
Authors: Reka Zsilinszka, MD (EM Resident Physician, Hospital of the University of Pennsylvania) and Kevin R. Scott MD, MSEd (EM Attending Physician, Hospital of the University of Pennsylvania) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 45-year-old male with a history of renal failure is brought in by EMS with tachycardia and altered mental status. His vital signs include BP 90/40, HR of 150, RR 20, T 97, SpO2 99% on 2L. On exam, he is responding to questions but appears uncomfortable and diaphoretic. A 12-lead ECG shows a regular wide-complex tachycardia. He reports that he has been feeling intermittent palpitations for the last 2 days. What is your next step?
Background
Out of hospital cardiac arrest leads to approximately 300,000 deaths per year. The most common rhythms associated with sudden cardiac death are ventricular fibrillation and ventricular tachycardia (McNally et al., 2011). Ventricular tachycardia (VT) is defined as a rhythm greater than 120 beats per minute that arises distal to the bundle of His, including the ventricular/distal conduction system or the ventricular myocardium. VT can further be classified as sustained (>30 seconds) or non-sustained (<30 seconds), and monomorphic or polymorphic. Risk factors for VT include ischemic heart disease, structural heart disease, acquired and inherited channelopathies, electrolyte imbalance, infiltrative cardiomyopathy, as well as electrophysiological anatomic abnormalities and pro-arrhythmic drugs (Myerburg et al., 1992). Monomorphic VT is characterized by consecutive uniform and consistent QRS morphology. Classically, the ACLS teaching of ventricular tachycardia diverges based on the clinical decision of “stable” or “unstable”, but in the clinical setting, this differentiation can often be less clear.
In a patient that arrives in cardiac arrest with pulseless VT, compressions should be started immediately. While compressions are ongoing, rapid IV or IO access should be obtained, defibrillator pads should be applied, and the patient should be attached to the monitor. Patients should immediately be treated with defibrillation. Other interventions in the setting of pulseless VT include establishing an airway and administering medications such as epinephrine (1mg IV/IO every 3-5 minutes), and amiodarone (300mg IV/IO followed by second dose of 150mg IV/IO). Digging for an underlying cause based on history and presentation is important as time permits in an emergent situation.
For a patient who arrives with VT with pulses, the approaches to management are more nuanced, and outside the scope of this post. For more on the management of stable VT, see this prior emDocs post. In general, however, for patients with VT in the ED setting with suspected poor or unknown left ventricular ejection fraction (LVEF), amiodarone (3-5mg/kg IV over minutes) or lidocaine (1-1.5 mg/kg IV bolus, up to 3mg/kg max and followed by an infusion) is the preferred first choice. In patients with known intact LVEF, procainamide (30-50 mg/min IV up to a total of 18 mg/kg) can be used as a second-line agent (Ortiz et al., 2017). Additionally, if the ECG shows no irregular rhythm and the rate is less than 250 beats per minute, a dual “therapeutic and diagnostic” trial of adenosine (6-18mg IV push) can be given to differentiate between some of the possible mimics of VT, such as SVT with aberrancy (Marx & Rosen, 2014). If in doubt, however, synchronized cardioversion in the setting of light sedation should be performed. Sedation options in clinically unstable patients include etomidate (0.1mg/kg IV) or fentanyl (1mcg/kg/dose) (Wood & Ferguson, 2006). Benzodiazepines (midazolam 1-5mg IV) are also an option but will drop blood pressure and have a long duration of action (Morgenstern, 2015).
VT is an important cause of wide complex tachycardia. In all patients presenting with wide complex tachycardia, emergency physicians should consider mimics of VT as a part of the evaluation with the caveat, however, that differentiating between the causes of a wide complex tachycardia can be difficult in a time-sensitive situation. This review will focus on identifying and treating several VT mimics, but if there is any doubt or the patient is unstable, treat as if the cause were unstable VT and revert to electricity!
Supraventricular Tachycardia with Aberrancy
Any supraventricular tachycardia (SVT), such as atrial flutter, sinus tachycardia, AV nodal re-entry tachycardia (AVNRT), or AV re-entry tachycardia (AVRT) with aberrancy, is probably the most difficult confounder of a monomorphic ventricular tachycardia when interpreting the ECG of a regular wide-complex tachycardia. SVT episodes can occur in any individual, but risk factors include excessive caffeine/alcohol use, illicit drug use, psychological stress, hyperthyroidism, electrolyte abnormalities, structural/ischemic/congenital cardiac abnormalities, and medication reactions. AVNRT and AVRT often occur in younger healthy individuals (Page et al., 2016).
