
Author: McKenna Furgurson, MD (EM Resident Physician, Parkland / UT Southwestern) // Reviewed by: James Cao, MD; Alex Koyfman, MD (@EMHighAK); Brit Long, MD @long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 37-year-old female with history of alcohol and drug abuse is brought in via EMS after being found asleep on a bench on a cold winter morning. She is unresponsive. Vital signs are notable for HR 45, BP 85/40, SaO2 90%, rectal temperature 29°C. Naloxone is given with no improvement, and the patient is intubated. On exam she is unresponsive, pulses show irregular rhythm, and extremities are cool. EKG obtained on arrival to ED is below. POC glucose is 65. What is the likely diagnosis, and what is the first step in management?

Answer: Accidental/environmental hypothermia; consider alcohol intoxication, thiamine deficiency, hypoglycemia, drug overdose. First step: remove cold/wet clothes and begin rewarming.
Background: Defined by core body temperature <35°C [1]
- Classified as the following: Mild 32-35°C; Moderate 28-32°C; Severe <28°C; Profound <20°C
- Between 1999-2011, an average of 1301 deaths/year in the US were associated with exposure to natural cold [2].
- Death rates are higher in elderly and in nonmetropolitan counties.
- Elderly are more susceptible due to impaired thermoregulation with age [3].
Causes of Hypothermia:
- Environmental / accidental
- Metabolic: Hypoglycemia, DKA, hypothyroid, adrenal insufficiency, thiamine deficiency
- Toxicologic considerations [4]
- Beta-blockers, cholinergics, and hypoglycemics can impair thermogenesis
- Ethanol, opioids, benzodiazepines, CO poisoning can cause impaired shivering or impaired perception of cold
- Antipsychotics, ethanol, and alpha blocking agents cause impaired vasoconstriction
- Sepsis
- Malnutrition, homelessness
- Advanced age
Evaluation:
- Obtain temperature: Mild 32-35°C; Moderate 28-32°C; Severe <28°C; Profound <20°C
- If unable to obtain temperature with a thermometer, the Swiss hypothermia staging system is helpful for estimation [5]; however, signs and symptoms do not necessarily correlate well with the degree of hypothermia.
- Some generalized, common findings: [2,5]
- Mild (32-35°C): Conscious and shivering; cool, pale skin; often tachycardic.
- Moderate (28-32°C): +/- Shivering; amnesia, loss of fine motor skills, slurred speech. Bradycardia and arrhythmias may occur.
- Severe (<28°C): Unconscious, no shivering. May see extreme bradycardia, hypotension, apnea, fixed dilated pupils, and areflexia.
- Profound (<20°C): VS not obtainable.
- Obtain temperature using a thermometer that is able to reach low levels. Core temperature may vary based on body site, so monitoring at more than one site is preferred [1,6].
- Esophageal probe placed within the lower third of the esophagus is preferred as it correlates with temperature of the heart and is reliable with rapidly changing temperatures [7]. Use if patient is intubated. If probe is in upper esophagus, reading may be elevated due to inhaled warm air.
- Rectal probe: Place 15 cm deep. Temperatures may lag behind core body temperature during rewarming.
- Bladder probe: False readings if irrigating bladder or performing peritoneal lavage. It may also lag behind core body temperature during rewarming.
- Labs: POC glucose, CBC, CMP, Coagulation panel/fibrinogen (cold can precipitate DIC), lactate, TSH, cortisol, CK, blood cultures/infectious work up, tox workup if suspected. Of note, blood is often rewarmed in the lab and can lead to results that may appear normal but do no reflect the true patient status.
- EKG findings [3]:
- Initial tachycardia (to increase cardiac output).
- Develop bradycardia (there is decreased spontaneous depolarization of pacemaker cells which makes this bradycardia refractory to atropine).
- Prolonged PR and QT intervals, and classic “J wave” (Osborn wave) on EKG are due to repolarization abnormalities.
