Author: Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF) // Edited by: Jennifer Robertson, MD, MSEd and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
A 54-year-old male with a history of hypertension, coronary artery disease, and hyperlipidemia presents to the emergency department (ED) with a chief complaint of transient right-sided weakness. The weakness lasted five minutes and then resolved without any residual deficits.
The patient’s exam reveals normal vital signs and normal neurologic exam including cranial nerves, motor, sensory, reflexes, cerebellar, and gait. His electrocardiogram (ECG) reveals left ventricular hypertrophy. The patient’s head computed tomography (CT) is normal.
What work up and management are indicated for transient weakness? What is the appropriate disposition? This article will address the diagnosis and management of transient ischemic attacks (TIA), transient weakness, and more.
How is TIA defined?
The TIA was once defined as a transient neurologic deficit, due to ischemia, with resolution of symptoms in less than 24 hours. In 2009, the American Heart Association (AHA) redefined the TIA as a ‘brief episode of neurological dysfunction resulting from focal cerebral ischemia not associated with permanent cerebral infarction.’ Importantly, even if a patient has resolved symptoms but has a visible infarct on imaging, he or she should be classified as having a stroke.1 Diagnosing a stroke requires imaging resources, most commonly diffusion–weighted magnetic resonance imaging (DWI). With the new definition of TIA, the annual incidence of stroke has increased, but the number of patients disabled due to stroke has decreased.2
TIAs should be taken seriously. In 2007, Johnston et al. demonstrated that patients with TIAs have a 5% risk of stroke within two days and a 10% risk of stroke within three months after sustaining the initial TIA.1,3 TIAs are thought to precede approximately 14%-23% of acute ischemic strokes (AIS). 4,5 A second study demonstrated similar numbers and also found that symptom duration over 60 minutes, age over 60 years, and increased blood pressure were associated with worse clinical outcomes.6
Is everything that presents as a TIA actually a TIA?
Unfortunately, not every person who presents with a transient focal neurologic deficit actually has a TIA. Atypical migraines, encephalopathy, seizures, neuropathy, psychiatric conditions, and metabolic pathology can all present as mimics of TIA. The literature demonstrates that anywhere between 5% and 31% of patients presenting with stroke-like symptoms actually have alternative diagnoses. Prabhakaran et al. found high rates of misdiagnosing mimics as TIA, with misdiagnosis rates ranging from 30% to 62%.7
Another study by Whiteley et al. found that 1/3 of patients with suspected TIA actually had a TIA mimic.8 Similarly, in a cohort study of 303 patients, approximately 18% of suspected TIA patients actually had experienced a mimic.9 Unfortunately, this study also found patients with TIA and mimics to have similar rates of vascular comorbidities, blood pressures upon arrival, duration of symptoms, aphasia, dysarthria, vertigo, unilateral sensory loss, and hemianopia.9 This can most certainly make diagnosing an actual TIA more difficult. The authors did find, however, that memory loss, headache, and blurred vision were associated with mimics, while unilateral weakness was more associated with true TIA.
Is imaging helpful in diagnosing TIA?
Unfortunately, this is complicated. A 2012 study by Förster et al evaluated imaging techniques in patients with symptoms concerning for acute TIA. The authors found that within the first 24 hours of symptoms, imaging is not perfect. CT rarely demonstrates acute ischemic findings. In the same 2012 study, 95.7% of scans were found to be normal and only 4.3% showed possible infarction. Magnetic resonance imaging (MRI) was found to be somewhat better, demonstrating 35% of acute infarcts.10 If possible, MRI with diffusion-weighted imaging (DWI) should be obtained, as it is more sensitive than CT for detecting acute ischemia, prior bleeding, and other lesions.11,12 MRI can also be helpful in these patients as those with DWI abnormalities are at high risk for stroke no matter their prognostic score (see below).13
Doppler ultrasound (US), CT angiography, and magnetic resonance angiography (MRA) comprise further options for vascular imaging. Carotid Doppler US is often used to evaluate for carotid stenosis, where greater than 50% stenosis warrants consideration for further treatment.1
Are scoring systems helpful?