A number of rules exist for differentiating between true VT versus another underlying rhythm, but the distinction often remains difficult (Dr. Smith’s, Life in the Fast Lane). However, all of these confounders can be treated with cardioversion. If the rhythm is regular, a trial of adenosine (6mg IV push up to 18mg IV push) may help differentiate between an underlying supraventricular rhythm in patients with known underlying SVT and aberrancy who have previously been treated with adenosine. Aberrancy refers to the presence of a bundle branch block causing a widened QRS complex. Rapid atrial rhythms such as SVT or atrial flutter with 1:1 conduction can often cause a rapid (>200 bpm) regular rhythm with wide complexes that can look exactly like a VT on first glance (Figure 3).
A handful of findings can point the provider to a diagnosis of VT over SVT with aberrancy. First, a history of heart disease such as prior myocardial infarction or heart failure raise the probability of VT. The finding of Q-waves on prior ECGs signaling a history of ischemia also make VT the more likely underlying rhythm. Additionally, a number of ECG findings can also raise the likelihood that the presenting rhythm of VT. Absence of RBBB or LBBB morphology and extreme axis deviation with broad QRS complexes > 160 ms are suggestive of VT. Atrioventricular dissociation is one of those findings, which occurs when P-waves and QRS complexes are functioning at different rates, signaling that sinus rhythm is occurring independently of the ventricular rhythm (Figure 4). Another ECG finding suggestive of VT is capture and fusion beats, which is caused by intermittent AV conduction via the normal conduction pathways; such supraventricular impulses can actually trigger depolarization and show a QRS complex. If this QRS complex occurs early and appears narrow, then this is called a capture beat. If the supraventricular impulse conducts to the ventricles and joins with a ventricular beat from the ventricular focus, the result is a fusion beat (Figure 5) (Brady et al., 2017). On the other hand, SVT with aberrancy is more likely if prior ECG demonstrates a bundle branch block pattern similar to the broad complex tachycardia present, if a prior ECG shows evidence of WPW, and if prior tachycardias have been treated successfully with vagal maneuvers or adenosine.
These findings are difficult to remember in time-sensitive situations, so remember: when in doubt, electricity (synchronized cardioversion) is your friend and treat as if the rhythm were VT!
One last consideration with regards to SVTs with aberrancy is that atrial fibrillation can cause a similar appearance, but the rhythm will be irregular. Treatment considerations remain the same with the addition of rate control with beta-blockers or calcium channel blockers if the underlying rhythm is known to be a-fib and there is no concern for WPW.
