
Author: Sophia Potalivo (MSIV, University of California Riverside School of Medicine); Niresh Perera, MD (Clinical US Fellow, UCLA Health); Flor Lema, MD (Clinical Ultrasound Fellow, UCLA Health); Jonathan Warren, MD (Clinical Ultrasound and EMS Fellow, Harbor-UCLA Medical Center) // Reviewed By: Manpreet Singh, MD; Brit Long, MD
Case:
A 56-year-old male presents to the emergency department after a high-speed motor vehicle accident. He is found to be tachypneic with severe 9/10 pain over his left chest. Chest x-ray and FAST reveal fifth and sixth anterior rib fractures, but no pneumothorax. No other injuries are found. Despite initial treatment with fentanyl, the patient continues to be in extreme pain and is tachypneic with shallow respirations. You consider how to best manage his pain.
Intro:
Chest trauma may result in significant pain with splinted respirations that decrease the ability to breathe with adequate tidal volumes. Shallow respirations increase the risk of atelectasis and pneumonia both within and outside of the hospital. Patients frequently require opioid pain control, which can adequately treat the pain but worsens the patient’s respiratory drive. Other negative effects of opioids include increased risk of dependence after hospitalization. These limitations highlight the need for alternative strategies, and multi-modal pain control can often be achieved via regional nerve blocks. Regional nerve blocks are also known to shorten the length of a patient’s hospital stay, lower in-hospital costs, and improve patient satisfaction.1
The serratus anterior plane block (SAPB) is one method of providing regional anesthesia to the third through sixth intercostal nerves, the long thoracic nerve, and the thoracodorsal nerves.2 As a result of the block, sensation will be decreased at the T2-T9 level on the anterior, ipsilateral side of the injection for as long as six to twelve hours.3,4,5
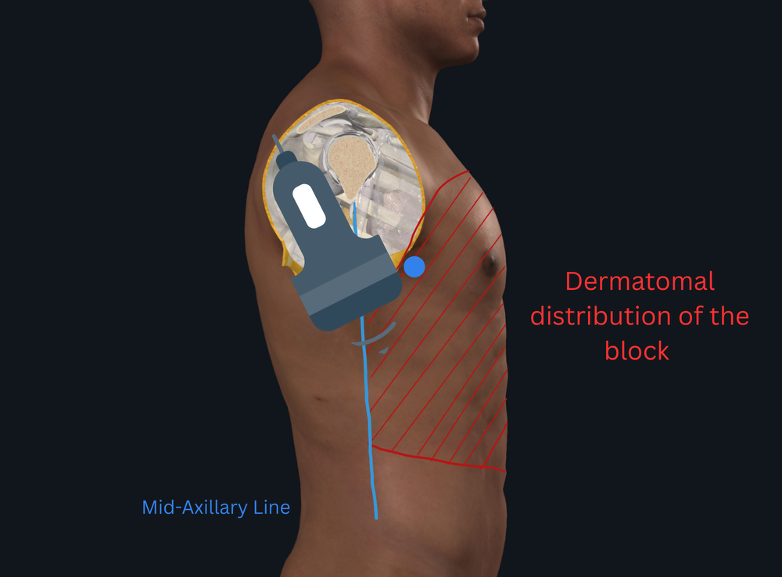
Figure 1 – Probe positioning and the dermatomes anesthetized
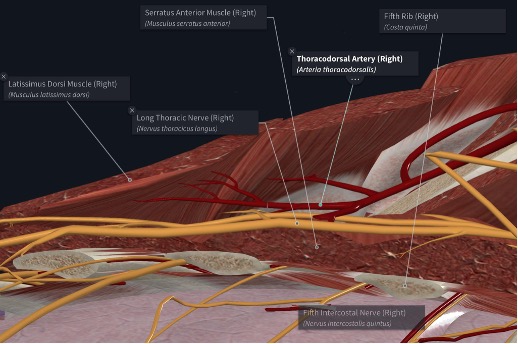
Figure 2 – Anatomy of the planar block including nerves and arteries in the space
Indications for a SAPB:2,5
- Anterolateral chest trauma:
- Rib fractures
- Burns
- Chest tube placement and pain
- Thoracotomies
- Pathology with significant pain such as herpes zoster
- Cardiothoracic surgery
- Breast surgery
There are multiple approaches to doing a SAPB, including injection superficial to, deep to, or on either side of the muscle for analgesia.6,7 Both superficial and deep approaches have been shown to be equally effective in terms of pain control as well as safety.8 This was further elucidated in a randomized control trial after thoracic surgery that found the safety profiles were similar between the two approaches but that the superficial approach had lower pain scores (p<0.001) and less opioid consumption (p=0.006) than the deep approach.9 The major benefits of SAPB are pain control and increased respiratory volumes. In a double-blinded randomized control trial of patients given a post-op SAPB, the nerve block group had a 25% reduction in opioid use (p<0.01).6 In an interventional study of 20 patients with rib fractures, patients were found to have an increase in mean vital capacity of 232 mL at 60 minutes post-block.10
Risks and Side Effects
Although SAPBs reduce opioid requirements, they are not without risks. SAPB puts patients at risk for damage to surrounding structures, bleeding, infection at the injection site, and Local Anesthetic Systemic Toxicity (LAST) syndrome.4
LAST syndrome can present with:11