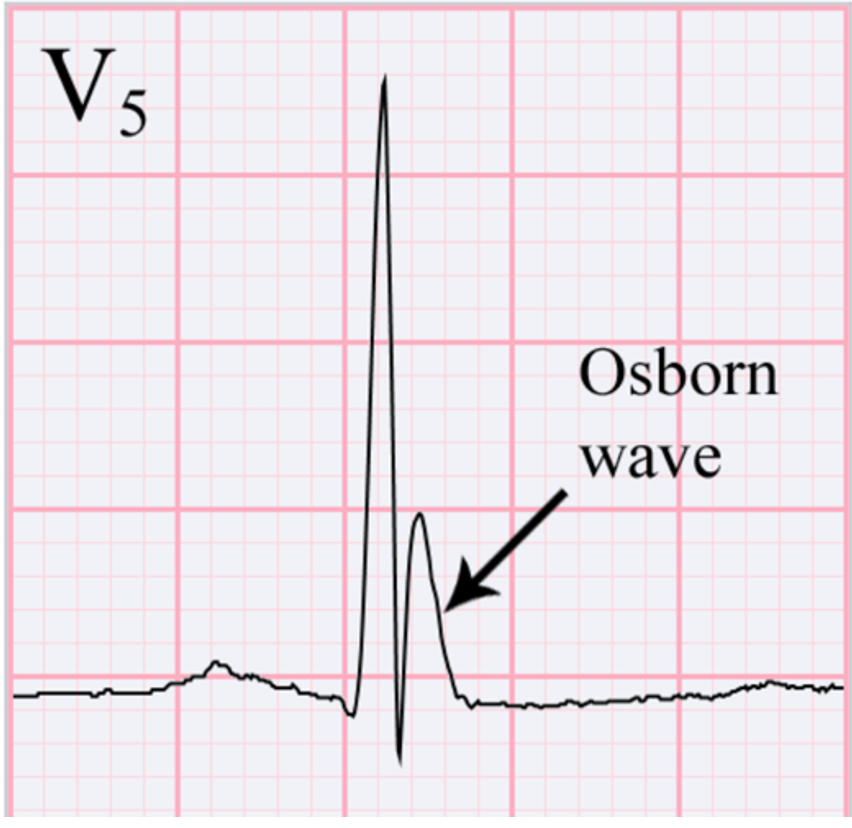
-
- Often see atrial fibrillation/flutter and ventricular dysrhythmias, which increase in those with temperature <32°C and are very common for <28°C.
- The heart is very irritable when cold, increasing risk of ventricular dysrhythmias. Take care when moving patient or performing procedures (such as central line- consider femoral vs IJ) to reduce ventricular dysrythymias.
Management: The Pulseless Patient
Cardiac arrest from hypothermia:
- Peripheral pulses may be unreliable due to vasoconstriction – check carefully for a pulse for 60 seconds and consider early arterial line placement.
- Do not do CPR if:
- ACLS
- Delayed or intermittent CPR can be adequate (if unable to perform continuous CPR, such as in the prehospital setting) due to decreased oxygen demand. For T<28°C, alternating 5 min CPR and <5 min without CPR is acceptable. For T<20°C, alternating 5 min CPR and <10 min without CPR is acceptable [8].
- Duration of CPR is not a predictor of outcome [5].
- AHA guidelines suggest continuing epinephrine according to standard ACLS algorithm.
- 2010 European Resuscitation Council guidelines suggest up to 3 defibrillation attempts and hold epinephrine until >30°C. Since medications may accumulate due to poor circulation/metabolizing, it is acceptable to double the interval time between epinephrine doses (ie, every 8 min instead of every 4 min) until >35°C [8,9].
- ECMO: Reserved for those with cardiac arrest, hemodynamic instability, completely frozen extremities, or no improvement with less invasive techniques. Rate of survival without neurologic impairment is 47-63% when patient are treated with ECMO or bypass, and 37% without [5]. More discussion on ECMO below.