Examples:

Figure 3 (Life in the Fast Lane): AVNRT with LBBB; image withLBBB morphology, no capture/fusion beats or AV dissociation seen.

Figure 4 (Life in the Fast Lane): ECG showing AV dissociation showing P waves (arrows).
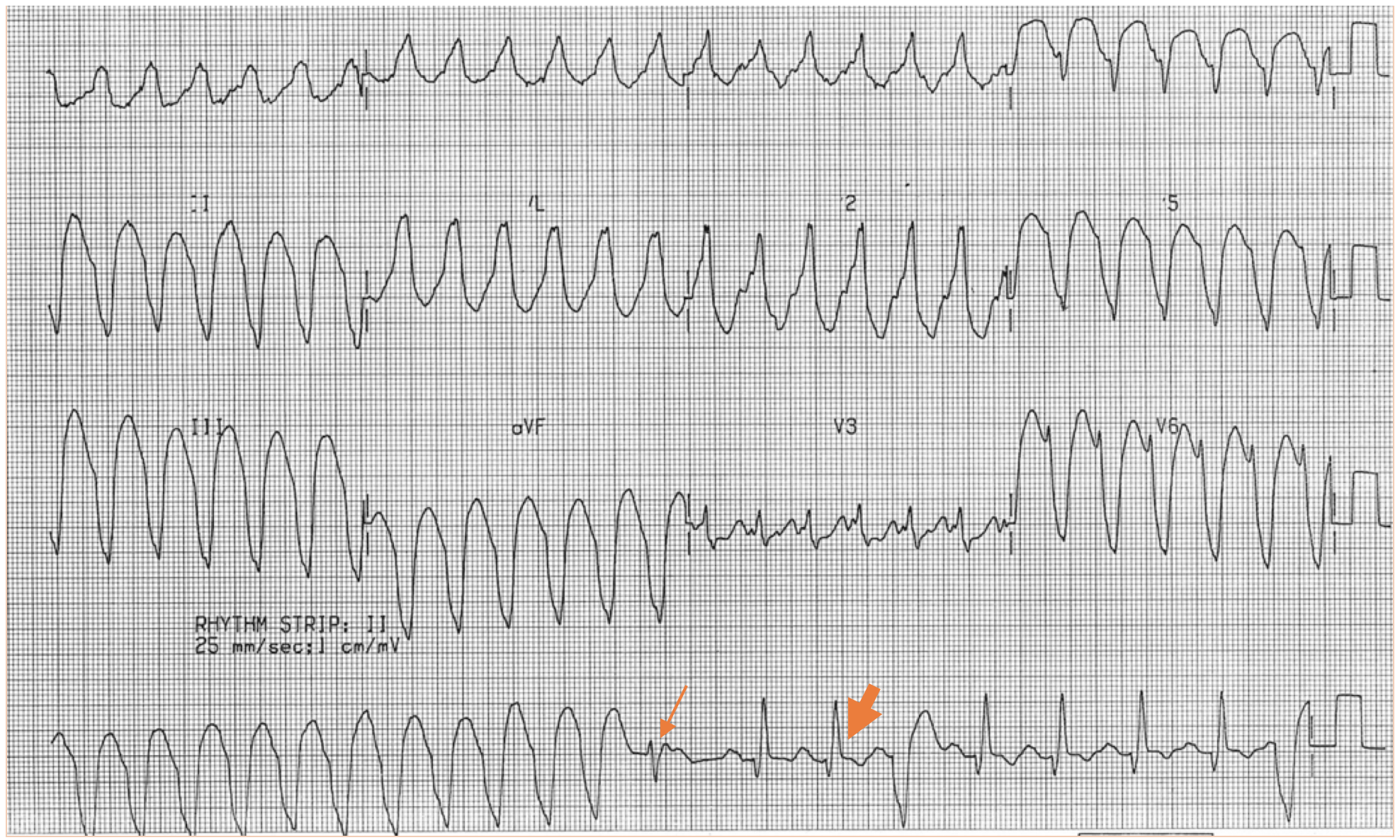
Figure 5 (Life in the Fast Lane): ECG showing fusion beats (small arrow) and capture beats (large arrow).
Wolff-Parkinson-White (WPW) syndrome
WPW is an “accessory pathway” syndrome, referring to a pre-excitation state that is caused by depolarization of the ventricles via an accessory pathway that bypasses the AV node. WPW can lead to an atrio-ventricular reentry tachycardia (AVRT) and very rapid heart rates.
Most often (~90%) the tachydysrhythmia of WPW is an orthodromic reentrant tachycardia, which occurs when the AV node conducts anterograde and the accessory pathway conducts retrograde for the circuit. In this setting, depolarization progresses normally through the ventricular conduction system, leading to a narrow complex tachycardia (Figure 5). However, infrequently (~10% incidence) the reverse can occur leading to depolarization of the ventricles through the accessory pathway. The AV node acts as the retrograde pathway that produces a wide-QRS complex antidromic AV-reentrant tachycardia, which mimics VT (Stapczynski & Tintinalli, 2011). It is imperative for emergency physicians to consider this in their differential of wide-complex tachycardias, especially in a person with known WPW, as treating an irregular antidromic AVRT (associated atrial fibrillation) with typical AV nodal blocking agents for stable VT or suspected SVT with aberrancy can be deadly.
Unfortunately, no great set of rules exist for differentiating an antidromic AVRT from VT, so keeping this as a consideration in a younger patient with previous similar episodes and with no structural heart disease is important (Dr. Smith’s). In a patient with suspected antidromic WPW with a regular rhythm, recent literature has shown that adenosine is safe and effective in differentiating wide-complex SVT from VT, but only if the rhythm is regular (Marill et al., 2009) (Figure 6). In a very rapid irregular wide-complex tachycardia suspicious for WPW with atrial fibrillation, the treatments of choice are Vagal maneuvers, procainamide (15-17mg/kg IV over 30 min, followed by IV infusion at 1-4mg per minute), or electrical cardioversion. Blocking the AV node can precipitate ventricular fibrillation, and thus AV nodal blockers such as adenosine, beta-blockers, amiodarone, and calcium channel blockers should be avoided.

