Introduction
Pulmonary arterial hypertension (PAH), defined by a mean pulmonary arterial pressure > 25 mmHg, is a progressive, incurable pulmonary disorder that historically was associated with a high rate of morbidity and mortality.1 Recent advancements in the therapeutic armamentarium of PAH has substantially improved survival rates and overall quality of life, but also carry considerable risks. PAH medications are classified as “high-risk medications” because critical safety issues exist with their narrow therapeutic index, complex dosing, unique devices for administration, and toxicity profile. If inappropriately managed, these agents can have toxicities or withdrawal phenomenon that can result in fatalities. As the likelihood of encountering PAH patients in the ED is increasing, it is important for ED providers to be well-versed on these pharmacologic agents and appropriate management in the ED setting to ensure a smooth and safe transition to the inpatient or outpatient setting. This post will serve to fill the gaps in knowledge of PAH medications and review key pearls for their safe and effective use in the ED.
*Disclaimer: Pulmonary hypertension is an umbrella term that encompasses five distinct disease states. Medications discussed in this post are only FDA-approved for WHO Group I, pulmonary arterial hypertension (exception of riociguat).2*
Therapeutic Targets for Pulmonary Arterial Hypertension

Prostacyclin Analogues
Mechanism of Action
In PAH, reduced activity of PGI2 synthetase decreases production of vasodilatory prostaglandins resulting in vasoconstriction, vascular proliferation, and platelet aggregation.3 Through direct stimulation of the PGI2 receptor, prostacyclin analogues elicit potent vasodilatory, antiproliferative, and antiplatelet effects.3