- Tinnitus
- Perioral numbness
- Seizures
- Cardiac arrest
Patients are at increased risk if they are hypoxic, hypercarbic, or acidotic due to increased cellular trapping and concentration of anesthetic.11 The treatment for LAST is intravenous lipid emulsion therapy to increase sequestration of anesthetic.11,12
Prevention is best done by:
- Aspirating while advancing the needle
- Incrementally injecting the local anesthetic
- Keeping the patient on cardiac monitoring during and after the procedure
- Identifying risk factors that put patients at increased risk for developing LAST syndrome
When choosing which anesthetic to use, it is recommended to reference a trusted source of your choice, such as Safe Local or MDCalc to determine appropriate dosing. When doing a SAPB bilaterally, the dose will need to be split in half for each side in order to not exceed the safe dose of local anesthetic.7 Patients are also at risk for peripheral nerve injury; however this complication is rare and is managed by prevention.1
The benefits of increased pain control and enhanced respiratory function pose a strong argument for SAPB use. The American College of Emergency Physicians (ACEP) is in agreement and officially endorsed ED physicians to consider this treatment as part of their practice in 2021.13 This statement comes after a U.S National Trauma Data Bank report in 2019 showed that regional nerve blocks such as SAPB are underutilized and only used in approximately 3% of eligible patients.14 A 2024 Australian study found that the number needed to treat with SAPBs was just 5 patients with rib fractures to achieve both a 2-point or greater reduction in pain score and an absolute pain score of less than 4 out of 10.15 Given the strong professional endorsement, proven efficacy, and significant underutilization, SAPBs represent a high-value intervention that should be more widely integrated into emergency medicine practice.
Limitations
Some of the limitations to doing these blocks are level of experience and time. Despite the endorsement from ACEP, there is low implementation of nerve blocks in EDs due to inconsistent training availability and variable training rigor.1,16 Time is a constant limitation in the ED, and the setup and performance of procedures can be difficult to accommodate during a busy shift. One way to mitigate the time needed for the procedure is for facilities to create nerve block carts for easy and quick access to supplies.1 Finally, the SAPB is not a permanent solution and patients will require further interventions or medications after the anesthetic wears off. Even so, multiple studies demonstrate sustained benefits, with reduced pain scores and opioid requirements persisting beyond the block’s duration.6,15
Technique
Supplies:
- Ultrasound with the linear high-frequency probe (consider using the curvilinear for patients with greater body habitus)
- Sterile probe cover and gel
- Sterile gloves and drapes
- Chlorhexidine or a cleaning solution
- Blunt spinal needle (preferably an echogenic needle)
- Extension Tubing
- Normal saline flush
- Small gauge needle for skin wheel
- 25-30 cc of your anesthetic of choice (or normal saline to dilute anesthetic to appropriate volume)

Figure 3 – All the supplies required to perform the serratus anterior nerve block
-
- Place the patient in a supine position with the affected arm above the patient’s head. The patient should be placed on the monitor to watch for hemodynamic instability. Set up the area for a sterile procedure. Ensure that the patient has a functioning IV.