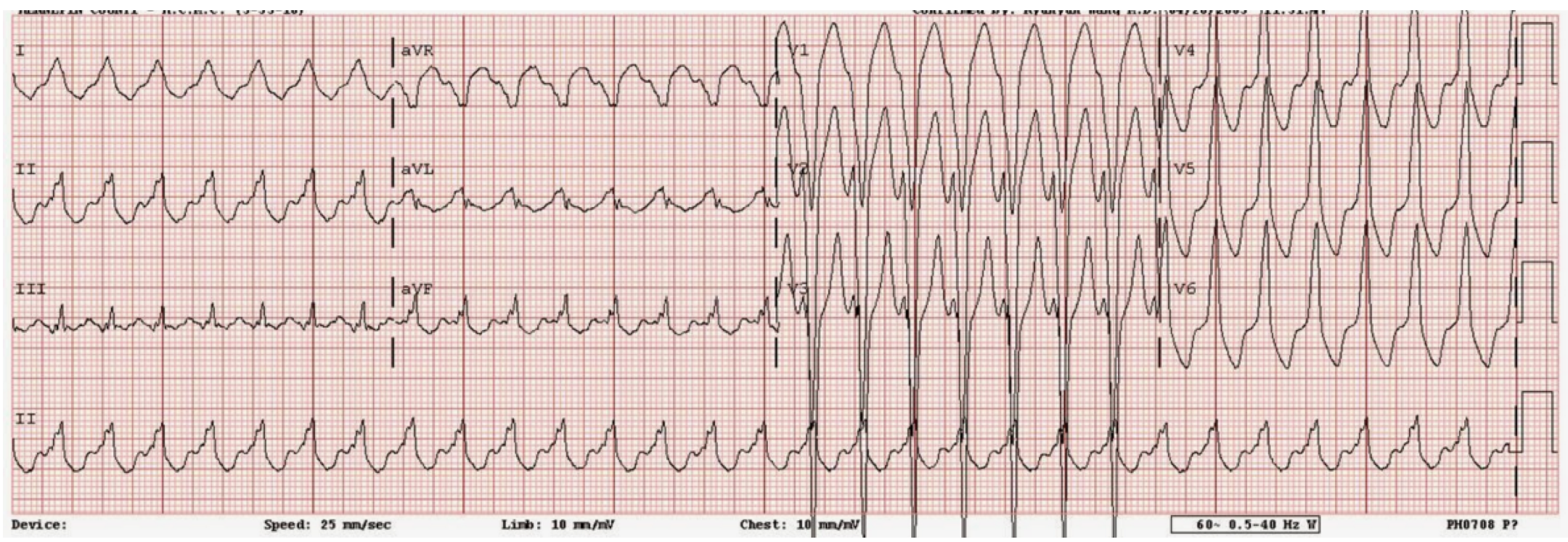
Figure 6 (Dr. Smith’s): ECG showing a rate of 180, regular, wide QRS complexes, treated with cardioversion and found to be antidromic WPW.

Figure 7 (Dr. Smith’s): Irregularly irregular wide-complex tachycardia, treated with cardioversion and found to be antidromic WPW with atrial fibrillation.
Hyperkalemia
Hyperkalemia can also be a confounding mimic and is one to always have on the differential of VT, especially in dialysis patients or those with known chronic renal insufficiency. Unfortunately, lab tests can often take upward of an hour to result, and some of the medications traditionally used for the treatment of stable VT can be deadly if there is an underlying hyperkalemia. ECG findings for mild hyperkalemia MAY include peaked T waves and a prolonged PR segment, but often can be normal. Moderate hyperkalemia may cause loss of P-waves, and the QRS complex may prolong, causing ectopic beats and escape rhythms. With severe hyperkalemia (levels 8.0 and above), we typically start to see unusually wide QRS complexes (>0.17 seconds) with a sine wave appearance (Figure 8). In patients with markedly wide “sine wave” QRS complexes, “slower” rates (<120 bpm) and a history of renal failure or dialysis, hyperkalemia should be high on the differential and treated immediately (Mattu, et al., 2000), (Life in the Fast Lane). Unfortunately, ECG findings in hyperkalemia do not necessarily reflect serum potassium levels.
