
Authors: Cameron Jones, MD, MPH (EM Resident Physician, Northwestern Memorial Hospital, Chicago, IL) and Dana Loke, MD (Clinical Instructor and Medical Education Fellow, Department of Emergency Medicine, Northwestern Memorial Hospital, Chicago, IL) // Reviewed by: Alexander Y. Sheng, MD, MHPE (@TheShenger); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case
Emergency Medicine Services (EMS) arrives with a 63-year-old male with a history of head/neck cancer, s/p tracheostomy, in respiratory distress. His initial oxygen saturation was 82%, which improved to 87% after EMS applied oxygen to his face and stoma. Upon arrival, the patient is sleepy but arousable, receiving oxygen by non-rebreather on the face and BVM at his stoma. As staff begin placing him on the monitor, you note a medical alert bracelet on the patient that informs you he has had a laryngectomy. How does this change your approach and what are your next steps?
Background
The primary indication for total laryngectomy is laryngeal cancer and thus, the vast majority of post-laryngectomy patients the emergency physician (EP) sees will have a history of head and neck cancer. Other, less common, indications for laryngectomy include severe laryngeal stenosis or chronic aspiration refractory to other treatments.1
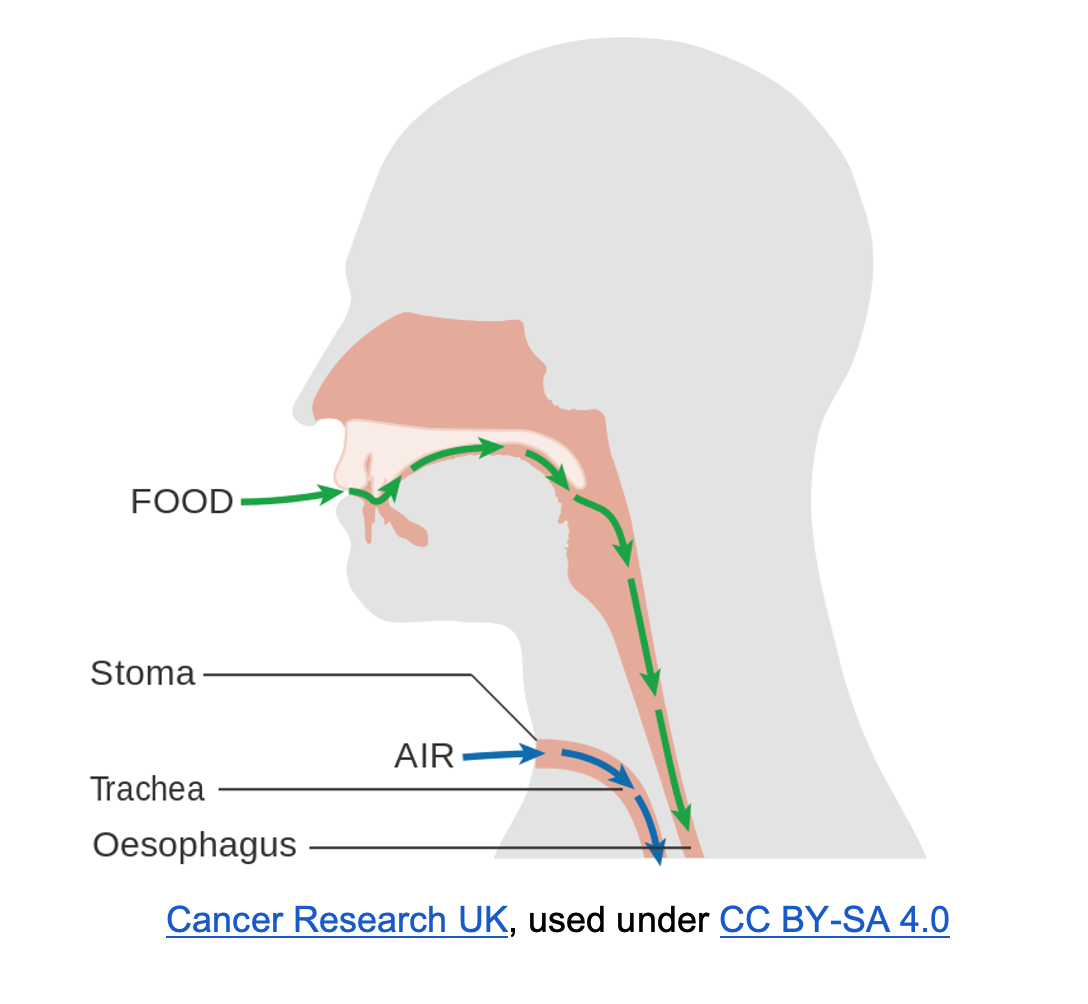
Total laryngectomy involves surgical removal of the entire larynx resulting in discontinuity between the trachea and oropharynx. With removal of the larynx, the end of the patient’s proximal trachea is mobilized and brought to the skin to create a stoma in the lower anterior neck. Therefore, patients who have undergone laryngectomy are obligate stoma-breathers and can only be oxygenated via the stoma.1,2 An understanding of the anatomy involved can help provide clues to recognizing that a patient has undergone a laryngectomy rather than a simple tracheostomy if unable to obtain history from the patient or family members. Post-laryngectomy patients will typically have larger stomas and examination of the stoma and tracheal inlet will reveal a blind ending superior to the stoma.3
What devices or tubes might ED physicians encounter with laryngectomies?
