Author: Anna Pickens, MD (@AnnaEMin5, Creator of EMin5) // Edited by: Alex Koyfman, MD (@EMHighAK), Brit Long, MD (@long_brit), and Manpreet Singh, MD (@MprizzleER)
Welcome to this week’s edition of EMin5 by Dr. Anna Pickens. Today: Meales! This is a hot topic in the news over the last month, especially in certain New York neighborhoods where an outbreak is occuring. And it is up to YOU in the ED to help stop the spread! Read on…
Video:

Measles is one of the classic pediatric febrile viral exanthems – each has it’s own pattern to look for!

Measles used to be pretty common before the Nation Wide vaccine program in 1965.

But we still get occasional outbreaks within communities in the US. Usually in unvaccinated patients that have traveled to another area of outbreak.

Although rare in the US, Measles is still a significant cause of morbidity/mortality worldwide.
Measles is HIGHLY contagious, with a 90% transmission rate to unvaccinated contacts.

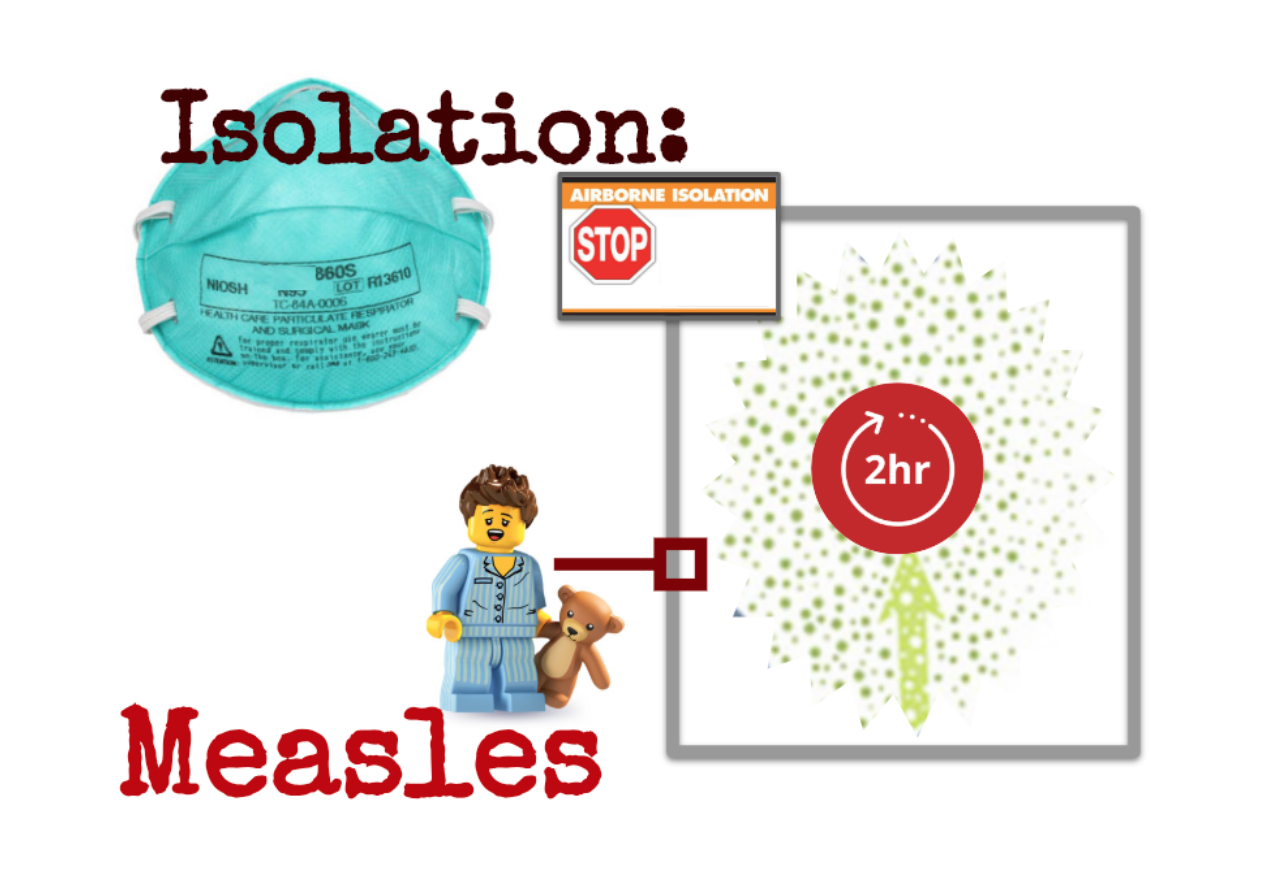
Part of the reason for this is that the virus stays alive in the air for up to 2 HOURS!
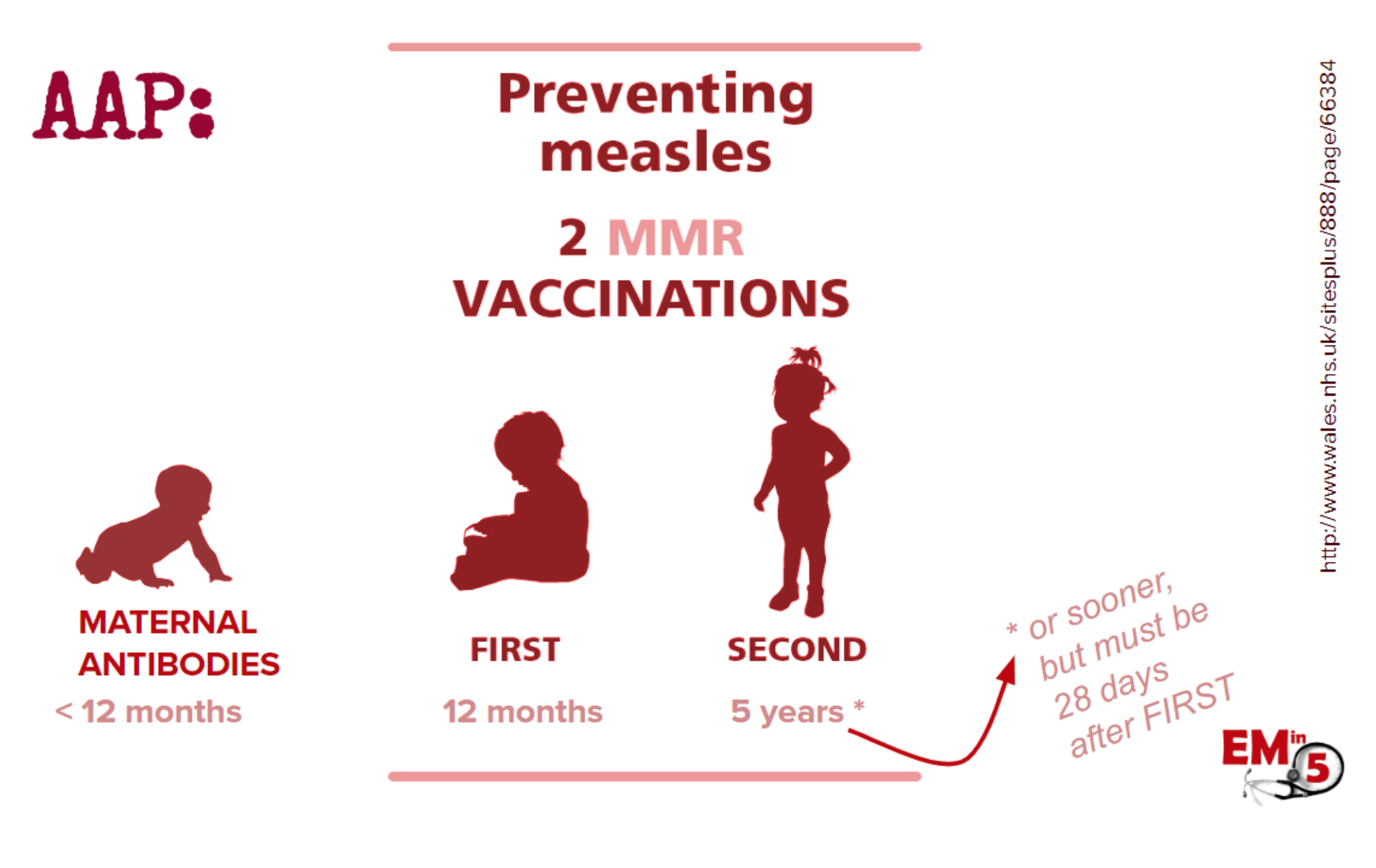