Initial treatment includes administration of calcium for cardiac membrane stabilization, either calcium gluconate 10% with peripheral access (5-10mL IV) or calcium chloride 10% through central access (3x more potent, give 5-10Ml IV) up to 4 times per hour (Figure 9). Next, medications, such as IV insulin (aspart 10-20units) with dextrose 50g (25-50mL; consider two amps in hypoglycemic, euglycemic, or insulin naïve patients) or sodium bicarbonate (50-150 mEq IV, if metabolic acidosis or hemodynamic instability are present), are given to drive the potassium intracellularly. Lastly, medications that eliminate potassium from the body can be administered, including furosemide (40-80mg IV) or sodium polystyrene (25-50grams PO or rectally, though this medication is controversial). Emergent hemodialysis may be necessary in severe cases of hyperkalemia or in patients already receiving HD as an outpatient (Stapczynski & Tintinalli, 2011). Treatment with sodium blockers such as procainamide, lidocaine, or amiodarone may be deadly in the setting of hyperkalemia. For more on hyperkalemia, see this post on hyperK treatment controversies.

Figure 8 (Dr. Smith’s): ECG showing sine wave appearance of QRS seen in severe hyperkalemia.

Figure 9 (Dr. Smith’s): ECG taken 3 minutes after Figure 8, after 2 doses of calcium gluconate.
Sodium channel blocker toxicity
Another VT mimic is sodium channel blockade toxicity. The classic example is tricyclic antidepressant (TCA) toxicity, which in severe cases can cause a wide complex tachycardia reminiscent of VT. While TCA toxicity is the most commonly considered sodium channel blocking medication, there are many others including Type Ia antiarrhythmics such as procainamide, Type Ic antiarrhythmics such as flecainide, as well as antimalarial medications, propranolol, and carbamazepine. Significant sodium channel toxicity is seen on ECG as widening of the QRS interval (QRS>160 is predictive of ventricular dysrhythmias) and a right axis deviation of the terminal QRS complex, seen as a terminal R wave greater than 3mm in aVR (Harrigan & Brady, 1999) (Figure 10, 11).
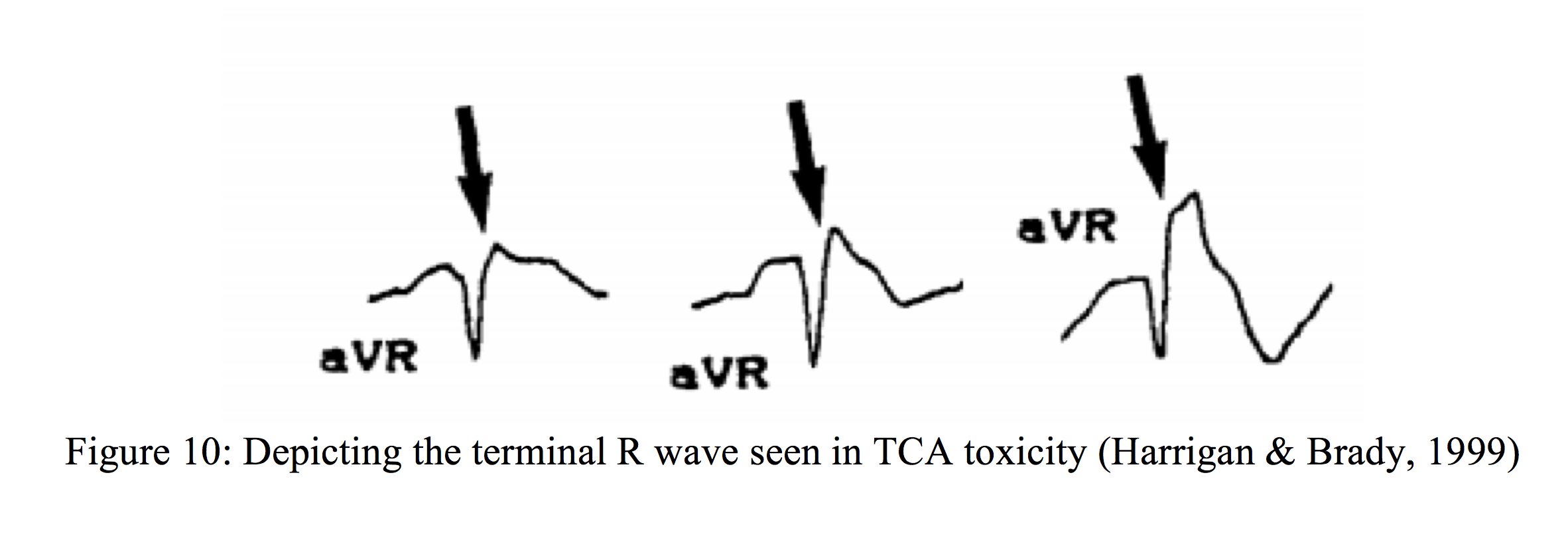

Figure 11 (Life in the Fast Lane).
