
Welcome back to the “52 in 52” series. This collection of posts features recently published must-know articles. Our thirteenth post looks at the ARREST trial.

Author: Christiaan van Nispen, MD (Emergency Medicine Physician Resident, San Antonio, TX) and Brannon Inman (Chief Resident, Emergency Medicine Physician, San Antonio, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single-center, open-label, randomized controlled trial
AKA: The “ARREST” Trial
Clinical question:
In patients aged 18-75 presenting with refractory ventricular fibrillation within 30 minutes of out-of-hospital cardiac arrest (OHCA), is immediate initiation of veno-arterial extracorporeal membrane oxygenation (VA ECMO) with angiography and reperfusion (if indicated) superior to standard advanced cardiac life support (ACLS) with angiography and reperfusion after return of spontaneous circulation (ROSC)?
Study design:
- Phase 2, single-center, open-label, randomized clinical trial
PICO:
Population:
- Appear to be 18-75 years of age
- Single center: University of Minnesota Medical Center within 30 minutes of OHCA with compressions being administered by an automated device
- Refractory (≥ 3 shocks administered without ROSC) ventricular fibrillation or pulseless ventricular tachycardia (ultimately, all patients enrolled were in ventricular fibrillation)
- Excluded:
- Patients with demonstrated do-not-resuscitate orders
- Patients with blunt, penetrating, or burn-related trauma
- Cardiac arrest due to drowning
- Known overdose
- Nursing home residents
- Patients with terminal cancer
- Patients with active gastrointestinal or other internal bleeding
- Pregnant or incarcerated patients
- Patients enrolled but declared clinically deceased without further intervention if any one of the following was present:
- End-tidal CO2 < 10 mm Hg
- PaO2 < 50 mm Hg
- Arterial oxygen saturation < 85 percent
- Lactic acid level > 18 mmol/L
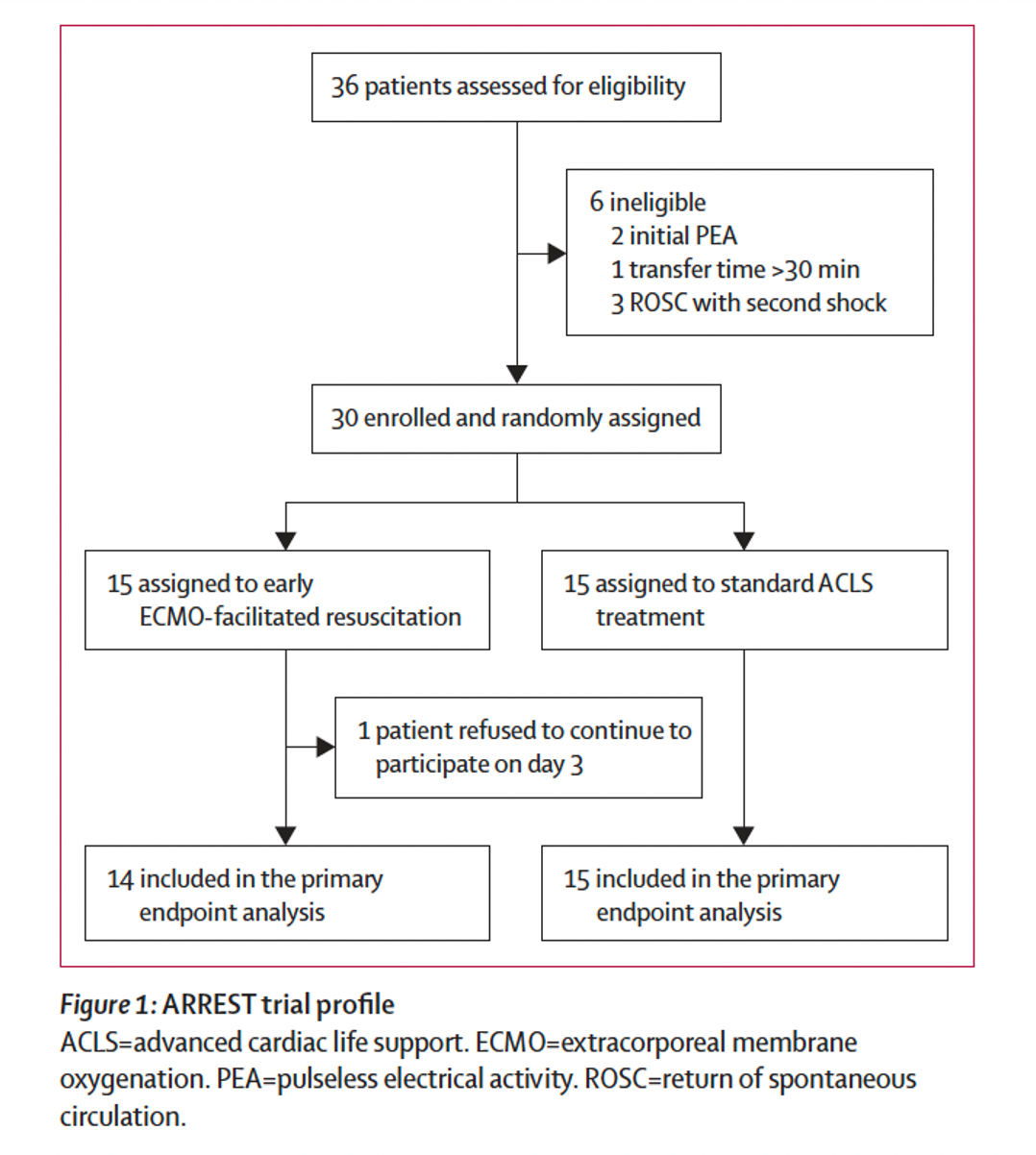
- Intended to enroll 5 rounds of 30 patients; enrollment discontinued by Data Safety Monitoring Board after the first group of 30 due to 0.986 posterior probability that remaining groups would not change the outcome
- 30 of 36 screened were enrolled; 1 ECMO group patient withdrew consent on day 3
Randomization: Largely balanced with the following noted –
- ECMO group had more males compared to the ACLS group (93 versus 73 percent)
- ECMO group with less known coronary artery disease (13 versus 27 percent)
- Though most markers of resuscitation on arrival were similar, the ECMO group had mildly higher initial arterial oxygen (86 versus 77 mm Hg)
- As only 30 patients were ultimately enrolled, some baseline characteristics were bound to be somewhat dissimilar
Intervention:
- On arrival, immediately taken to the cardiac catheterization lab for VA ECMO cannulation
- After cannulation, angiography was performed with reperfusion if clinically indicated
Comparator:
- Standard ACLS continued in the emergency department for at least 15 minutes after arrival or 60 minutes from activation of the 911 system
- If ROSC was achieved, the patient was taken to the cardiac catheterization lab for angiography, with reperfusion if clinically indicated
Patients in both groups who survived past the cardiac catheterization lab received the following standardized care in the cardiac intensive care unit:
- Targeted temperature management (34⁰C for 24 hours)
- Computed tomography of the head on the day of arrival and day 3
- Continuous EEG until awake
- Neuro-prognostication no sooner than 72 hours
- Other critical care management per intensivists, who were blinded to group allocation
Outcome:

- Significantly more patients achieved primary outcome in the ECMO group
- All ECMO group survivors made meaningful recoveries (see secondary outcomes)
- No patient in the ACLS group made meaningful recovery
- Two patients in the ECMO group were declared clinically dead based on criteria (see: Population) and neither cannulated nor received cardiac catheterization, though their deaths are still recorded against the ECMO group
- As above, the study intended to enroll 5 rounds of 30 patients with a review between each round; enrollment was discontinued by Data Safety Monitoring Board after the first round due to a 0.986 posterior probability that the remaining groups would not change the outcome
Take away:
- Significantly more patients survived to hospital discharge in the ECMO group; the only ACLS survivor died before 3 months.
- Of the ECMO group survivors, there was minimal functional disability at 6 months considering their presenting problem was refractory ventricular fibrillation (study authors state that poor mRS at discharge largely related to deconditioning after hospitalization, which improved with physical therapy and other rehabilitation).
- ECMO group also received emergent angiography and if needed, reperfusion, which may have aided in a superior outcome (ACLS group only received this if ROSC was achieved).
- Nursing home residents (who often have more comorbidities and impairment of acts of daily living at baseline) and the elderly (≥ 75 years old) were excluded likely puts the study in a stronger position to achieve good outcomes for their enrollees.
- This study was conducted at a single center in a metropolitan area (where EMS transport times are lower) with the staffing and facilities to immediately cannulate patients for ECMO, perform angiography, and then further manage them in a cardiac ICU; the combination of all these factors are not present at many United States hospitals, especially not 24 hours per day.
- All enrolled patients had primary VF arrest.

My take:
This is a potentially practice-changing study for the management of out-of-hospital cardiac arrest in the non-trauma setting. Not only did an impressive percentage of early ECMO patients survive to discharge, but they also had no or only slight disability by 6 months. However, it is worth noting all enrolled patients in both arms had primary VF arrest. Furthermore, it will be difficult to readily implement these protocols at most facilities, as it would require around-the-clock access to immediate ECMO and cardiac catheterization, which is not a reality in many hospitals. It could be though, at least in metropolitan areas, if local authorities, hospitals, and EMS systems work together to have at least one medical center with these capabilities active around the clock, with EMS protocols in place to bring all cardiac arrest patients to that facility as quickly as possible.
Reference:
- Yannopoulos D, Bartos J, Raveendran G et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomized controlled trial. 2020;396(10265):1807-1816. doi: 10.1016/S0140-6736(20)32338-2.
Appendix:
Cerebral performance category (CPC)
- Good cerebral performance: conscious, alert, able to work, might have mild neurologic or psychologic deficit
- Moderate cerebral disability: conscious, sufficient function for independent activities of daily life. Able to work in sheltered environment
- Severe cerebral disability: conscious, dependent on others for daily support. Can be ambulatory to severe dementia or paralysis
- Coma or vegetative state without presence of all brain death criteria
- Brain death: apnea, areflexia, EEG silence
Source: Kiehl EL, Parker AM, Matar RM, et al. C-GRApH: A validated scoring system for early stratification of neurologic outcome after out-of-hospital cardiac arrest treated with targeted temperature management. J Am Heart Assoc.2017;6(5):e003821. Doi: 10.1161/JAHA.116.003821
Modified Rankin Score (mRS)
- No symptoms of neurologic disability
- No significant disability despite some symptoms; able to carry out all usual duties and activities
- Slight disability; unable to carry out all previous activities, but able to look after own affairs without assistance
- Moderate disability; requires some help but able to walk without assistance
- Moderately severe disability; unable to walk and attend to bodily needs without assistance
- Severe disability; bedridden, incontinent, and requiring constant nursing care and attention
Source: MDCalc. Modified Rankin Scale for Neurologic Disability. Accessed June 21, 2022. https://www.mdcalc.com/modified-rankin-scale-neurologic-disability