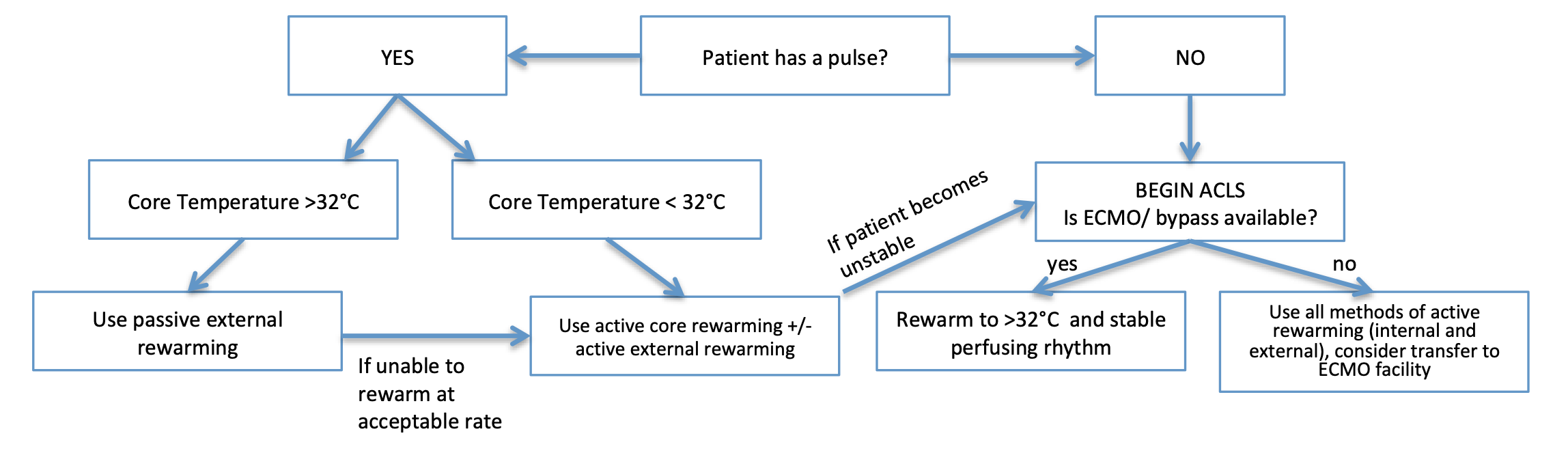
Management: Patient with a Pulse
Rewarming methods [6]
Passive external warming: Use for patients with mild hypothermia. Reduce heat loss by removing wet clothing and using blankets to allow patient’s intrinsic heat to rewarm self. Best for mild hypothermia.
- If not increasing by 0.5/hr then move to active rewarming.
- Elderly with poor metabolic/cardiovascular homeostasis may not have enough reserve.
Active external warming [6]: Use for moderate and severe hypothermia. Incorporates direct exposure of skin to exogenous heat source.
- Immersion, radiant heat, forced air, heating blankets.
- Possible concern for burn injuries, especially is patient is altered.
- Rewarm trunk before extremities due to possible “afterdrop” effect when the extremities vasodilate and release the cool blood back to core circulation.
- Avoid rewarming frostbitten extremities until core temp >34°C.
Active internal/core warming [1,5,7]: Use for severe and profound hypothermia.
- Fluids: IV fluids should be warmed to 38-42°C [5].
- Large volumes are often needed due to cold diuresis (vasoconstriction and decreased release of ADH), and due to vasodilation during rewarming (which may cause hypotension).
- Airway: Heated humidified air raises body temp by 1-2°C per hour. It is not as effective as peritoneal or pleural lavage, but it is quick to initiate, and may rewarm heart and decrease irritability/ risk of ventricular fibrillation [1].
- Bladder, pleural, and peritoneal lavage really only used if unable to get patient to an ECMO center or ECMO center is >6 hours away.
- Bladder lavage: Irrigation of warmed fluid (40-42°C) with 3-way foley.
- Peritoneal and pleural lavage are equally efficient at rewarming: about 6°C /hr [1].
- Peritoneal lavage: Use heated crystalloid: 10-20ml/kg.
- Pleural lavage: Two large thoracostomy tubes: One is superior anterior and the 2nd is inferior and posterior. Use heated (40-42°C) saline infused through anterior tube and drains posteriorly [1].
Extracorporeal rewarming: Hemodialysis, cardiopulmonary bypass, ECMO. Rewarms 4-10°C/hour.
- Indications [10]: Cardiac arrest, T <28°C, systolic blood pressure <90, life-threatening arrhythmia, completely frozen extremities, severe rhabdomyolysis with hyperkalemia, or no improvement with less invasive techniques.
- VA- ECMO is preferred method and is continued until patient has a stable cardiac rhythm and core temperature > 32°C [11].
- VA- ECMO has higher survival rates than other rewarming techniques [7]. It also has higher survival and more favorable neurological outcomes compared with CPR alone [5]. Of those who survive rewarming with bypass methods, most have minimal neurologic deficits and can even resume former lifestyles [12].
Disposition:
- Patients with mild hypothermia can be rewarmed and discharged after observation if able to stay in a warm environment (for example, do not discharge the patient back to the environment in which he/she became hypothermic). If there is any concern in disposition, the patient should be admitted.
- Patients with moderate to severe hypothermia who required active core rewarming or had hypothermic cardiac arrest with ROSC should be admitted to ICU.