TCA toxicity can also cause a sinus tachycardia due to its anticholinergic properties, in addition to a prolonged QT interval due to the drugs’ inhibition of potassium efflux. Management of severe sodium channel blocker/TCA toxicity leading to myocardial depression and a wide complex tachycardia includes standard resuscitative measures of rapid airway management as needed for seizures, altered mental status, or hemodynamic instability; adequate IV access; and monitoring equipment. The mainstay of treatment is IV sodium bicarbonate and should be dosed at 1-2mEq/kg repeated every 3-5 minutes until QRS complexes begin to narrow. If the patient is seizing, benzodiazepines such as diazepam 5-10mg IV or IM should be administered. If the patient is intubated, maintaining a pH of 7.5-7.55 can be helpful to prevent acidosis, which can exacerbate cardiac depression/arrhythmias. The type Ia and Ic antiarrhythmics mentioned above should be avoided, as should beta blockers and amiodarone due to potentially worsening of conduction abnormalities. One final consideration is that patients presenting within 1 hour of ingestion should be given 1g/kg of activated charcoal though a nasogastric tube after intubation, or orally if alert, awake, and willing to drink (Marx & Rosen, 2014).
Pacemaker Mediated Tachycardia (PMT)
The penultimate mimic we will discuss involves a re-entrant tachycardia that can occur in patients with dual chamber pacemakers. In PMT, a premature ventricular ectopic beat can trigger retrograde conduction occurring via the AV node outside the atrial refractory period, causing retrograde p-waves being sensed as atrial activity leading to further ventricular pacing (Stapczynski & Tintinalli, 2011) (Figure 12). The paced tachycardia can proceed at the maximum rate as determined by the pacemaker programming, and in patients with underlying coronary artery disease, the rapid rates of PMT can precipitate rate-related ischemia. The resulting wide complex tachycardia can be terminated by placing a magnet over the pacemaker (placing it in a fixed rate mode) or slowing AV node conduction with adenosine (6mg IV). Many modern pacemakers now have algorithms that enable the termination of PMT, so if the arrhythmia occurs, interrogation and replacement should be considered.

Figure 12 (Life in the Fast Lane): ECG depicting a rapid wide complex rhythm with no preceding atrial activity.
Idiopathic ventricular tachycardia
Another less commonly known mimic is idiopathic ventricular tachycardia, which is found in patients without known structural heart disease. There are two main types of idiopathic VT, both with different treatment algorithms, and are important to consider as a differential in younger, healthy patients presenting with VT. The first, known as right outflow tract tachycardia, has a VT focus arising from the right ventricular outflow tract. Episodes are often triggered by emotional stress or menstrual cycles and are usually self-limited. Rarely, this type of tachycardia can be symptomatic with chest pain, palpitations, and syncope (Srivathsan et al., 2005).