Drug Pearls for the ED
Parenteral Prostacyclins
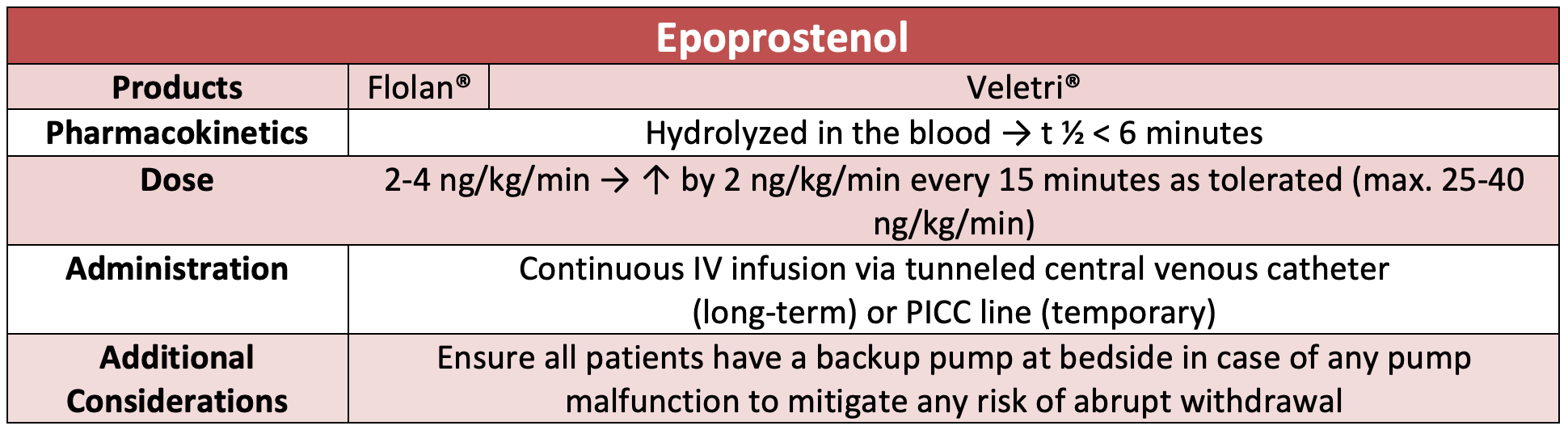
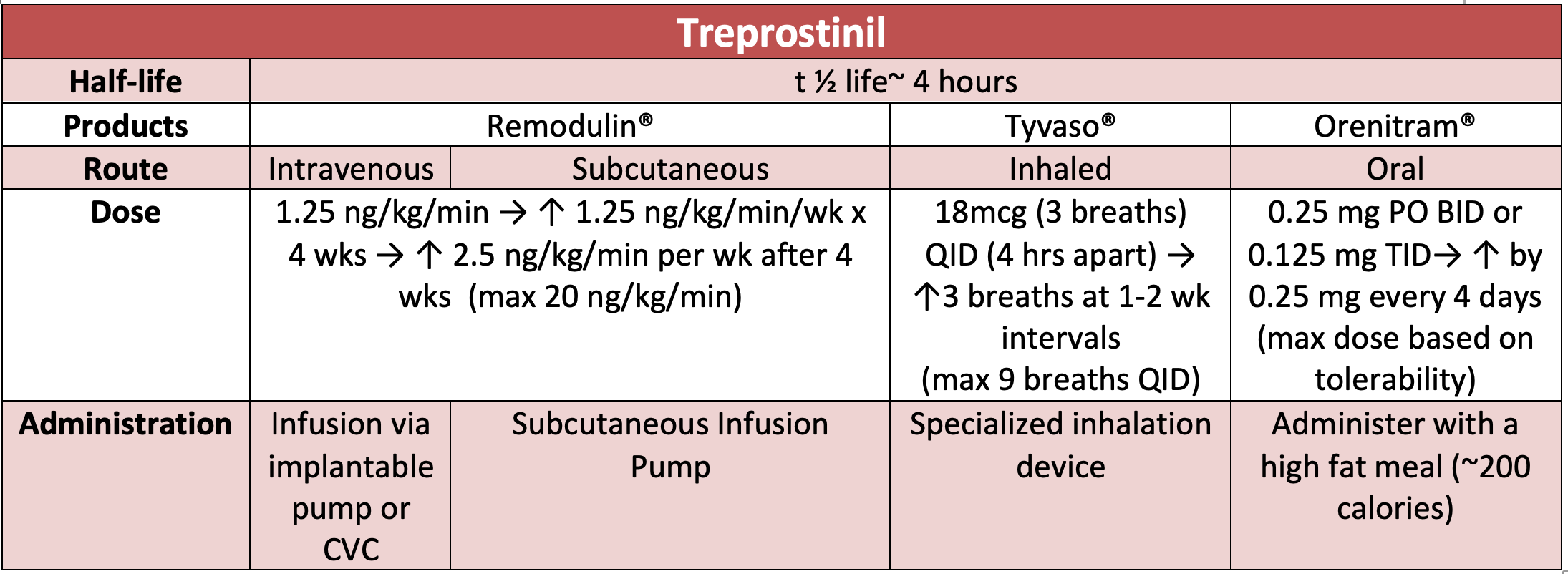
Prostacyclin analogues formulated for parenteral administration include epoprostenol (Veletri® or Flolan®) and treprostinil (Remodulin®). Intravenous prostacyclins require placement of a surgically inserted central catheter for administration as a continuous infusion through an ambulatory delivery system composed of a battery-operated pump and medication cassette in the outpatient setting.4-7 Epoprostenol is ultra-short acting and rapidly degraded by plasma esterases within ~6 minutes, allowing for ease of dose titrations to attain symptom control. However, abrupt discontinuation can result in subtherapeutic concentrations within minutes.4,5,7 Subsequently, patients are at risk of fatal rebound pulmonary hypertension and cardiorespiratory compromise.7 Although treprostinil has an extended half-life of ~4 hours, the risk of cardiorespiratory collapse upon abrupt discontinuation still exists, emphasizing importance for ED providers to ensure seamless continuation of prostacyclin therapies if appropriate upon ED arrival.6,7 Treprostinil is also formulated as a continuous subcutaneous infusion. This formulation is far less invasive and mitigates the complications associated with central catheter placement.6 However, subcutaneous absorption can be impaired in setting of high-dose vasopressors or fluid overload, and there is no standardized dosing conversion if switching to an IV therapy is warranted.