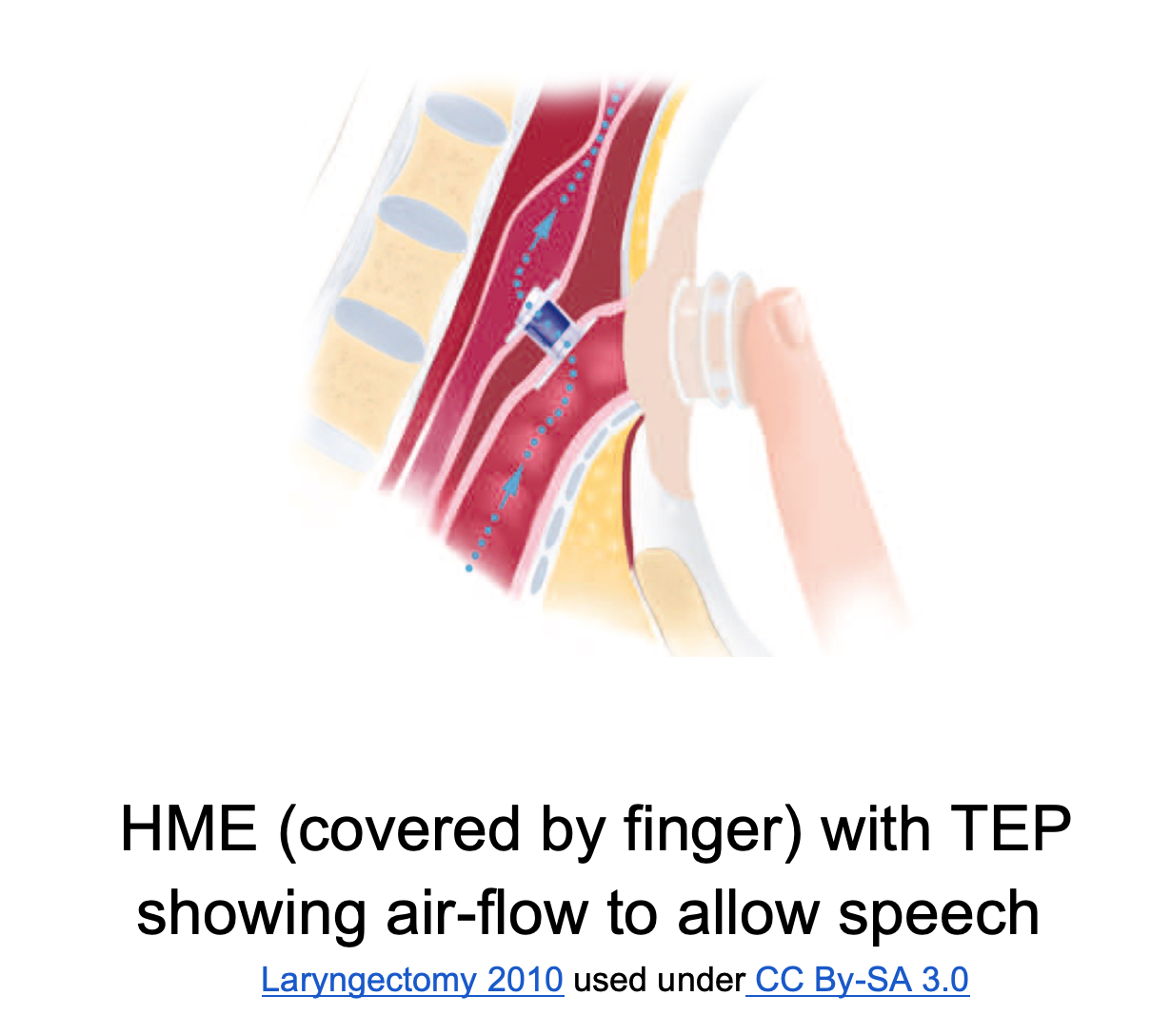
Patients will most commonly have a simple heat/moisture exchanger (HME) over the stoma to help with humidification. These often look like a flat button with a housing to hold it in place, and these devices can usually be easily removed. Additionally, many patients with laryngectomies will have a tracheo-esophageal prosthesis (TEP), a one-way valve between the superior trachea and the patient’s esophagus to allow speech and which can usually be visualized through the stoma on the posterior-superior trachea. Finally, some patients may have a soft, flexible tube in place to maintain the stoma tract, especially in the initial days or weeks after surgery.2,4 These silicone tubes, often referred to as Larytubes (though this is actually a commercial name) can be attached directly to an HME.5
Less commonly, patients may have an adjunctive airway such as a tracheostomy tube or an endotracheal tube in place, which can make it more challenging to initially recognize a laryngectomy stoma vs a tracheostomy. Understanding and trouble-shooting various tracheostomy tubes is outside the scope of this article (please refer to this previous emDocs post on airway emergencies and this emDocs and CORE EM post on tracheostomy care).