- Identify the fifth intercostal space at the midaxillary line.
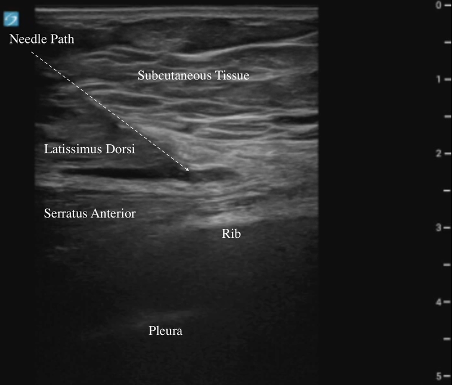
- Place the linear probe in the transverse plane of the serratus anterior muscle with the probe in the non-dominant hand and the needle in the dominant hand. The indicator should point towards the patient’s chest. Find the view below of the latissimus dorsi, serratus anterior, and the ribs.
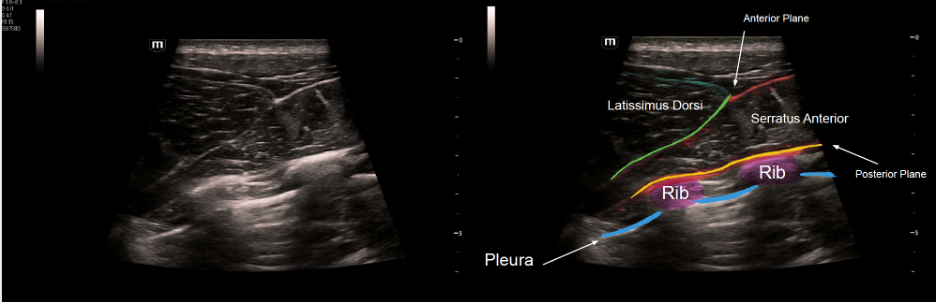 Figure 4 – Sonographic anatomy of the serratus anterior block
Figure 4 – Sonographic anatomy of the serratus anterior block - Once the desired view is obtained, mark the entry point and use the small gauge injection needle to make a wheel with an anesthetic for patient comfort.
- Place the blunt spinal needle connected to the flushed saline tubing to the patient’s skin at the anterior-most edge of the probe and puncture the skin. The ultrasound probe should be used in an in-plane approach until the fascial plane is accessed. It is important to ensure that air has been flushed out of the tubing as it can obscure your view if you inject air bubbles into the site.
- The anesthetic can be injected superficial to or deep to the serratus anterior muscle.2 Before injection of the anesthetic, hydrodissection should be performed with normal saline to ensure the needle tip is correctly located within the fascial plane. The correct location can be identified by the ellipsoid expansion of the fascial plane.
Video 1 – Expansion of the anterior plane as it is injected with saline for hydrodissection (provided by The Pocus Atlas) - Once injection of saline into the plane of choice is confirmed, exchange the flush for the syringe of anesthetic. Begin to inject slowly, and there should be no resistance to injection. You can also use a three-way stop cock to switch between the saline flush and anesthetic
Video 2/Figure 5 – Continued injection of anesthetic into the anterior plane with labeled anatomy on the right.- Place a bandage on the patient and label with the date and time of the block, the type of anesthetic, and the amount used.
Pearls
- Use the ribs as a target if attempting a deep SAPB to avoid accidentally causing an iatrogenic pneumothorax.
- Needle guidance along the curvature of the thorax may be difficult; consider rocking the probe to enhance visualization.
- Consider performing the block with two people: one to do the procedure and another to push normal saline and the anesthetic as needed. The second person can also be available to change settings on the ultrasound.
- Consider using color doppler before injection to visualize the thoracodorsal artery and avoid injury.
Pitfalls
- Ensure sterile technique to avoid increased infection risk.
- An echogenic needle is not necessary, but is recommended to increase needle visualization.
- Properly position and prepare the patient for the procedure to decrease the risk of sudden movements that could increase the risk of accidental iatrogenic pneumothorax.
Case Conclusion:
You utilized your knowledge of the SABP and injected 30cc of 0.25% bupivacaine, providing significant pain relief. The patient was discharged over four days with no development of pneumonia and with adequate pain control.
