Originally published at CoreEM.net, dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Original post written by Dr. Steven McDonald; Edited by Dr. Tim Greene; Posted by Dr. Anand Swaminathan
Follow Dr. Swaminathan and CORE EM on twitter at @EMSwami and @Core_EM
Lisfranc Injuries
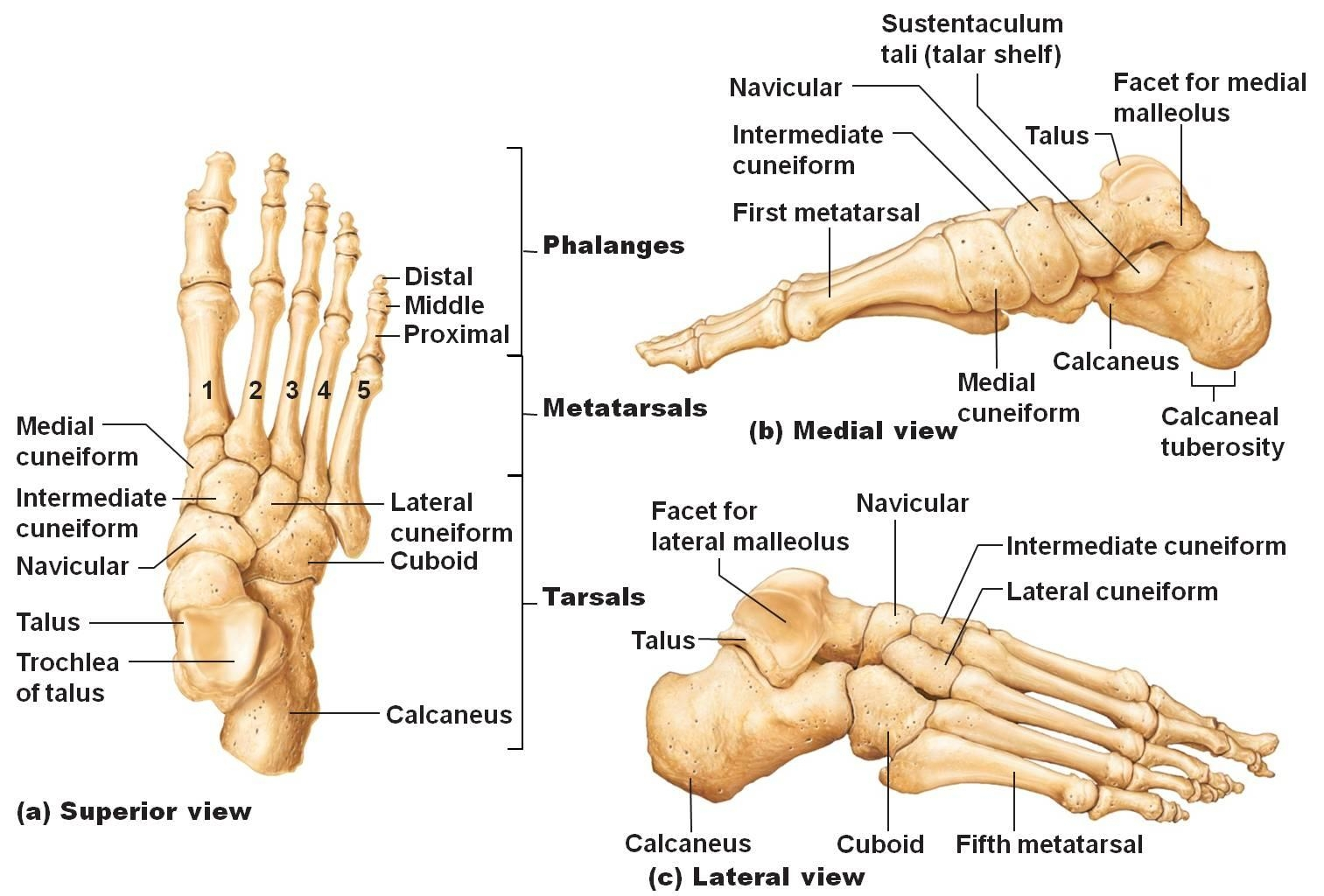
Anatomy of the Foot Bones (anatomyclass123.com)
Definition
- The Lisfranc joint complex is a tarso-metatarsal articulation named for Jacques Lisfranc (1790-1847), one of Napoleon’s battlefield surgeons.
- Specifically, it is the articulation of the 1st, 2nd, and 3rd metatarsals with the medial, intermediate, and lateral cuneiforms, respectively, as well as the articulation of the 4th and 5th metatarsals with the cuboid. (Englanoff 1995)
- The Lisfranc (or Oblique) ligament secures the second metatarsal to the medial cuneiform, serving as a mortise joint anchoring the entire complex and preventing medio-lateral or plantar displacement.
- Fractures and concomitant disarticulations of this joint are termed Lisfranc fracture-dislocations