Other Conditions/Complications:
- Consider sepsis, Wernicke disease, adrenal insufficiency, rhabdomyolysis, disseminated intravascular coagulation (DIC), decompensated hypothyroidism.
- Provide antibiotics if concerned for sepsis, thiamine for Wernicke Disease, hydrocortisone for adrenal insufficiency, IV fluids for rhabdomyolysis, IV T4 for decompensated hypothyroidism.
Pearls:
- Consider the broad differential for hypothermia if it is not an obvious environmental cold exposure.
- Continue with prolonged CPR, hypothermia is neuroprotective, and patients can have good outcomes despite long resuscitative measures.
- ECMO is the best method for rewarming – consider transfer to ECMO facility in prehospital setting and even afterwards if ECMO facility is within 6 hours away.

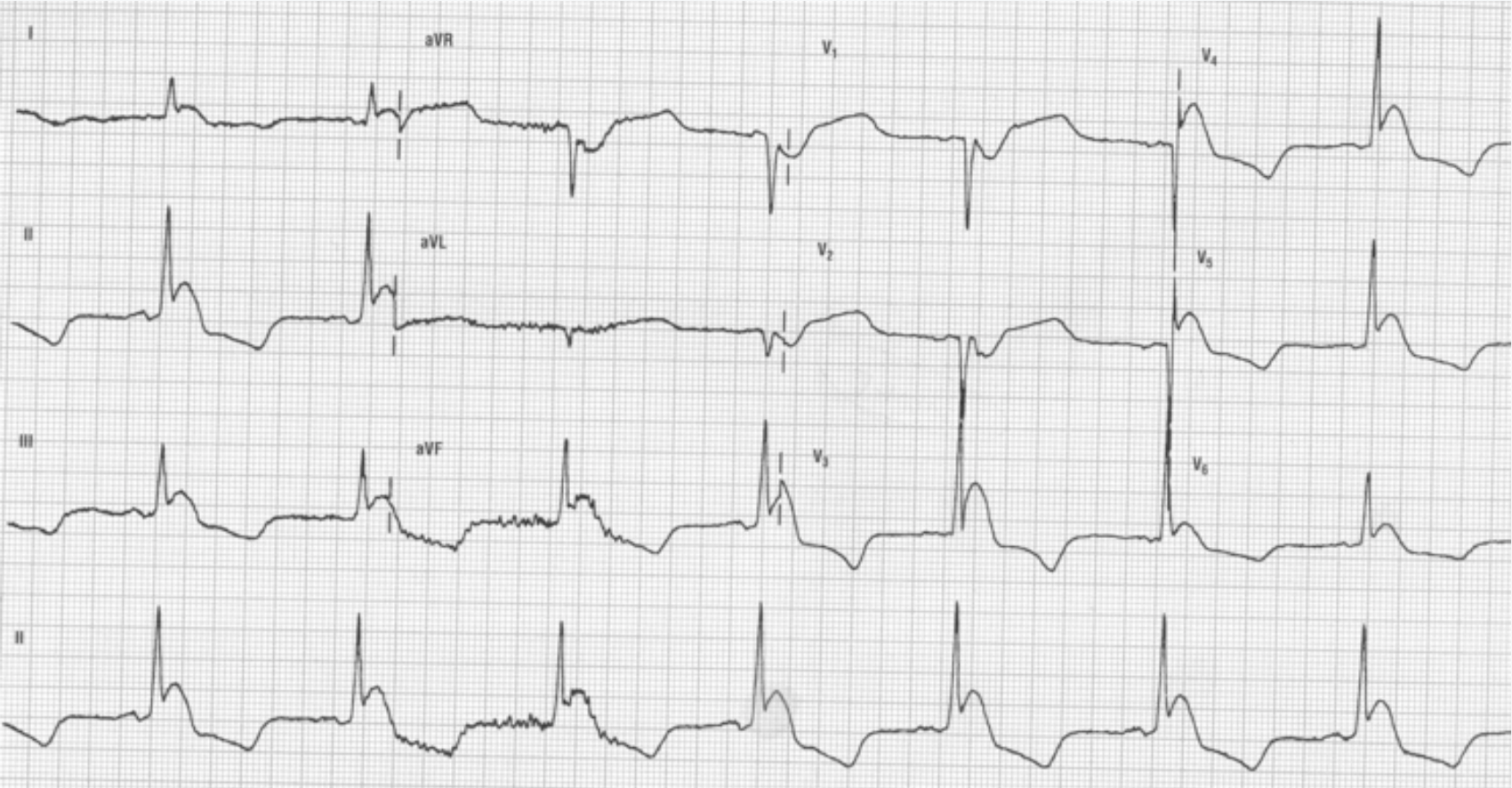
A 54 year-old-man is brought to the emergency department by emergency medical services after being found unresponsive in a local park. His ECG is shown above. Which of the following is the most likely cause of this patient’s presentation?