One big question regarding stroke care is whether one can predict who will experience a stroke following a TIA. The assumed risk of stroke within 90 days following a TIA is approximately 10%. Several scoring systems to help predict possible stroke are available. The ABCD2 score is perhaps the most well-known. Unfortunately, this score does not take imaging into account.
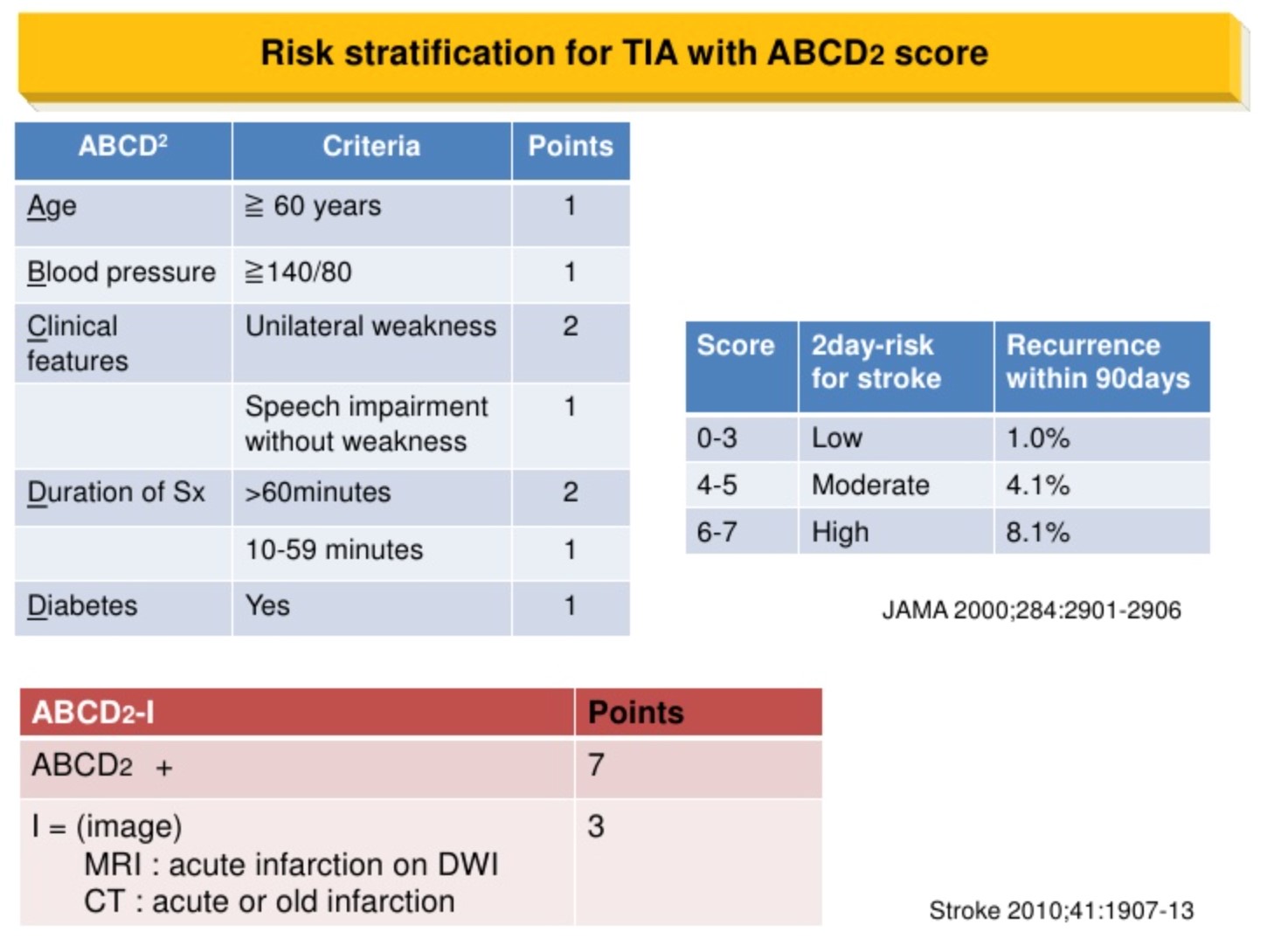
Diagram http://image.slidesharecdn.com/chadabcdscore-111029024736-phpapp02/95/chads2-and-abcd-score-2-728.jpg?cb=1319856502
We are classically taught using the ABCD2 score will adequately predict stroke risk. However, recent literature questions the predictive value of this score. In 2011, Perry et al. conducted an external validation of the ABCD2 and found that by using this score, physicians may misclassify up to 8% of patients as low risk. Additionally, the sensitivity of the score for high risk patients was found to be only 31.6%.14 Stead et al. compared the ABCD2 score to brain and carotid imaging for risk stratification and found the ABCD2 score to provide no useful additional information.15 Schrock et al. found the ABCD2score to be unhelpful toward guiding diagnostic testing, as 15% of patients with high grade carotid stenosis would be missed if ABCD2 was used alone.16 An Australian study also assessed use of the ABCD2 score in the ED and found the ABCD2 to have poor predictive value toward determining future stroke. Those patients who were calculated as low, moderate, and high risk on the ABCD2 all had similar rates of stroke at 30 and 90 days (around 1% at 30 days and 2% at 90 days).17 An Annals of Emergency Medicine study in 2013 conducted a meta-analysis of the ABCD2 score and found it to be suboptimal in reliably predicting future stroke.18
Hence, the use of the ABCD2 score is questionable for predicting risk of future stroke. Therefore, a 2014 Japanese study modified the score and produced the ABCD3-I score.19 The third D stands for “dual TIA,” or a second TIA episode within one week of the first TIA. The “I” component refers to any abnormal magnetic resonance imaging and/or carotid stenosis greater than 50%. The study found that dual TIA and carotid stenosis were associated with higher stroke risk, but abnormal MRI imaging was not. Unfortunately, the modified score did not even reach moderate prediction capabilities (C-statistic of 0.66 for ABCD3-I), but it did fare better than the original score (C-statistic of 0.54 for ABCD2). 19
Currently, scoring systems should not take the place of clinical gestalt. They can assist providers in evaluating for risk factors, but they cannot definitively stratify patients into clear-cut categories.
What is the disposition?
The current literature indicates that predicting future stroke risk in patients with TIAs is difficult. Most would argue that urgent evaluation, risk stratification, and preventative therapy are needed for these patients. Controversy does exist regarding the need for admission, but fortunately, the American Heart Association (AHA) and the National Stroke Association (NSA) have developed certain admission criteria that can be helpful when determining a patient’s disposition needs.