ECG findings are characteristic of a wide complex, LBBB pattern with a right (inferior) axis (Figure 13). First line therapy in the acute settings are vagal maneuvers and adenosine (6mg IV push, up to 24mg), with verapamil (5-10mg IV over 1 min) as a second-line option. Cardioversion may be used if pharmacotherapy fails or is contraindicated.
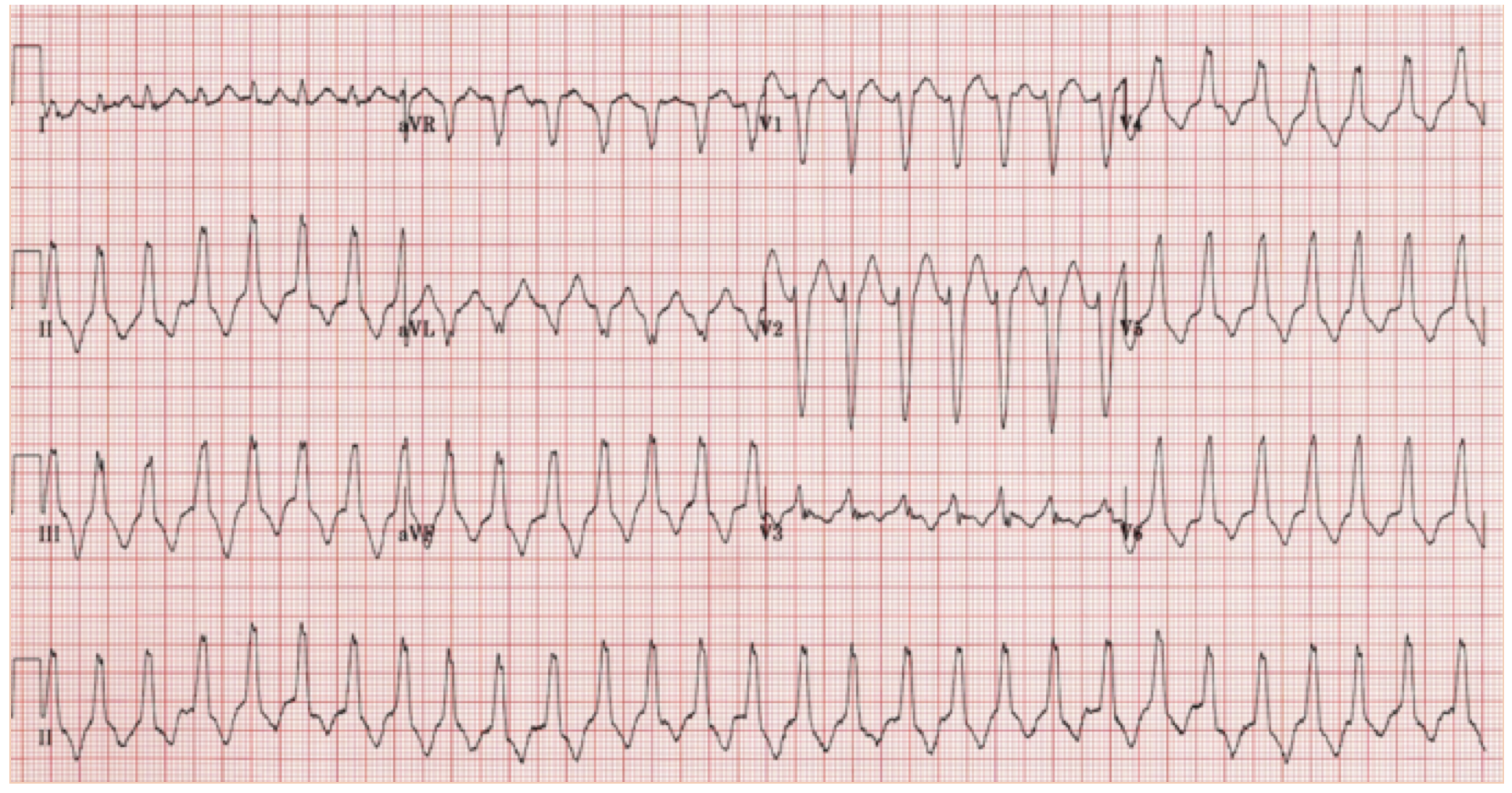
Figure 13 (Life in the Fast Lane): Right ventricular outflow tract tachycardia showing LBBB morphology, wide QRS complex, and inferior axis.
The second type of idiopathic ventricular tachycardia is known as fascicular ventricular tachycardia or idiopathic left ventricular tachycardia, with the focus arising in the left ventricle. Patients typically present with syncope or palpitations, with cardiac death being very rare. The arrhythmia is often precipitated by exercise. ECG findings show RBBB morphology with a left axis. First-line treatment is verapamil (5-10mgIV over 1 min), which is usually effective, giving this tachycardia the nickname “verapamil-sensitive” ventricular tachycardia. As always, cardioversion is also an option for the unstable patient (Srivathsan et al., 2005).
Conclusion
Back to our initial case of the 45-year-old with a history of renal failure with MI and also with prior similar episode. This patient is difficult because he could fit a lot of these mimics (SVT with aberrancy vs hyperkalemia vs drug toxicity vs. VT with structural heart disease). But a quick step by step review of all we learned today:
- Is the patient in cardiac arrest without pulses?
- If yes, start compressions and immediately defibrillate
- Is the patient unstable?
- If Yes then SHOCK with synchronized cardioversion (start at 100J and double from there, though no one will fault you for starting at 200J)
- Airway and code cart/equipment at bedside
- Is the patient stable? If yes, then…
- Does this patient have a history of WPW? (Are they young, <20 years old, similar prior episodes?) Consider antidromic WPW with atrial fibrillation if wide complex irregular rhythm => electricity is always a good option vs procainamide (15-17mg/kg IV over 30 min, followed by IV infusion at 1-4mg per minute)
- Is SVT with aberrancy likely? => Patient is younger (< than 50), previous similar episodes, BBB on prior ECG, no structural or ischemic heart disease), negative by all Brugada criteria
- IF YES then trial adenosine vs vagal maneuvers => start at 6mg => 12mg => 18mg IV push, but make sure you have pacer pads on when you do this!!