A) Digoxin toxicity
B) Hyperacute myocardial infarction
C) Hypothermia
D) Tricyclic antidepressant overdose
Answer: C
Hypothermia is defined as a core body temperature below 35°C. Osborn waves, also known as J waves, are an extra deflection at the end of the QRS complex due to elevation of the ST segment and are an ECG manifestation of moderate to severe hypothermia. J waves are best seen in the precordial leads of the ECG and become more prominent with increasing hypothermia. Other ECG manifestations of hypothermia include prolongation of the RR, PR, QRS, and QT intervals due to slowed electrical impulse conduction through cardiac potassium channels.

ECG manifestations of digoxin toxicity (A) include a “scooped out” depressed ST segment, premature ventricular beats, bradycardia, and bidirectional ventricular tachycardia. ECG evidence of a hyperacute myocardial infarction (B) includes peaked T waves and T wave inversions. ECG features of tricyclic antidepressant overdose (D) include marked widening of the QRS complex, tachycardia, and a positive R’ in lead aVR.
Further Reading:
FOAM Reading:
- WikEM “Hypothermia” https://wikem.org/wiki/Hypothermia#cite_note-3
- EM:Rap January 2014 “Hypothermia Part 1” and “Hypothermia Part 2”: https://www.emrap.org/episode/january2014/accidental
- REBELEM “Accidental Hypothermia” https://rebelem.com/accidental-hypothermia/
References:
- Otto R, Metzler M. Rewarming from experimental hypothermia: comparison of heated aerosol inhalation, peritoneal lavage, and pleural lavage. Crit Care Med. 1988;16(9):869-875.
- “QuickStats: Number of Hypothermia-Related Deaths, by Sex – National Vital Statistics System, United States, 1999–2011.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 4 Jan. 2013, www.cdc.gov/mmwr/preview/mmwrhtml/mm6151a6.htm.
- Mallet M. Pathophysiology of accidental hypothermia. QJM. 2002;95(12):775-785.
- Vassallo SU, Delaney KA. Thermoregulatory Principles. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds. Goldfrank’s Toxicologic Emergencies, 11e. McGraw-Hill
- Brown D, Brugger H, Boyd J, Paal P. Accidental Hypothermia. New England Journal of Medicine. 2012;367(20):1930-1938.
- Danzl D, Pozos R. Accidental Hypothermia. New England Journal of Medicine. 1994;331(26):1756-1760.
- Paal, P, Gordon L, Strapazzon G, Brodmann Maeder M, Putzer G, Walpoth B, Walpoth B, Wanscher M, Brown D, Holzer M, Broessner G, Brugger H. Accidental hypothermia–an update. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2016;24(1): 111.
- Gordon L, Paal P, Ellerton JA, Brugger H, Peek GJ, Zafren K. Delayed and intermittent CPR for severe accidental hypothermia. Resuscitation. 2015 May;90:46-9.
- Soar J, Perkins G, Abbas G et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution. Resuscitation. 2010;81(10):1400-1433.
- Dunne B, Christou E, Duff O, Merry C. Extracorporeal-Assisted Rewarming in the Management of Accidental Deep Hypothermic Cardiac Arrest. Heart, Lung and Circulation. 2014;23(11):1029-1035.
- Paal P, Brugger H, Strapazzon G. Accidental Hypothermia. Handbook of Clinical Neurology. 2018;157:547-563.
- Walpoth B, Walpoth-Aslan B, Mattle H, Radanov BP, Schroth G, Schaeffler L, Fischer AP, Segesser L, Althaus U. Outcome of Survivors of Accidental Deep Hypothermia and Circulatory Arrest Treated with Extracorporeal Blood Warming. Survey of Anesthesiology. 1998;42(4):199.





1 thought on “EM@3AM: Hypothermia”
Pingback: EM DOCS another useful site – Liverpool Emergency Department Simulation/Education