How can providers differentiate a laryngectomy from a tracheostomy?
In many ways, ED care for the patient with a laryngectomy relies primarily on staff recognizing and appreciating their distinction from tracheostomy patients. Unfortunately, many emergency personnel struggle to recognize the anatomical differences and how this impacts their care.6,7 Most patients will be able to provide this information themselves if they are stable enough to do so. While laryngectomy patients lose the ability to speak using their native vocal cords due to removal of the voicebox, those with TEPs or electrolarynxes can learn to speak using these devices. It is important to have a patient-centered approach and first attempt to communicate directly with them via one of these methods or an alternative, such as writing.8 Family or friends accompanying the patient can also provide valuable information. If unable to obtain information from the patient, a relation, or electronic medical records, physical inspection may also alert providers that the patient has had a laryngectomy. Look for medical alert bracelets or medical cards many patients are given after their surgery.3 Many of these patients may initially receive supplemental oxygen at both the face and stoma while gathering further history, and the absence of end-tidal capnography (EtCO2) waveform measured at the face indicates absence of upper airway respirations. Next, inspect the stoma site itself. Laryngectomy patients will typically have a larger stoma, and palpation or visualization of trachea superior to the stoma will reveal a blind pouch in post-laryngectomy patients.2-4 The presence of a TEP also indicates a laryngectomy.
What are the most common complications after laryngectomy?
Pharyngocutaneous fistulas are one of the more common post-op issues, especially in patients who have undergone pre-operative radiation therapy. These fistulas can present with salivary leakage into the soft tissues and erythema around the patient’s stoma or incision or worsening tenderness at the incision site, most often between 7-10 days after surgery. Wound dehiscence and local hematomas can also occur, which, depending on their severity, may require otolaryngology (ENT) consultation.3,9,10
However, for the EP, the most important complications to recognize are those that may lead to hypoxia or ventilatory failure. Given the absence of airway exchange through the nose and mouth, patients with laryngectomies are especially susceptible to obstruction of the airway. If a trach device is present, removing the entire device or the inner cannula (if a mature stoma) and passing a suction catheter can often alleviate this obstruction. TEPs can occasionally become dislodged and partially obstruct a patient’s distal trachea or proximal bronchi. A visible tracheo-esophageal fistula site with no button/prosthesis in place on exam should prompt this consideration, which can typically be diagnosed with x-ray.4 For those patients with thick secretions in the distal trachea or proximal small bronchi, small aliquots (around 5 cc) of normal saline expressed through the stoma can help break up these secretions and induce a cough reflex to help them.