- Consider and treat serum electrolyte abnormalities such as hyperkalemia
- Consider and treat possible drug toxicities (sodium channel blocking agents, TCA toxicity)
- Does this patient have a pacemaker? Could this be PMT? If so, you can try adenosine or use a magnet to place pacer in a fixed pacing mode. Consult your electrophysiology colleagues for reprograming or replacement.
- If adenosine trial from step 2 is unsuccessful, or you skipped steps 2-5 because you are convinced this is VT (elderly, no pacemaker, structural/ischemic heart disease, VT by Brugada criteria), you can either:
- Perform light sedation (with etomidate 0.1 mg/kg, fentanyl 1 mcg/kg/dose, or ketamine 0.5-1 mg/kg) and synchronized cardioversion
- Give amiodarone 150mg IV over 10minutes
- Give Lidocaine 1-1.5mg/kg IV over 2-3 minutes
- Give Procainamide up to a max dose of 10-20mg/kg IV
- Remember, your consultants (aka Cardiology) are there for a reason! It’s always acceptable to ask for backup, and consider what else may be causing a wide-complex rhythm.
References / Further Reading:
– Brady, W.J., Mattu, A., Tabas, J., Ferguson, J.D. (2017). The differential diagnosis of wide QRS tachycardia. American Journal of Emergency Medicine. http://dx.doi.org/10.1016/j.ajem.2017.07.056
-Harrigan, R. A., & Brady, W. J. (1999). ECG abnormalities in tricyclic antidepressant ingestion. Am J Emerg Med, 17(4), 387-393.
–Life in the fast lane (2008). Life in the Fast Lane, [Australia]. https://lifeinthefastlane.com/
-Marill, K. A., Wolfram, S., Desouza, I. S., et al,(2009). Adenosine for wide-complex tachycardia: efficacy and safety. Crit Care Med, 37(9), 2512-2518. doi:10.1097/CCM.0b013e3181a93661
-Marx, J. A., & Rosen, P. (2014). Rosen’s emergency medicine: Concepts and clinical practice (8th ed.). Philadelphia, PA: Elsevier/Saunders.
– Mattu, A., Brady, W.J., Robinson, D.A. (2000). Electrocardiographic manifestations of hyperkalemia. American Journal of Emergency Medicine, 18(6), 721-729.
-McNally, B., Robb, R., Mehta, M., et al. (2011). Out-of-hospital cardiac arrest surveillance — Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005–December 31, 2010. MMWR Surveill Summ, 60(8), 1-19.
-Morgenstern, J. (2015, December 22). Management of unstable atrial fibrillation in the emergency department. Retrieved August 22, 2017, from https://first10em.com/2015/12/07/atrial-fibillation/
-Myerburg, R. J., Kessler, K. M., & Castellanos, A. (1992). Sudden cardiac death. Structure, function, and time-dependence of risk. Circulation, 85(1 Suppl), I2-10.
– Ortiz, M., Martin, A., Arribas, F., Coll-Vinent, B., del Arco C., Peinado, R., Almendralon, J. (2017). Randomize comparison of intravenous procainamide vs intravenous amiodarone for the acute treatment of tolerated wide QRS tachycardia: the PROCAIMO study. European Heart J, 38(17), 1329-1335.
-Page, R. L., Joglar, J. A., Caldwell, et al. (2016). 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia. Journal of the American College of Cardiology, 67(13), e27-e115. doi:http://dx.doi.org/10.1016/j.jacc.2015.08.856
-Smith, S.W. (2008). Dr. Smith’s ECG Blog. http://hqmeded-ecg.blogspot.com/
-Srivathsan, K., Lester, S. J., Appleton, C. P., Scott, L. R., & Munger, T. M. (2005). Ventricular tachycardia in the absence of structural heart disease. Indian Pacing Electrophysiol J, 5(2), 106-121.
-Stapczynski, J. S., & Tintinalli, J. E. (2011). Tintinalli’s emergency medicine: A comprehensive study guide (7th ed.). New York, N.Y.: McGraw-Hill Education LLC.
-Wood, J., & Ferguson, C. (2006). Procedural sedation for cardioversion. Emerg Med J, 23(12),932-934. doi:10.1136/emj.2006.043067





2 thoughts on “Ventricular Tachycardia Mimics”
Pingback: Länkar v49-50 | Internmedicin
Pingback: VT – Ventrikeltackykardi – Mind palace of an ER doc