post-Dural-Puncture Headache: Characteristics, Management, and Prevention.” Annals of Emergency Medicine, vol. 22, no. 12, 1993, pp. 1863–1870., doi:10.1016/s0196-0644(05)80416-0.
- Safranek, Daniel J. “Post-Lumbar Puncture Headaches: Experience in 501 Consecutive Procedures.” The Journal of Emergency Medicine, vol. 11, no. 3, 1993, p. 368., doi:10.1016/0736-4679(93)90079-m.
- Flaatten, H., et al. “Puncture Technique and Postural Postdural Puncture Headache. A Randomised, Double-Blind Study Comparing Transverse and Parallel Puncture.” Acta Anaesthesiologica Scandinavica, vol. 42, no. 10, 1998, pp. 1209–1214., doi:10.1111/j.1399-6576.1998.tb05279.x.
- Ahmed, S V, et al. “Post Lumbar Puncture Headache: Diagnosis and Management.” Postgraduate Medical Journal, vol. 82, no. 973, 2006, pp. 713–716., doi:10.1136/pgmj.2006.044792.
- Lin, W. “Myth: Fluids, Bed Rest, and Caffeine Are Effective in Preventing and Treating Patients with Post-Lumbar Puncture Headache.” Western Journal of Medicine, vol. 176, no. 1, 2002, pp. 69–70., doi:10.1136/ewjm.176.1.69.
- Safa-Tisseront. “Effectiveness of Epidural Blood Patch in the Management of Post-Dural Puncture Headache.” Survey of Anesthesiology, vol. 46, no. 1, 2002, pp. 47–48., doi:10.1097/00132586-200202000-00047.





1 thought on “Unlocking Common ED Procedures – The Impossible Space: Lumbar Punctures”
Pingback: Lumbalpunktion – LP – Mind palace of an ER doc