Bleeding around the stoma site in tracheostomy patients should be immediately addressed, as it may be the herald of significant hemorrhage. Tracheo-innominate fistulas (TIFs) are one of the most feared complications of tracheostomies. However, TIFs are extremely rare in laryngectomy patients due to their altered anatomy and the absence of a trach tube in place for any significant period of time, thus preventing erosion into the innominate artery.10 Instead, providers should be alert for carotid-blowout syndrome (CBS), in which the carotid or branch vessels are threatened or eroded, which is more common in irradiated patients due to poor tissue integrity. The first sign may be new bruising/hematoma, or oozing from the neck or intra-orally. If suspected, a secure airway (ideally via intubation of the stoma with cuffed endotracheal tube) should be established immediately as bleeding can quickly lead to aspiration and stoma/airway compromise. Providers should activate massive transfusion protocols and perform resuscitation as they would for other significant hemorrhage, and direct pressure should be applied over any external bleeding and intraorally using packing and forceps. Definitive management will require surgical treatment or IR embolization, and therefore, specialty consultation should occur early.11,12
Resuscitating the patient with a laryngectomy
In the crashing patient, especially one with altered anatomy that will be less familiar to most ED personnel, it is important to have an algorithmic approach to allow rapid and systematic assessment and stabilization (see figure below). As noted above, the most important step in this evaluation is recognizing that a patient has a laryngectomy stoma rather than a tracheostomy. This recognition will allow all providers to focus on oxygenating, supporting and troubleshooting the stoma rather than attempting to ventilate or establish a definitive airway via the mouth and upper airway. Even if the patient is found to have a tracheostomy, rather than a laryngectomy, it is also important to know why their tracheostomy was performed. Some patients with tracheostomies have essentially non-patent upper airways due to severe stenosis or other anatomic abnormalities and must be functionally treated as laryngectomy patients in the ED. However, there is little harm in applying oxygen to the face/nose and stoma initially while gathering information and making this determination.2 As with any unstable patient, you should try to mobilize resources and personnel as quickly as possible. If given advance notice by a pre-arrival call, providers should gather all necessary equipment (Table 1), ensure appropriate nursing/tech staff is available, and notify respiratory therapy (RT) staff if available.13 Some larger academic hospitals may have trach specialists among their RTs, and, in a facility with ENT available, they should be consulted as soon as possible in the unstable post-laryngectomy patients.

Once you have recognized the patient has a laryngectomy, all oxygenation efforts should be focused on the patient’s stoma. A bag-valve mask fitted with a pediatric mask or a supraglottic airway device, such as a laryngeal mask airway (LMA), will allow for a good seal around the stoma (see video linked below).14 While providing oxygen and ventilatory support as needed, providers should begin their assessment of the stoma itself.
Video from National Tracheostomy Safety Project on Stoma Ventilation
This process begins with examining the devices in or around the stoma and attempting to determine how recently the patient’s laryngectomy was performed. With tracheostomy tubes, traditional teaching emphasizes that EPs and emergency responders should try to avoid removal of in-situ devices or re-cannulation of the stoma within 7-10 days of surgery, as the tract may not yet be mature. Most post-laryngectomy patients remain hospitalized for around a week and are not typically sent home with a tracheostomy tube in place.9 However, the presence of sutures in place around the stoma site may suggest a more recent procedure, and, if possible, in these scenarios exploration of the stoma and airway should be performed under direct fiberoptic visualization or with specialty consultants at the bedside.15
Next, attempt to determine the patency of the stoma or devices present. HMEs or similar button devices should be removed, and if the patient does have a trach in place, the inner cannula should be removed. Next, attempt to gently pass a suction catheter or bougie through the stoma, trach tube, or patency tube. If a suction catheter cannot be passed through a tube in place, any present cuff should be deflated and the tube should be removed. In general, patency at the stoma itself is less often an issue than with the tracheostomy patient, and, once all cuffs have been deflated and devices removed, reassess by listening and feeling at the stoma for respirations and using end-tidal capnography. If the patient is breathing and oxygen levels have stabilized, continue applying oxygen at the stoma and continue your usual assessment to determine alternative causes of respiratory distress.2,3 If encountering obstruction in the proximal respiratory tract, use of a fiberoptic scope (reusable or single-use bronchoscopes or shorter nasopharyngeal scopes) can be extremely helpful for direct visualization of the airway.16
If at any point the patient decompensates, stops breathing, or arrests, a definitive airway must be established via the stoma. For the EP, the fastest and safest way to do so will most likely be via intubation of the stoma with an endotracheal tube (ETT). A size 6.0 ETT will easily pass through most stomas and should be the first size in most adults. Placement of a tracheostomy tube is likely to be similarly effective, though most EPs will find use of an ETT to be more familiar and also eliminates the cognitive load of choosing a trach tube size. Intubation over a bougie or fiberoptic will allow the provider to maintain a ready tract into the airway and can allow for rapid down-sizing if meeting resistance with a 6.0 tube. The tube should only be advanced a few centimeters past the cuff, as it is very easy to accidentally pass into a mainstem (similar to when performing a cricothyrotomy).3,15

Take-Home Points
- Patients who have undergone laryngectomies have no connection between their lower and upper airway and can only be oxygenated and ventilated via their stoma.