AHA: ABCD2 score of > 3, ABCD2 score of 0-2 and uncertain follow up, or ABCD2 score of 0-2 and evidence that focal ischemia occurred.1
NSA: Consider admission if first TIA within 24-48 hours. For recent TIA within one week, hospitalization is needed for worsening TIA symptoms, duration of symptoms longer than one hour, internal carotid stenosis greater than 50% with symptoms, known cardiac source of embolus, or hypercoagulable state.20
Also, when determining disposition, local resources and patient population should be considered. Difficulty in obtaining follow up and unclear follow up also suggest need for admission.
In patients for whom follow up can be obtained with none of the above high risk factors, acute clinics, rapid evaluation units, or observation units have shown promise. One study found that patients with follow up within one day demonstrated a 90 day stroke reduction of 8%.21 ED observation units may reduce cost, shorten length of stay, and adequately risk stratify TIA patients in association with neurology consultation.22
Rapid evaluation units
The EXPRESS (Effect of urgent treatment of transient ischemic attack and minor stroke on early recurrent stroke) study conducted in the UK evaluated the use of TIA clinics versus primary care management in patients not admitted to the hospital. Not surprisingly, risk stratification and treatment were faster in the TIA clinic, as well as a significant reduction in stroke from 10% to 2%.21 A study evaluating the use of a round-the-clock TIA clinic called the SOS-TIA clinic, evaluated 1085 patients in a hospital-based clinic, finding a 90 day stroke rate of 1.24% in clinic patients.23 Another study conducted in Germany evaluated outcomes in patients with TIA treated in outpatient clinics that specialize in workup.24 The clinic was staffed by neurologists, and each patient received a MRI or head CT, a carotid US, an ECG, and ankle-brachial indices (ABI). The authors of this study found the stroke rate at 90 days to be 1.6% overall, with 2.9% in the population experiencing TIA or minor stroke. Similarly, a Canadian study found a decreased risk of stroke at 90 days by using the ABCD2 score in conjunction with testing such as carotid US and brain imaging at an outpatient stroke prevention clinic.25 Other studies have shown similar results, with rapid access to a specialized clinic/unit that can risk stratify, properly image, and treat patient comorbidities to reduce stroke risk, but they may result in higher costs.25-27
A dedicated TIA unit, whether TIA clinic or ED observation unit with expedited workup, can reduce recurrent events and need for hospitalization. Studies with these units have found 90 day rates of recurrent events ranging from 1.7% to 3.2%.20,23,27-29
How should patients be managed?