To ensure the medication administration is uninterrupted, routine assessment of the medication delivery system should be performed to confirm the pump is functioning and to ensure appropriate placement/patency of the central catheter. The line infusing the prostacyclin agent must be labeled clearly and no other medications should be concurrently infused through the same line to avoid inadvertent boluses or incompatibility issues.9 Some experts recommend placing two peripheral access sites upon arrival to avoid any lapses in treatment in the setting of inadvertent line obstruction, medication leakages or cartridge malfunctions.8,9 If urgent procedures or imaging is necessary, checking compatibility between home infusion pumps and magnetic resonance imaging (MRI) scanners is essential. In cases of incompatibility, extra tubing can be used in order to place the pump outside of the MRI room.8 ED clinicians should ensure that patients are continued on the patient’s home dose upon arrival and dose adjustments should only made under consultation with a PAH specialist.
Inhaled Prostacyclin Analogues
Inhaled prostacyclin analogues, iloprost and treprostinil, offer targeted drug delivery to the pulmonary vasculature and minimize systemic adverse effects.10, 11 Compatibility of the specialized inhalation devices for iloprost and treprostinil with mechanical ventilation have not been well established.8,12 Converting to continuous nebulization of epoprostenol (Flolan®) has the most supportive literature with mechanical ventilation or high-flow nasal cannula with aerosolized precautions. 8,12 Inhaled Veletri® has also been studied and shown to be non-inferior to Flolan® in patients requiring mechanical ventilation with ARDS.13However, given the technical challenges with aerosolized administration and risk of catastrophic consequences, it is important that staff with expertise are involved in the care of these patients.
Oral Prostacyclin Analogues