The vaccine schedule recommended by the AAP is 2 shots – the first around 12 months old and the second around 5 years old. Before that babies are somewhat protected by maternal antibodies (If the mom has had measles or is vaccinated, that is).
If your patient is so unlikely as to have gotten measles, you can expect the some of the following symptoms:
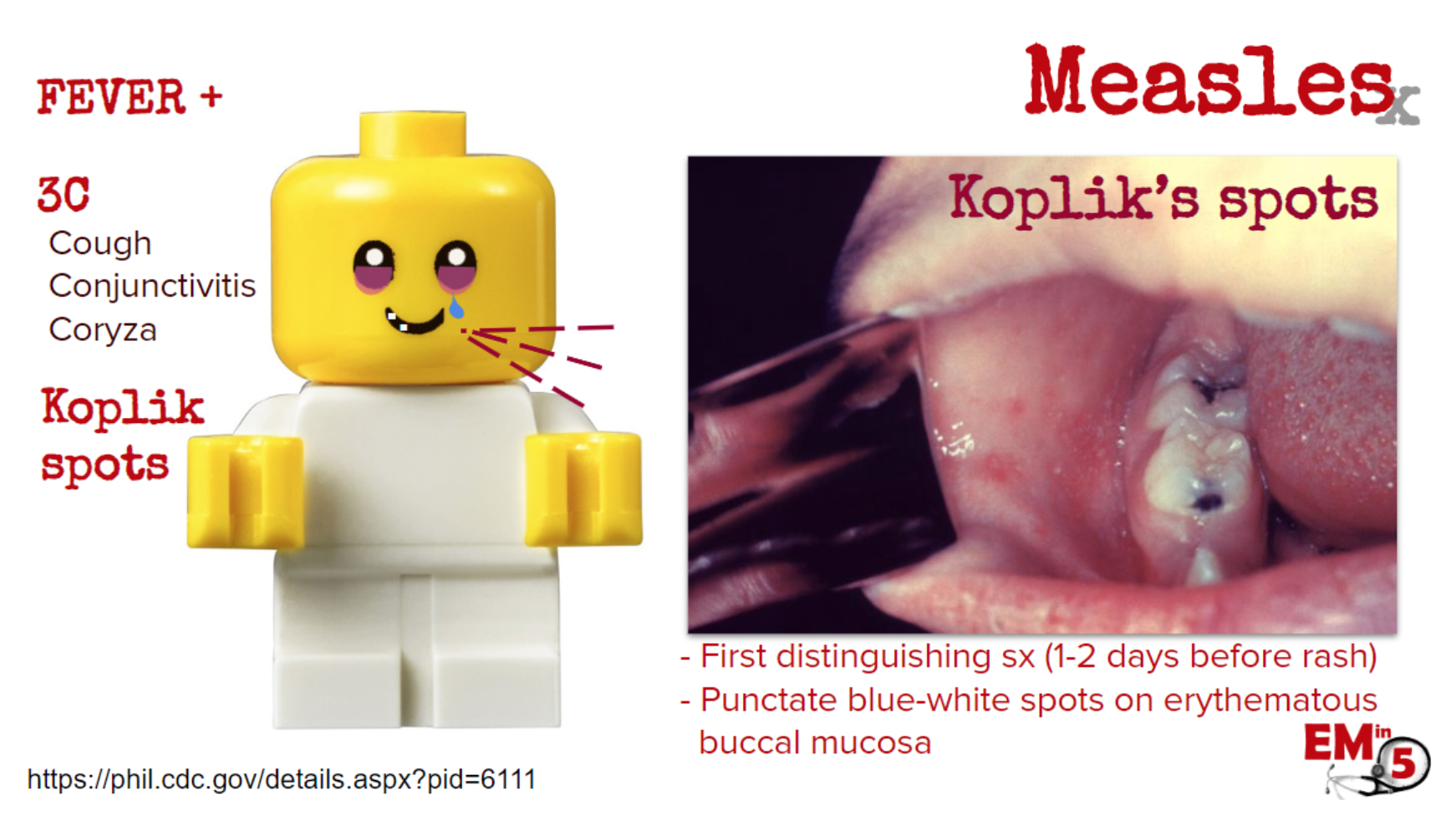
A few days of fever, viral-like syndrome, and the “3 C”s. You may also see some Koplik spots, which are a potentially early diagnostic finding, as they are pathognomonic for measles and may be present before the rash.
The rash then spreads from the hairline, to the face, to the trunk to the limbs.