Cornerstones of treatment for TIA revolve around reducing the risk of future events with blood pressure control, lipid control, and antiplatelet agents.1,20,23,30-32 Blood pressure should be maintained at 140/90 with a thiazide diuretic and/or an ACE inhibitor. Statins should be given to keep LDL of under 100mg/dL or 70mg/dL in high risk patients. Niacin or gemfibrozil are recommended to maintain HDL above 40mg/dL. Antiplatelet agents include aspirin with or without dipyridamole, or clopidogrel alone. 33
Multiple studies have evaluated the most efficacious antiplatelet regimen, whether mono or dual therapy. Dual antiplatelet therapy is commonly administered to patients with acute coronary syndromes; however, it is controversial in TIA. An Australian study found aspirin reduced the absolute risk of stroke in high-risk patients from 7% to 6.1%, with a number needed to treat (NNT) of 110. The addition of clopidogrel produced another 0.5% absolute reduction in stroke, with a NNT of 200.32 Diener et al. found no difference between clopidogrel and aspirin in low risk patients, but clopidogrel was superior in high-risk patients (diabetes, cardiac disease, prior stroke or MI, hyperlipidemia). However, a higher bleeding risk was found in dual therapy.33
In 2013, the CHANCE (Clopidogrel in High-risk patients with Acute Nondisabling Cerebrovascular Events) trial found a 1.4% stroke reduction in patients who used combination therapy (aspirin 75mg daily and clopidogrel 75mg daily). No increased bleeding risk was found. However, aspirin was also provided at only 75mg, as compared to 325mg in other studies.34 Additionally, the study population was predominantly Chinese, which is an important aspect as the Chinese population generally has higher rates of cerebrovascular attacks (CVA), prior CVAs and TIAs, and higher smoking rates than patients in the United States. Later in 2013, Wong et al. conducted a meta-analysis of 14 randomized controlled trials (RCTs), and also included the original CHANCE study. The authors compared multiple medication regimens and found dual antiplatelet therapy with clopidogrel and aspirin to be associated with decreased stroke risk (relative risk of 0.69), without significantly increasing bleeding risk. Aspirin and dipyridamole were not associated with any risk reduction.35
Other studies including CHARISMA (Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance), SPS3, and MATCH trials found no statistical difference between mono-therapy and dual-therapy in reducing future events, but an increased rate of bleeding with dual therapy. 36-38 More recent meta-analyses suggest early treatment with dual therapy within 24 hours of the event may reduce risk of future events, but this should not be extended past 21 days.39,40 Currently, there is insufficient evidence in American populations to recommend clopidogrel plus aspirin, and guidelines from the AHA and NSA should be followed. The ongoing POINT (Platelet Oriented Inhibition in new TIA and minor ischemic stroke) trial is being conducted in the U.S. evaluating clopidogrel with aspirin and aspirin monotherapy.41
Future Treatments
Medications currently under investigation include cilostazol (predominantly studied in Japan),42 ticagrelor,43 and the new oral anticoagulants. Apixaban, dabigatran, edoxaban, and rivaroxaban may play a future role in prevention of recurrent events.44-49
Other therapies
Cardioembolic TIA is a different animal in that stroke prophylaxis also requires anticoagulant medications. Atrial fibrillation with TIA requires warfarin with a goal INR of 2-3. Anticoagulation is also recommended in the setting of acute myocardial infarction with left ventricular thrombus, dilated cardiomyopathy, or valvular disease.1,20,31
If a major intracranial artery has stenosis of 50%-99%, angioplasty or stent placement may be needed in association with aspirin, blood pressure management, and lipid control. 1,20,31
Bonus:
What is the updated 2015 ACEP Clinical Policy on acute ischemic stroke (AIS)?