Oral treprostinil (Orenitram®) is an extended release tablet dosed 2-3 times daily.14 Each dose must be timed with a meal that contains at minimum of 250 calories and 30-50% fat in order to ensure adequate bioavailability.15 Since this formulation is rarely on formulary, providers may be faced with the need to switch to an alternate route of administration if a patient did not bring their home medication supply or has no enteral access. Dose conversions between oral and IV formulations are not standardized, and significant caution is advised given the high risk of medication errors.
Prostacyclin Analogues Adverse Effects
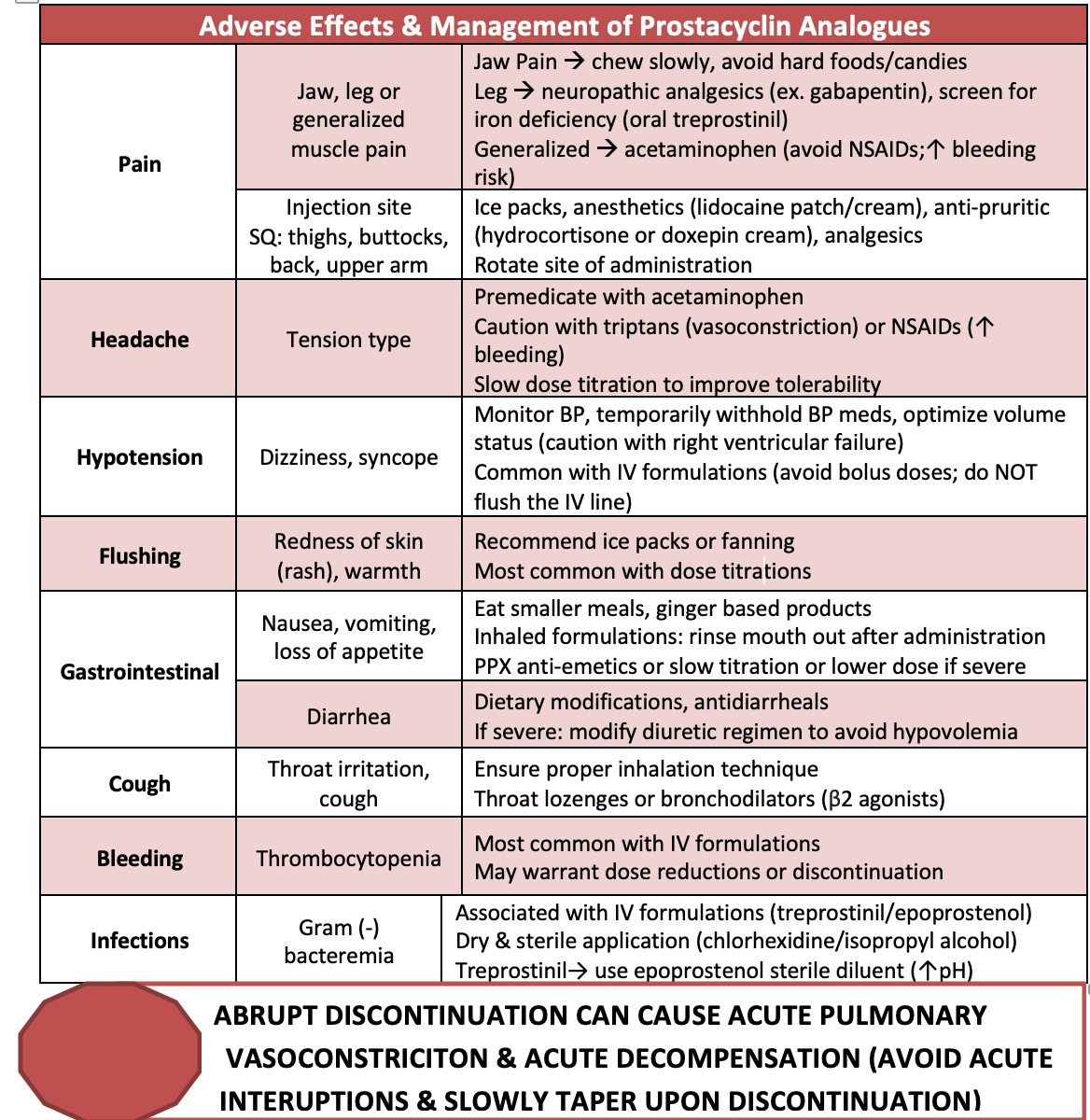
Owing to their vasodilatory properties, prostacyclin analogues can cause hypotension, flushing, peripheral edema and headache.7,8 Rapid titration carries the highest risk of hypotension, which can be profound in PAH patients with right ventricular heart failure.8,12 The off-target antiplatelet properties can increase the incidence of bleeding, though severe bleeding complications are rare.8 Permanent catheter placement for IV prostacyclins along with the unique formulation diluents predispose patients to increased infectious complications. Treprostinil is formulated in a diluent with a neutral pH which produces an environment conducive to bacterial overgrowth. Therefore, this formulation has been linked to a 2-fold increased risk of bacteremia.15 Interestingly, the microbiology of bacteremia differs between agents with gram positive skin microflora, Staphylococcus, Micrococcus commonly observed with IV epoprostenol compared to gram-negative infections including Pseudomonas and Enterobacter, with coagulase-negative Staphylococcus with IV treprostinil.15 If sepsis is the reason for hospital admission, ED providers should assess the medication catheter site as a possible source of infection and initiate broad-spectrum antibiotics for empiric coverage. Given the high infection risk, it is prudent to maintain sterility of the catheter site throughout ED interventions. If the catheter must be removed, switching to an alternative site of administration prior to removal is vital to minimize any lapse in medication exposure.7 Recall from previous paragraphs, it is of utmost importance to minimize any lapse in therapy and alternative infusion sites must established before removal of the infected catheter. Other common adverse effects and practical management strategies are outlined in the table below.
Prostacyclin Receptor Agonists
Selexipag (Uptravi®)
Mechanism of Action
Selexipag is a selective agonist of the prostacyclin receptor (IP-receptor) that induces potent vasodilation and relaxation of smooth muscle through increased cytosolic AMP and cytosolic calcium.16

Drug Pearls for the ED
Selexipag is available as an oral tablet dosed twice daily. The tablets should not be crushed or chewed and the drug should be held for patients that lose enteral access until more data regarding extemporaneous compounding is available.16 Unlike abrupt withdrawal with prostacyclin analogues, temporary interruptions of selexipag has not been shown to lead to acute deterioration, even up to 14 days following discontinuation.17 Of importance to ED providers, concurrent administration of selexipag with prostacyclin analogues should be avoided due to risk of exaggerated adverse effects ( i.e. muscular pain and flushing, to fatal hypotension). 16 Despite its selectivity to the IP-receptor, the proposed benefit in reducing “off-target” effects with selexipag has not been shown and this agent carries similar adverse effects to the prostacyclin analogues with the addition of hyperthyroidism that occurs secondary to its agonist on membrane-bound prostanoid receptors in the thyroid gland.18
![]()
Phosphodiesterase (PDE-5) Inhibitors
Mechanism of Action
In PAH PDE-5 is upregulated and accelerates NO degradation, thereby diminishing its vasodilatory effects. PDE-5 inhibitors (PDE-5i) restore NO production and pulmonary arterial relaxation.3

Drug Specifics
Tadalafil and sildenafil are the only PDE-5i FDA-approved for PAH.19,20 Tadalafil is available as an oral tablet that may be extemporaneously compounded into a solution to facilitate delivery via nasogastric tubes.20 Sildenafil is available as an IV or oral solution to allow for continued use in ventilated or non-ventilated patients. The IV form should be administered at 50% of the oral dose.19 Withholding a PDE-5i is preferred in the setting of hemodynamic instability as the risk of clinical deterioration in the acute setting is low.21 If continuation of PDE-5i is warranted, a switch to sildenafil may be favored because its shorter half-life and non-renal elimination reduces the risk of drug accumulation in critical illness.
An interaction that comes to the forefront of all ED providers minds is the classic interaction with nitrates and PDE-5i. There is a high propensity for this interaction to be overlooked given PDE-5i are often referred to by their brand names, “Viagra” or “Cialis”. Clinicians may refrain from inquiring about PDEi in females, given their more common use in men with benign prostatic hyperplasia and erectile dysfunction (ED). The potential consequences of this interaction are more dangerous in the PAH patient because the drugs are administered daily (instead of as needed) and individual doses are ~4-5 times higher for PAH than ED.22The American Heart Association (AHA) published a position statement to enhance provider awareness of this interaction. All patients with a history of PAH, males and females, should be screened for PDE-5i use. Clinicians should refer to these medications by using their brand and generic names to avoid confusion. A washout period of 24 hours for sildenafil and 36 hours for tadalafil prior to nitrate administration is required to mitigate this fatal interaction.19,20 In emergent situations of chest pain that require treatment, the use of a non-nitrate alternative such as a beta blocker or calcium channel blocker can be considered when appropriate.24
Endothelin Receptor Agonists
Mechanism of Action
Endothelin receptor antagonists (ERAs) reverse pulmonary vascular constriction and improve pulmonary vascular resistance through inhibition of ET-A or ET-B. Bosentan and macitentan are dual ETA/ETB receptor antagonists whereas ambrisentan has 4000-fold increased selectivity for ETA vs ETB.25,26,27

Drug Pearls for the ED
Bosentan undergoes extensive hepatic metabolism and is a potent inducer of two major CYP isoenzymes, CYP2C9 and CYP3A. These enzymes are involved in the metabolism of many therapeutic agents used in the ED setting, such as sedatives (ex. midazolam, fentanyl), antibiotics (macrolides, fluoroquinolones), or anticoagulants (ex. warfarin), necessitating dose adjustments to achieve the same therapeutic response.25 On the contrary, ambrisentan and macitentan are hepatically metabolized to a lesser extent and have fewer drug-drug interactions. 8,25 If a patient has a positive pregnancy test and is on these medications, the ED clinician should be aware that all ERAs are pregnancy category X due to the risk of embryo-fetal toxicity that require restricted distribution. 25 Due to the teratogenic risk and inclusion on the NIOSH hazardous medication list, female health care providers must take precautions when dispensing or administering ERAs by wearing gloves and avoid crushing the tablets.9
Bosentan can cause a dose dependent, reversible hepatotoxicity in up to 10% of patients owing to its inhibition of canalicular bile salt transport.28 In the presence of shock liver or acute hepatic decompensation, ERAs should be permanently discontinued.9 Other unique toxicities associated with ERAs is anemia with reductions in hemoglobin by at least 1 g/dL is expected within the first 4-6 weeks of treatment with an ERA, though is rarely life-threatening.24-26 Lower extremity edema occurs secondary to inhibition of ETA receptors which modulates salt and water retention. Exacerbations of acutely decompensated heart failure severe enough to warrant hospitalization has been reported to occur within the first 4 to 8 weeks of ERA initiation. 25,26,27 Ambrisentan carries the highest risk whereas macitentan causes minimal fluid retention and may be an ideal alternative when this complicates treatment.
![]()
Riociguat
Mechanism of Action
Riociguat (Adempas®) acts as a direct stimulator of soluble gunaylyl cyclase which mediates vasodilation through production of free nitric oxide. Riociguat is the only agent that has been approved for Chronic Thromboembolic Pulmonary Hypertension (CTEPH).28

Drug Pearls for the ED
Riociguat works directly on the nitric oxide pathway along with PDE-5i therefore there is a fatal risk of hypotension if co-administered with nitroglycerin, and other nitrate derivatives.29 Continuation of this therapy in the hospital setting is complicated by the exorbitant cost and relatively rare use that limits approval on hospital formularies. Continuation of a patient’s home supply or transition to an alternative vasodilator such as sildenafil or tadalafil should be made under the discretion of a PAH specialist. If a PDE-5 is considered as an alternative, a washout period of 24 hours is required to minimize the risk of fatal hypotension. Use of riociguat in critically ill patients who are NPO or have impaired gastric absorption is limited because it is not recommended to crush for enteral tube administration due to the teratogenic potential. Similar to ERAs, riociguat is also listed under a restricted distribution program due to its teratogenic risks and carries the same contraceptive and monitoring requirements mentioned with the ERAs.29
Summary Pearls
- DO consult your PAH specialists early to facilitate safe medication use.
- DO ensure you place two peripheral IVs for patients on IV prostacyclins.
- DO use generic and brand names when conducting a medication history.
- DO perform a thorough physical exam of the catheter line to ensure IV prostacyclin is patent.
- DON’T abruptly discontinue prostacyclin analogues.
- DON’T administer PDE-5 inhibitors or riociguat with nitrates (washout period required).
- DON’T administer ERAs, riociguat, and selexipag during pregnancy (all agents are teratogenic).
- DON’T ever adjust the dose of a PAH medication without consultation with a PAH specialist.
References/Further Reading:
- Hoeper MM, Kramer T, Pan Z, et al. Mortality in pulmonary arterial hypertension: prediction by the 2015 European pulmonary hypertension guidelines risk stratification model. Eur Respir J. 2017;50(2).
- Klinger JR, Elliott CG, Levine DJ, et al. Therapy for Pulmonary Arterial Hypertension in Adults: Update of the CHEST Guideline and Expert Panel Report. Chest. 2019;155(3):565-586.
- Lan NSH, Massam BD, Kulkarni SS, Lang CC. Pulmonary Arterial Hypertension: Pathophysiology and Treatment. Diseases. 2018;6(2)
- Veletri (epoprostenol) [prescribing information]. South San Francisco, CA: Actelion Pharmaceuticals US Inc; July 2017.
- Flolan (epoprostenol) [product monograph]. Mississauga, Ontario, Canada: GlaxoSmithKline Inc; February 2019.
- Remodulin (treprostinil) [prescribing information]. Research Triangle Park, NC: United Therapeutics Corp; July 2018.
- Coons JC, Clarke M, Wanek MR, Bauer A, Bream-rouwenhorst HR. Safe and effective use of prostacyclins to treat pulmonary arterial hypertension. Am J Health Syst Pharm. 2013;70(19):1716-23
- Torbic H. Management of Pulmonary Arterial Hypertension in the ICU. J Pharm Pract. 2019;32(3):303-313.
- Kingman MS, Chin K. Safety recommendations for administering intravenous prostacyclins in the hospital. Crit Care Nurse. 2013;33(5):32-9.
- Ventavis (iloprost) [prescribing information]. South San Francisco, CA: Actelion Pharmaceuticals US, Inc; October 2017.
- Tyvaso (treprostinil) [prescribing information]. Research Triangle Park, NC: United Therapeutics Corp; October 2017.
- Muzevich KM, Chohan H, Grinnan DC. Management of pulmonary vasodilator therapy in patients with pulmonary arterial hypertension during critical illness. Crit Care. 2014;18(5):523.
- Hawn JM, Bauer SR, Wanek MR, et al. Effectiveness, Safety, and Economic Comparison of Inhaled Epoprostenol Brands, Flolan and Veletri, in Acute Respiratory Distress Syndrome. Ann Pharmacother. 2019; 1060028019888853.
- Orenitram (treprostinil) [prescribing information]. Research Triangle Park, NC: United Therapeutics Corp; October 2019.
- Bloodstream infections among patients treated with intravenous epoprostenol or intravenous treprostinil for pulmonary arterial hypertension–seven sites, United States, 2003-2006. MMWR Morb Mortal Wkly Rep. 2007;56(8):170-2.
- Uptravi (selexipag) [prescribing information]. South San Francisco, CA: Actelion Pharmaceuticals US Inc; September 2019.
- Preston IR, Channick RN, Chin K, et al. Temporary treatment interruptions with oral selexipag in pulmonary arterial hypertension: Insights from the Prostacyclin (PGI) Receptor Agonist in Pulmonary Arterial Hypertension (GRIPHON) study. J Heart Lung Transplant. 2018;37(3):401-408.
- Coghlan JG, Picken C, Clapp LH. Selexipag in the management of pulmonary arterial hypertension: an update. Drug Healthc Patient Saf. 2019;11:55-64.
- Revatio (sildenafil citrate) [prescribing information]. New York, NY: Pfizer Labs; January 2019.
- Adcirca (tadalafil) [prescribing information]. Indianapolis, IN: Eli Lilly and Company; May 2017.
- Buckley MS, Staib RL, Wicks LM, Feldman JP. Phosphodiesterase-5 inhibitors in management of pulmonary hypertension: safety, tolerability, and efficacy. Drug Healthc Patient Saf. 2010;2:151-61.Bishop BM, Mauro VF, Khouri SJ. Practical considerations for the pharmacotherapy of pulmonary arterial hypertension. Pharmacotherapy. 2012;32(9):838-55.
- Cheitlin MD, Hutter AM Jr, Brindis RG et al. Use of sildenafil (Viagra) in patients with cardiovascular disease. Technology and Practice Executive Committee. Circulation 1999;99(1):168-77.
- Rosen RC, Jackson G, Kostis JB. Erectile dysfunction and cardiac disease: recommendations of the Second Princeton Conference. Curr Urol Rep. 2006;7(6):490-6.
- Tracleer (bosentan) [prescribing information]. South San Francisco, CA: Actelion Pharmaceuticals; April 2019.
- Volibris (ambrisentan) [product monograph]. Mississauga, Ontario, Canada: GlaxoSmithKline Inc; September 2018.
- Opsumit (macitentan) [product monograph]. Toronto, Ontario, Canada: Janssen Inc; August 2019.
- Fattinger K, Funk C, Pantze M, et al. The endothelin antagonist bosentan inhibits the canalicular bile salt export pump: a potential mechanism for hepatic adverse reactions. Clin Pharmacol Ther. 2001;69(4):223-31.
- Adempas (riociguat) [prescribing information]. Whippany, NJ: Bayer HealthCare Pharmaceuticals Inc; January 2018.