It starts as discrete maculopapular rash, but can become more confluent:

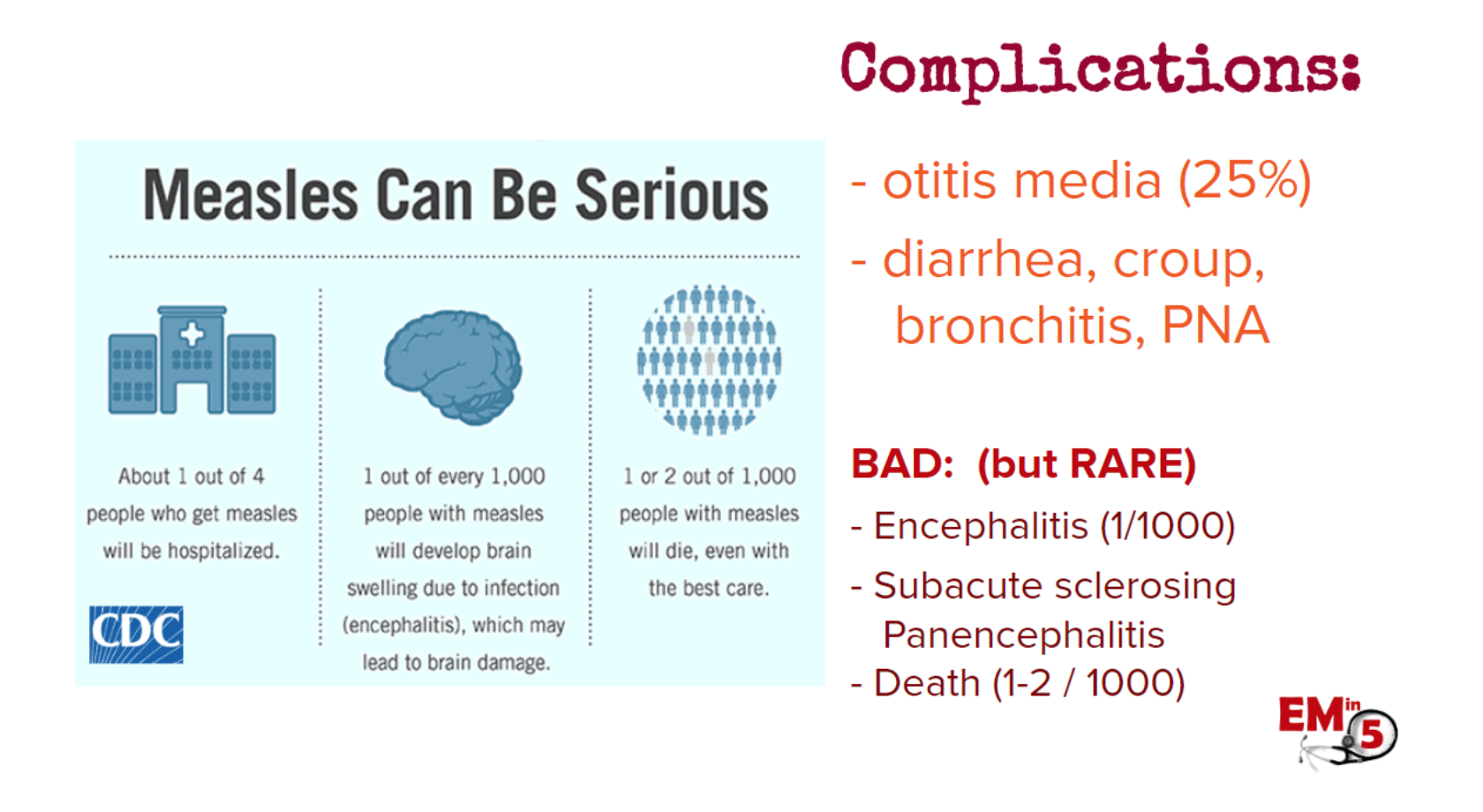
Complications are rare, but can be serious. Those at higher risk for complication are <5yo, >20yo, immunocompromised and pregnant.
Here is the typical timeline for measles:

The treatment for measles is mostly supportive care, so our main job in the ED is to help prevent spread.

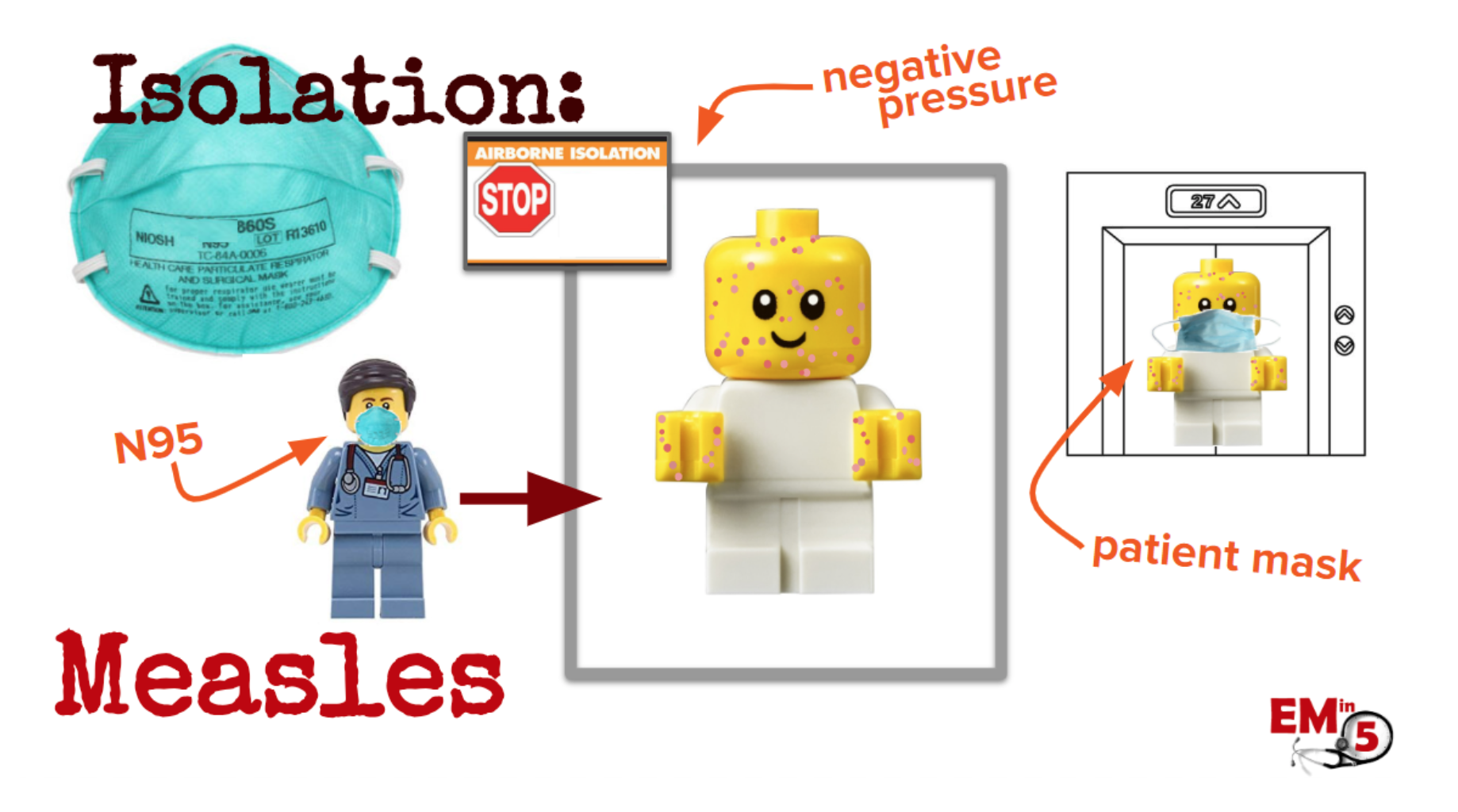
If a patient comes in who you suspect may have measles, you need to place them in airborne isolation. This means a negative pressure room, staff must wear an N-95 mask, and if patients are transported, they must also wear a patient mask.
And because that virus can stay alive in the air for 2 hours, no one else should be placed in that room for 2 hours after the measles patient has left. Think about how that can affect your waiting room and hallways, too! Yikes!
If you suspect measles in a patient, you must notify the CDC and your Local Health Dept, and for population health purposes you must confirm the measles by getting a blood sample and throat swab.

Next, in order to help prevent spread, we need to think about who has come in contact with the measles patient while they have been contagious. Patients are contagious for 4 days before and 4 days after the first day of rash.

Then you need to confirm with all the family, friends, schoolmates, healthcare workers or other exposed people if they have had 2 documented MMR vaccines. “I think so” isn’t good enough.
If they have, or were born before 1957 (ie, they’ve had measles as a kid), then there is nothing further to do, they are immunized!
If not, they need to be given a post-exposure prophylaxis live measles vaccine. If they get it within 72 hours of exposure, they should protected. If they can’t get the live vaccine or are otherwise high risk (<6 months old, pregnant, immunocompromised), they need to be given the measles Immunoglobulin (IG). If they get it within 6 days of exposure, they should be protected.

Unimmunized contacts that get the vaccine within 72 hours are good to go back to school or work (as long as they are asymptomatic, of course).
However, if they are healthcare workers, refuse the PEP, or are high risk and got the IG, they must be in isolation (in their home) for 21 days! (per the CDC) Serious stuff! Get vaccinated!