Question 1: Is intravenous (IV) tissue plasminogen activatior (tPA) safe and effective for acute ischemic stroke patients if given within 3 hours of symptoms onset?50
Level A: none.
Level B: IV tPA should be offered and may be given to select patients with acute ischemic stroke. The increased risk of symptomatic intracerebral hemorrhage (sICH) should be considered.
Level C: shared decision making when feasible.
Question 2: Is IV tPA safe and effective for acute ischemic stroke patients treated between 3 to 4.5 hours after symptom onset?
Level B: Despite the known risk of spontaneous intracranial hemorrhage (sICH) and the variability in the degree of benefit in functional outcomes, IV tPA may be offered and given to carefully selected AIS patients within 3 to 4.5 hours after symptom onset at institutions where systems are in place to safely administer the medication.
The policy lists a NNT of 8 for excellent functional outcome if tPA is given within 3 hours of symptom onset and a NNH of 17 for symptomatic intracerebral hemorrhage.
References / Further Reading
- Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke 2009; 40 (6): 2276-93.
- Chalela JA, Kidwell CS, Nentwich LM, et al. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet. 2007;369(9558):293-298.
- Whiteley WN, Wardlaw JM, Dennis MS, Sandercock PA. Clinical scores for the identification of stroke and transient ischaemic attack in the emergency department: a cross-sectional study. J Neurol Neurosurg Psychiatry. 2011 Sep;82(9):1006-10.
- Amort M, Fluri F. Transient ischemic attack versus transient ischemic attack mimics: frequency, clinical characteristics and outcome. Cerebrovasc Dis. 2011;32(1):57-64.
- Förster A, Gass A. Brain imaging in patients with transient ischemic attack: a comparison of computed tomography and magnetic resonance imaging. Eur Neurol. 2012;67(3):136-41.
- Perry JJ, Sharma M. Prospective validation of the ABCD2 score for patients in the emergency department with transient ischemic attack. CMAJ. 2011 Jul 12;183(10):1137-45.
- Stead LG, Suravaram S. An assessment of the incremental value of the ABCD2 score in the emergency department evaluation of transient ischemic attack. Ann Emerg Med. 2011 Jan;57(1):46-51.
- Schrock JW, Victor A, Losey T. Can the ABCD2 risk score predict positive diagnostic testing for emergency department patients admitted for transient ischemic attack? Stroke. 2009 Oct;40(10):3202-5.
- Ghia D, Thomas P. Low positive predictive value of the ABCD2 score in emergency department transient ischaemic attack diagnoses: the South Western Sydney transient ischaemic attack study. Intern Med J. 2012 Aug;42(8):913-8.
- Kiyohara T1, Kamouchi M. ABCD3 and ABCD3-I scores are superior to ABCD2 score in the prediction of short- and long-term risks of stroke after transient ischemic attack. Stroke. 2014 Feb;45(2):418-25.
- Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007; 370(9596):1432-1442.
- Lavalle ́e P, Meseguer E, Abboud H, et al. A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects. Lancet Neurol. 2007;6(11):953-960.
- Hörer S, Schulte-Altedorneburg G, Haberl RL. Management of patients with transient ischemic attack is safe in an outpatient clinic based on rapid diagnosis and risk stratification. Cerebrovasc Dis. 2011;32(5):504-10.
- Wasserman J, Perry J, Dowlatshahi D, et al. Stratified, urgent care for transient ischemic attack results in low stroke rates. Stroke. 2010;41(11):2601-2605.
- Wu CM, Manns BJ, Hill MD, Ghali WA, Donaldson C, Buchan AM. Rapid evaluation after high-risk TIA is associated with lower stroke risk. Can J Neurol Sci. 2009 Jul; 36(4):450-5.