Lisfranc Joint (orthoinfo.aaos.org)
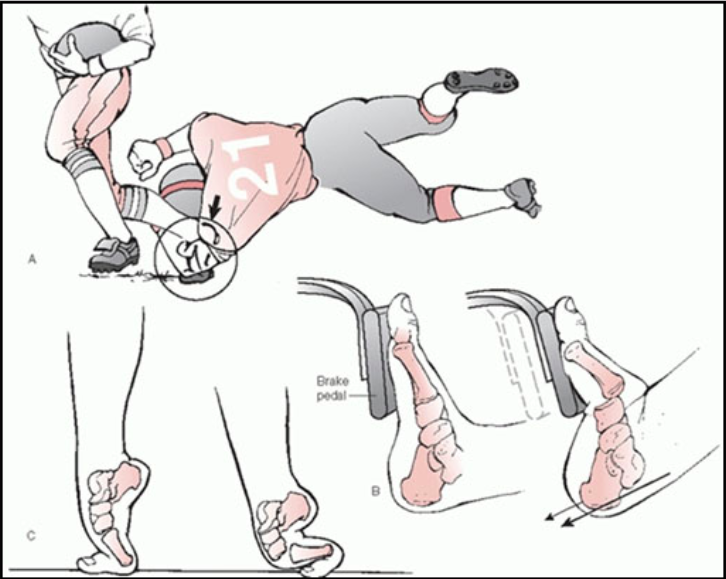
Lisfranc Mechanism of Injury (http://anklefootsurgery.com)
Mechanism of Injury
- Motor vehicle and industrial accidents constitute the majority of Lisfranc injuries.
- In elderly patients and athletes, Lisfranc injuries may occur after low-energy rotational events.
- Typically occurs when an axial load is applied to a plantar-flexed foot.
Epidemiology
- Prevalence: 1 in 55,000 (Sherief 2007)
- Missed on first evaluation in 20% of cases (Englanoff 1995)
Classification
- No validated formal classification scheme exists for assessing the severity or management of a Lisfranc injury

Volar Surface Ecchymosis (http://www.orthopaedicsone.com/)
Physical Exam
- In cases of complete ligamentous tear, ecchymotic discoloration of the plantar midfoot is common; however, findings on inspection may be subtle or absent.
- Tenderness to palpation over the midfoot
- Stress examination of the midfoot
- Performed by stabilizing the heel with one hand and twisting the forefoot with the other.
- Markedly exacerbates pain
- The “Piano Key” test: Exacerbation of pain with dorsal and plantar flexion of each digit (Wedmore 2015)
- Single limb heel raise: Exacerbation of pain when patient stands on one leg and then on tip toes (places significant strain on injured area)