- Some tracheostomy patients must be functionally treated as laryngectomy patients, as they have a very limited or non-patent upper airway due to stenosis, mass, etc.
- In all patients with anterior neck stomas who present to the ED, initially apply O2 to both the face and neck but immediately attempt to determine upper airway patency via history, examination of the stoma, or absence of end-tidal CO2 waveform at the face.
- Emergency oxygenation at a tracheal stoma is best applied with a BVM fitted with a pediatric facemask or with a laryngeal mask airway (LMA).
- For the patient with a laryngectomy in respiratory distress, the primary tasks are to apply supportive oxygen, assess stoma patency and establish a definitive airway if necessary.
- If the patient stops breathing, arrests, or decompensates, intubate the tracheal stoma using a 6.0 ETT over a bougie or fiberoptic device.
References
- Ceachir O, Hainarosie R, Zainea V. Total Laryngectomy – Past, Present, Future. Mædica. 2014;9(2):210.
- Mcgrath, BA, Atkinson D, Moore JA, Bates L. Comprehensive Tracheostomy Care. National Tracheostomy Safety Project. 2013. Accessed September 10, 2021. https://www.tracheostomy.org.uk/storage/files/Comprehensive%20Tracheostomy%20Care.pdf
- Townsley RB, Baring DEC, Clark LJ. Emergency department care of a patient after a total laryngectomy. Eur J Emerg Med. 2014;21(3):164-169. doi:10.1097/MEJ.0B013E32835ED735
- Bryant CD. Complications of Airway Devices. In: Tintinalli J.E., & Ma O, & Yealy D.M., & Meckler G.D., & Stapczynski J, & Cline D.M., & Thomas S.H.(Eds.), Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw Hill; 2020. Accessed September 22, 2021. https://accessmedicine-mhmedical-com.turing.library.northwestern.edu/content.aspx?bookid=2353§ionid=221180267
- University of Mississippi Medical Center. Laryngectomy: What to Expect. Accessed September 23, 2021. https://www.umc.edu/Healthcare/ENT/Patient-Handouts/Adult/Head_Neck/HN%20_PDF/Laryngectomy%20_What%20to%20Expect_Fin.pdf.
- Darr A, Dhanji K, Doshi J. Tracheostomy and laryngectomy survey: do front-line emergency staff appreciate the difference? 2021. doi:10.1017/S0022215112000618
- Whitcroft KL, Moss B, Mcrae A. ENT and airways in the emergency department: national survey of junior doctors’ knowledge and skills. J Laryngol Otol. 2016;130(2):183-189. doi:10.1017/S0022215115003102
- Lee MT, Gibson S, Hilari K. Gender Differences in health-related quality of life following total laryngectomy. International Journal of Language & Communication Disorders. 2010;45(3):287-294.
- Goepfert RP, Hutcheson KA, Lewin JS, et al. Complications, hospital length of stay, and readmission after total laryngectomy. Cancer. 2017;123(10):1760-1767. doi:10.1002/CNCR.30483
- Hasan Z, Dwivedi RC, Gunaratne DA, Virk SA, Palme CE, Riffat F. Systematic review and meta-analysis of the complications of salvage total laryngectomy. European Journal of Surgical Oncology. doi:10.1016/j.ejso.2016.05.017
- Miguel C, Estomba C, Alberto F, et al. Carotid blowout syndrome in patients treated by larynx cancer. Braz J Otorhinolaryngol. 2017;83(6):653-658. doi:10.1016/j.bjorl.2016.08.013
- Carotid Artery Rupture Precautions. Head and Neck Protocols. University of Iowa Healthcare. 2017. Accessed September 24, 2021. https://medicine.uiowa.edu/iowaprotocols/carotid-rupture-precautions.
- Morris LL, Whitmer A, Mcintosh E. Tracheostomy care and complications in the intensive care unit. Crit Care Nurse. 2013;33(5):18-30. doi:10.4037/CCN2013518
- Bhalla RK, Corrigan A, Roland NJ. Comparison of two face masks used to deliver early ventilation to laryngectomized patients. Ear Nose and Throat Journal 2004; 83: 414.
- Long B, Koyfman A. Resuscitating the tracheostomy patient in the ED. American Journal of Emergency Medicine. doi:10.1016/j.ajem.2016.03.049
- McGrath, B. A., Bates, L., Atkinson, D., & Moore, J. A. (2012). Multidisciplinary guidelines for the management of tracheostomy and laryngectomy airway emergencies. Anaesthesia, 67(9), 1025–1041. https://doi.org/10.1111/j.1365-2