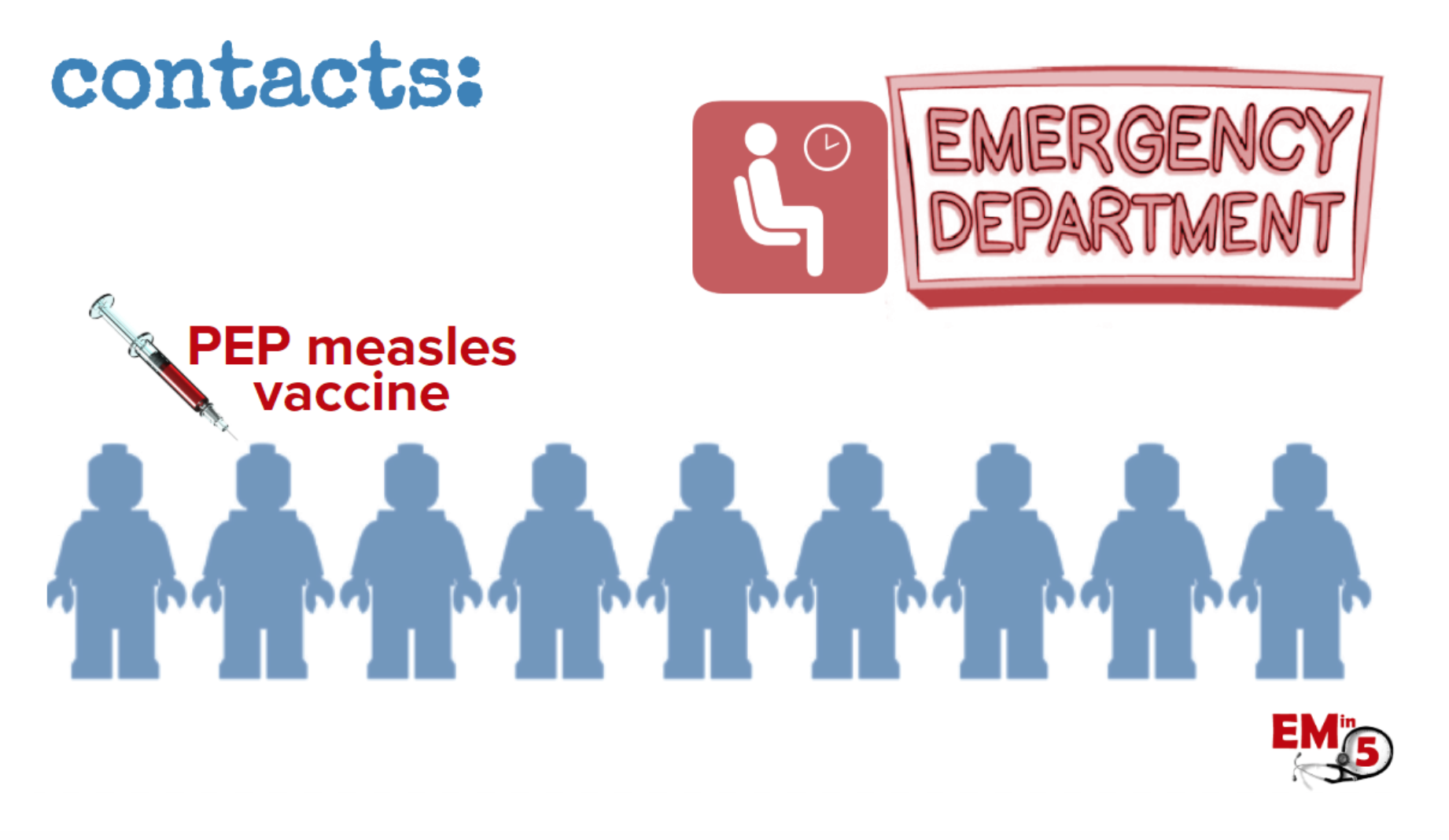
And make sure to think about anyone the measles patient came in contact with at the hospital – patients in your waiting room, the ED, the hallways, staff, family members, etc.
If any of them are unimmunized and were in the area of the measles patient within 2 hours, they need the PEP live measles vaccine BEFORE they leave the ED in order to prevent spread!
Suggested/Further Reading:
CDC:
- https://www.cdc.gov/infectioncontrol/basics/transmission-based-precautions.html
- https://www.cdc.gov/vaccines/pubs/pinkbook/meas.html
Pediatric EM Morsels:
Don’t Forget the Bubbles:




