
Author: Vivek Medepalli, MD (EM Resident Physician, UTSW / Parkland Memorial Hospital) // Reviewed by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX), Colin Danko, MD (EM Attending Physician, UTSW / Parkland Memorial Hospital) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 63-year-old male presents to the ED complaining of sudden onset shortness of breath for the past 2 hours. He has a history of CAD, HTN, and T2DM He states that he has been compliant with his medications. BP 97/68, HR 108, RR 21, 92% RA. Physical exam is notable for a holosystolic murmur most prominent over the apex and radiating to the axilla, mild bibasilar rales, JVD, and 2+ lower extremity pitting edema.
What is the most likely cause of this patient’s symptoms, and what are the next steps in management?
Answer: Mitral Regurgitation
Epidemiology:
- Primary mitral regurgitation secondary to valvular disease occurs in 1.5-3% of the population [1,2]
- Most commonly due to mitral valve prolapse in developed countries and rheumatic heart disease in developing countries [3]
- Prevalence of mitral regurgitation during cardiac catheterization in the setting of acute MI is 9-13% [4]
- Moderate-to-severe regurgitation in 3-4% of acute MI patients
- Mitral regurgitation seen in 38% of patients with dilated cardiomyopathy
- More common in males
Etiology:
- Primary Mitral Regurgitation [3,5]
- Degenerative mitral valve disease (ex. Mitral valve prolapse)
- Rheumatic heart disease
- Endocarditis
- Trauma
- Congenital malformations
- Drug-related valvular disease (ex. Cabergoline, bromocriptine)
- Secondary Mitral Regurgitation [3,5]
- Coronary artery disease
- Acute myocardial infarction (ruptured papillary muscle)
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
Pathophysiology:
- Acute Mitral Regurgitation: Commonly seen with acute MI, chordae tendinae rupture, endocarditis, and trauma[2,5]
- Regurgitant flow through diseased mitral valve leads to systolic backflow into the left atrium
- Subsequent backflow into the pulmonary circulation leads to pulmonary edema and sudden-onset shortness of breath
- Pulmonary hypertension leads to backflow into venous circuit, resulting in JVD, hepatomegaly, peripheral edema
- Decreased filling of left ventricle leads to decreased forward flow, resulting in hypotension and cardiogenic shock
- Chronic Mitral Regurgitation: [2,5]
- Changes occur more slowly, leading to eccentric hypertrophy and dilation of the left atrium
- Chronic left atrial dilation can lead to atrial fibrillation
Clinical Features:
- Acute Mitral Regurgitation: [6]
- Sudden-onset pulmonary edema and hypotension
- Cardiogenic shock
- Physical exam will show pulmonary rales, peripheral edema, JVD, hepatomegaly, S3, hyperdynamic cardiac apex
- Classic murmur described as holosystolic, most prominent over the cardiac apex, and radiating to the axilla
- Only present in 50% of cases; however, absence of murmur does not exclude acute mitral regurgitation [2,7]
- Classic murmur described as holosystolic, most prominent over the cardiac apex, and radiating to the axilla
- Chronic Mitral Regurgitation
- Majority of patients have mild regurgitation at baseline, which is often asymptomatic or associated with mild dyspnea [7]
- Some patients with mild symptoms at rest can have profound acute regurgitation with exercise, resulting in acute pulmonary edema [3,8]
Evaluation:
- Transthoracic Echocardiogram:
- Recommended to evaluate the presence, etiology, severity, and further hemodynamic consequences of the regurgitation [3,10]
- Often shows an elevated ejection fraction (>60%) due to forward flow into the systemic circulationcombined with backflow into the left atrium [10]
- Since regurgitant lesions tend to overestimate LV function, the absence of hyperdynamic function is concerning for impaired function
- Color doppler shows backward flow into the left atrium
- Consider transesophageal echocardiogram in patients with inconclusive transthoracic echocardiogram
- Recommended to evaluate the presence, etiology, severity, and further hemodynamic consequences of the regurgitation [3,10]

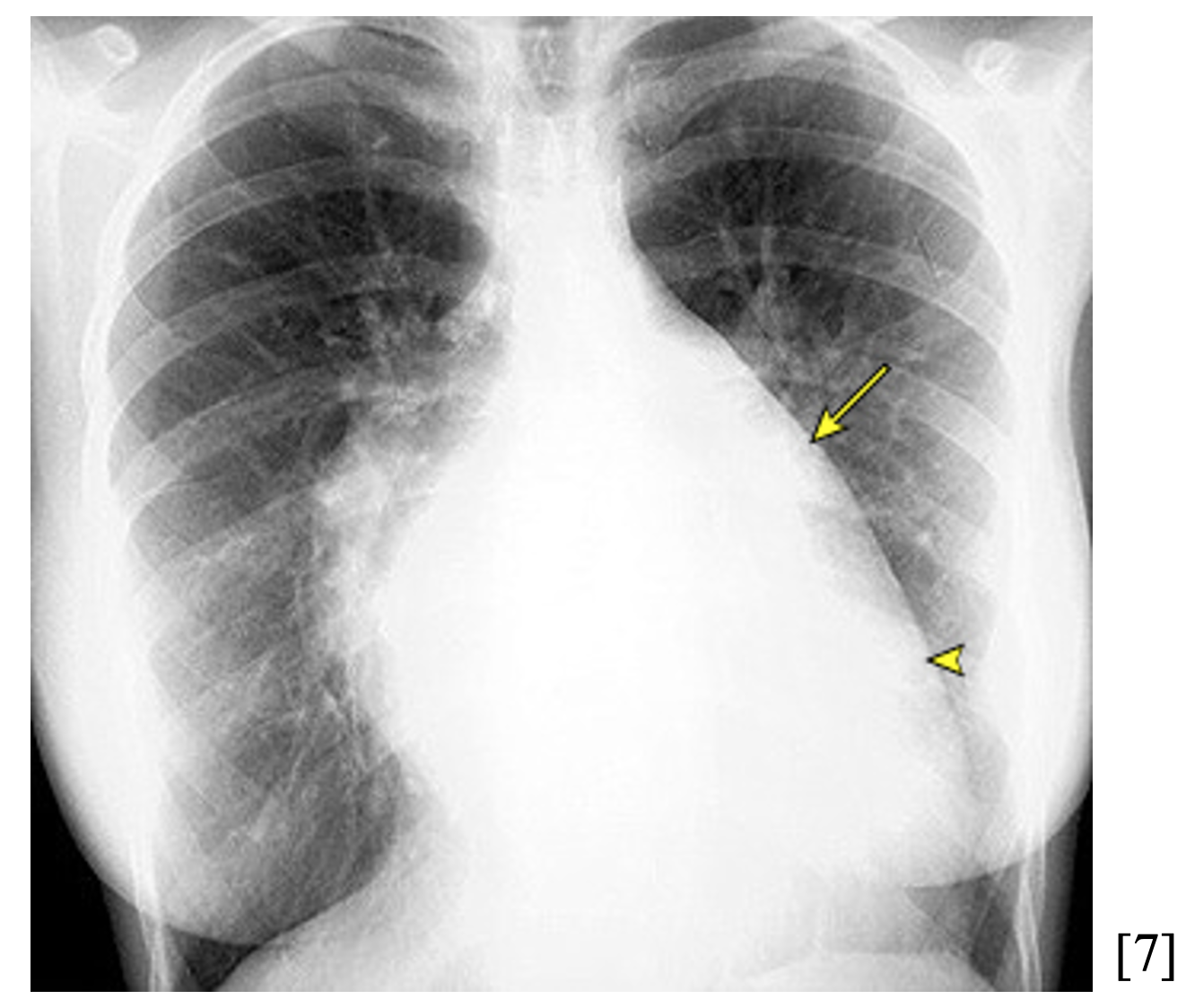
- Chest X-Ray
- May show cardiomegaly, enlarged left atrium, or pulmonary edema in symptomatic patients [2, 6]
- EKG
- Will not show changes strictly due to mitral regurgitation acutely, but may reveal underlying cardiac ischemic event as source of symptoms
- May reveal left atrial enlargement (biphasic P waves) or left ventricular hypertrophy in the setting of chronic mitral regurgitation [6]
- Supplemental laboratory evaluation: tailor to patient’s clinical presentation
- Troponins if ACS is suspected
- Blood cultures if the patient has clinical signs of endocarditis
- Pro-BNP is often elevated and nonspecific
Treatment:
- Severe acute mitral regurgitation typically requires emergent surgical valve repair or replacement [6]
- Volume overload and hypertension worsen regurgitation
- Patients are afterload sensitive; the goal blood pressure is the lowest value that provides organ perfusion
- Volume overload but perfusing
- Decreasing afterload reduces regurgitant flow and increases cardiac output
- Utilize dihydropyridine calcium channel blockers such as nicardipine or clevipidine; nitroglycerin may also be used
- Preload reduction assists with gas exchange and cardiac function
- Utilize nitroglycerin infusion with titration
- Noninvasive positive pressure ventilation (NIPPV) and diuretics may be used
- Target slightly higher heart rates, as slow heart rates increase regurgitant flow
- Decreasing afterload reduces regurgitant flow and increases cardiac output
- Volume overload but poor perfusion
- Provide inotropic support while maintaining mean arterial pressure
- Start epinephrine infusion, or use dobutamine (be ready with norepinephrine)
- Milrinone can be used in the ICU
- Preload reduction
- Use NIPPV
- HR control; avoid bradycardia and severe tachycardia
- If significantly tachycardic, use amiodarone or even IV digoxin
- Provide inotropic support while maintaining mean arterial pressure
- Emergent consultation recommended to interventional cardiology and cardiothoracic surgery
- Mechanical circulatory support may be used as a bridge to surgery
- In the setting of ACS, prompt revascularization therapy is indicated
- May be sufficient to reverse acute mitral regurgitation not caused by chordae tendinae or papillary muscle rupture [6]
- If patient has clinical signs of endocarditis, start broad spectrum antibiotic therapy
Consultation:
- Cardiology/Interventional Cardiology
- Cardiothoracic Surgery
Disposition:
- Mild-to-moderate symptomatic mitral regurgitation with hemodynamic stability can be admitted to floor/ward with telemetry capabilities [6]
- Severe mitral regurgitation may require ICU admission and/or emergent surgical repair
Summary and Pearls:
- The most common cause of primary mitral regurgitation is prior structural valve disease (ex. Mitral valve prolapse) and secondary mitral regurgitation is ischemic heart disease
- Acute mitral regurgitation presents with sudden onset dyspnea, JVD, peripheral edema
- The diagnostic modality of choice is transthoracic echocardiogram (TTE); EKG and laboratory markers can provide supplementary information to reveal etiology
- Mild to moderate mitral regurgitation can be managed with symptomatic medical therapy, while severe valve disease requires ICU admission and possible emergent surgical valve repair or replacement