References:
- Malik A, Thom S, Haber B, et al. Regional Anesthesia in the Emergency Department: an Overview of Common Nerve Block Techniques and Recent Literature. Current Emergency and Hospital Medicine Reports. 2022;10(3):54-66.
- Xie C, Ran G, Chen D, Lu Y. A narrative review of ultrasound-guided serratus anterior plane block. Ann Palliat Med. 2021;10(1):700-706. doi:10.21037/apm-20-1542
- Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68(11). doi:10.1111/anae.12344
- Serra S, Santonastaso DP, Romano G, et al. Efficacy and safety of the serratus anterior plane block (SAP block) for pain management in patients with multiple rib fractures in the emergency department: a retrospective study. European Journal of Trauma and Emergency Surgery. 2024;50(6):3177-3188.
- Jack JM, McLellan E, Versyck B, Englesakis MF, Chin KJ. The role of serratus anterior plane and pectoral nerves blocks in cardiac surgery, thoracic surgery and trauma: a qualitative systematic review. Anaesthesia. 2020;75(10):1372-1385.
- Vandenbrande J, Jamaer B, Stessel B, et al. Serratus plane block versus standard of care for pain control after totally endoscopic aortic valve replacement: a double-blind, randomized controlled, superiority trial. Reg Anesth Pain Med. 2024;49(6):429-435. Published 2024 Jun 3. doi:10.1136/rapm-2023-104439
- Benesch T, Mantuani D, Nagdev A. Case Report: Bilateral Ultrasound-guided Serratus Anterior Plane Blocks for a Chest Wall Burn. Clin Pract Cases Emerg Med. 2021;5(1):117-120. doi:10.5811/cpcem.2020.12.50184
- Singh NP, Makkar JK, Dhawan I, Singh N, Singh PM, Siddiqui N. Relative Perioperative Analgesic Efficacy of Superficial Versus Deep Approach of Serratus Anterior Plane Block for Anterior Chest Wall Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Clin J Pain. 2024;40(12):726-733. Published 2024 Dec 1. doi:10.1097/AJP.0000000000001249
- Meng G, Chen W, Shi D, Mei B, Liu X. Superficial vs. deep serratus anterior plane block for analgesia in patients undergoing single-port video-assisted thoracoscopic surgery: A randomized prospective trial. J Clin Anesth. 2025;106:111950. doi:10.1016/j.jclinane.2025.111950
- Kring RM, Mackenzie DC, Wilson CN, Rappold JF, Strout TD, Croft PE. Ultrasound-Guided Serratus Anterior Plane Block (SAPB) Improves Pain Control in Patients With Rib Fractures. J Ultrasound Med. 2022;41(11):2695-2701. doi:10.1002/jum.15953
- Gitman M, Fettiplace MR, Weinberg GL, Neal JM, Barrington MJ. Local Anesthetic Systemic Toxicity: A Narrative Literature Review and Clinical Update on Prevention, Diagnosis, and Management. Plast Reconstr Surg. 2019;144(3):783-795. doi:10.1097/PRS.0000000000005989
- Sepulveda EA, Pak A. Lipid Emulsion Therapy. [Updated 2024 Feb 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549897/
- American College of Emergency Physicians. Ultrasound-Guided Nerve Blocks. ACEP; Approved April 2021. https://www.acep.org/…/ultrasound-guided-nerve-blocks.pdf. Accessed September 10, 2025.
- Cheema FA, Chao E, Buchsbaum J, et al. State of Rib Fracture Care: A NTDB Review of Analgesic Management and Surgical Stabilization. The American surgeon. 2019;85(5). Accessed August 22, 2025. https://pubmed.ncbi.nlm.nih.gov/31126359/
- Partyka C, Asha S, Berry M, et al. Serratus Anterior Plane Blocks for Early Rib Fracture Pain Management: The SABRE Randomized Clinical Trial. JAMA Surg. 2024;159(7):810-817.
- Walsh CD, Ma IWY, Eyre AJ, et al. Implementing ultrasound-guided nerve blocks in the emergency department: A low-cost, low-fidelity training approach. AEM Educ Train. 2023;7(5):e10912. Published 2023 Oct 8. doi:10.1002/aet2.10912