Lisfranc Joint Normal Alignment (Case courtesy of Dr Wael Nemattalla, Radiopaedia.org. From the case rID: 10121)
Imaging
- Patients may not meet Ottawa ankle/foot imaging rules. In patients with suspicious mechanism, have a low threshold to image
- X-ray Yield
- High-energy mechanism: Obvious fracture/dislocation of the associated tarsal and metatarsal bones will likely (but not definitely) be present on x-ray.
- Low-energy mechanism (with high clinical suspicion of Lisfranc injury): Weight-bearing AP views of the foot can help make the diagnosis if the initial foot x-ray is normal.
- Subtle x-ray findings suggestive of a clinically significant Lisfranc injury:
- Loss of the smooth alignments at the medial border of the second metatarsal with the medial cuneiform and/or the medial border of the fourth metatarsal with the cuboid
- Diastasis (separation beyond normal) of the space between the bases of the 1st and 2nd metatarsals
-
- Diastasis is a measurement >2mm in a normal foot, or >1mm relative to the contralateral foot in people with widened joint spaces at baseline
- Bilateral films are thus necessary when obtaining weight-bearing views.
-
- A metatarsal shaft should never be more dorsal than its respective tarsal bone
- Presence of an avulsion fracture, called the “fleck sign”
Lisfranc Injury X-Rays
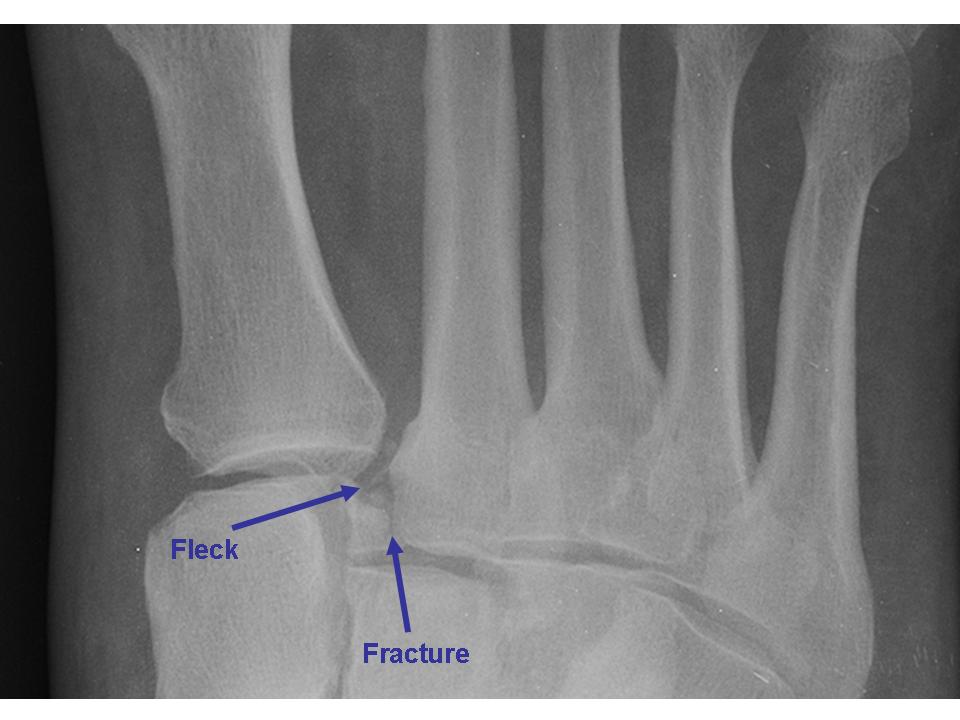
Fleck Sign (http-::ortho-teaching.feinberg.northwestern.edu:)

Lisfranc Joint

Lisfranc Fracture – Lateral X-ray (Case courtesy of Dr Hanisalam, Radiopaedia.org. From the case rID: 10948)

Metatarsal Diastasis (https://sportsinjuryupdatedotcom.files.wordpress.com)
ED Management
- Carefully perform neuromuscular examination with special attention to dorsalis pedis (DP) pulse – transection is rare but well described
- Any of the following conditions requires emergent reduction and orthopedic consultation
- Fracture displacement
- Associated dislocation
- Evidence of compartment syndrome
- Evidence of neurovascular injury
- CT scan of the foot
- Improved visualization particularly when X-rays equivocal but continued suspicion (i.e. inability to bear weight)
- Operative planning
- Obtaining CT in ED will depend on department resources and orthopedic referral availability
- Immobilization with posterior splint
- Strict non-weight bearing (NWB) on crutches
- Orthopedic or podiatry follow-up within one week for possible surgical reduction and fixation
Prognosis
- When initially misdiagnosed/untreated, Lisfranc injuries carry a poor prognosis, often resulting in deformity, functional deficit, and chronic pain
- When diagnosed appropriately, patients who undergo open reduction and internal fixation of fractures have superior outcomes to those with purely ligamentous injury (Sherief 2007)
- Patients with no fracture on CT and no displacement on weight-bearing films generally are managed non-operatively
Take Home Points
- A Lisfranc injury must be part of the differential for any midfoot trauma because of the significant morbidity associated with missed diagnosis
- Physical exam findings, including deformity, swelling and ecchymosis, may be subtle or absent
- Normal foot x-rays do not rule out a Lisfranc injury, weight-bearing views or CT are essential
References
- Englanoff G et al. Lisfranc Fracture-Dislocation: A Frequently Missed Diagnosis in the Emergency Department. Ann Emerg Med 1995: 26 (2); 229-233. PMID: 7618790
- Sherief, T et al. Lisfranc injury: How frequently does it get missed? And how can we improve? Injury: International Journal of the Care of the Injured 2007: 34; 856-860. PMID: 17214988
- Wedmore, I. et al. Emergency Department Evaluation and Management of Foot and Ankle Pain. Emergency Medicine Clinics of North America May 2015: 33 (2); 371-372. PMID: 25892727