- Olivot JM, Wolford C, Castle J, et al. Two ACES: transient ischemic attack work-up as outpatient assessment of clinical evaluation and safety. Stroke. 2011;42(7):1839-1843.
- Sanders LM, Srikanth VK, Jolley DJ, et al. Monash transient ischemic attack triaging treatment: safety of a transient ischemic attack mechanism-based outpatient model of care. Stroke. 2012; 43(11):2936-2941.
- Asimos AW, Johnson AM, Rosamond WD, et al. A multicenter evaluation of the ABCD2 score’s accuracy for predicting early ischemic stroke in admitted patients with TIA. Ann Emerg Med. 2010;55(2):201-210.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331-337.
- Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006;354(16):1706-1717.
- SPS3 Investigators; Benavente OR, Hart RG, McClure LA, Szychowski JM, Coffey CS, Pearce LA. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N Engl J Med. 2012;367(9):817-825.
- Diener HC, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. The Lancet. 2004. 364(9431):331-337.
- Lee M, Saver J, Hong KS, Rao NM, Wu YL, Ovbiagele B. Risk- benefit profile of long-term dual- versus single-antiplatelet therapy among patients with ischemic stroke: a systematic review and meta-analysis. Ann Intern Med. 2013;159(7):463-470.
- Shinohara Y, Katayama Y, Uchiyama S, et al. Cilostazol for prevention of secondary stroke (CSPS 2): an aspirin-controlled, double-blind, randomised non-inferiority trial. Lancet Neurol. 2010;9(10):959-968.
- SOCRATES trial. Web site. http://www.clinicaltrials.gov/show/ NCT01994720. Accessed September 1, 2014.
- Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011; 365(11):981-992.
- Connolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011;364(9):806-817.
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139-1151.
- Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093-2104. 64.
- Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891. 65.
- Diener HC, Eikelboom J, Connolly SJ, et al. Apixaban versus aspirin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a predefined subgroup analysis from AVERROES, a randomised trial. Lancet Neurol. 2012;11(3): 225-231.
- Clinical Policy: Use of Intravenous tPA for the Management of Acute Ischemic Stroke in the Emergency Department. Ann Emerg Med. http://www.acep.org/workarea/DownloadAsset.aspx?id=89978
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331-337.
- Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006;354(16):1706-1717.
- SPS3 Investigators; Benavente OR, Hart RG, McClure LA, Szychowski JM, Coffey CS, Pearce LA. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N Engl J Med. 2012;367(9):817-825.
- Diener HC, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. The Lancet. 2004. 364(9431):331-337.
- Lee M, Saver J, Hong KS, Rao NM, Wu YL, Ovbiagele B. Risk- benefit profile of long-term dual- versus single-antiplatelet therapy among patients with ischemic stroke: a systematic review and meta-analysis. Ann Intern Med. 2013;159(7):463-470.
- Shinohara Y, Katayama Y, Uchiyama S, et al. Cilostazol for prevention of secondary stroke (CSPS 2): an aspirin-controlled, double-blind, randomised non-inferiority trial. Lancet Neurol. 2010;9(10):959-968.
- SOCRATES trial. Web site. http://www.clinicaltrials.gov/show/ NCT01994720. Accessed September 1, 2014
- CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011; 365(11):981-992.
- Connolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011;364(9):806-817.
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139-1151.
- Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093-2104. 64.
- Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011; 365(11):981-992.
- Connolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011;364(9):806-817.
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139-1151.
- Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093-2104. 64.
- Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891. 65.
- Diener HC, Eikelboom J, Connolly SJ, et al. Apixaban versus aspirin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a predefined subgroup analysis from AVERROES, a randomised trial. Lancet Neurol. 2012;11(3): 225-231.
- Clinical Policy: Use of Intravenous tPA for the Management of Acute Ischemic Stroke in the Emergency Department. Ann Emerg Med. http://www.acep.org/workarea/DownloadAsset.aspx?id=89978






2 thoughts on “Updates on TIA”
Pingback: Global Intensive Care | Updates on TIA
Thanks for this nice review. The recently published POINT trial gives some more information about dual anti-platelet therapy in the acute phase after a TIA. Of course the trial had mixed findings and the treatment remains controversial.