
Authors: Jacob Tauferner, MD (EM Resident Physician, UTSW/ Dallas, TX); Mihir Patel, MD (EM Attending Physician, Dallas, TX) // Reviewed by: Sophia Görgens, MD (EM Physician, Northwell, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 24-year-old male presents to the ED from a mixed marital arts competition after being struck on the side of the right head by a fist earlier today. The patient denies any loss of consciousness, neck pain, vomiting, or use of blood thinners. His vital signs include BP 133/82, HR 76, T 97.5, RR 15, SpO2 99% on room air. On exam there is no periorbital ecchymosis, eye trauma, hemotympanum, facial tenderness, or trismus. On evaluation of the right ear a fluctuant and tender area is noted to the superior portion of the ear. The area of fluctuance measures approximately 3 cm in diameter.

What is the diagnosis?
Answer: Auricular hematoma
Epidemiology:
- More common in contact sports such as wrestling, mixed martial arts, ultimate fighting, rugby, and boxing.[1]
- In a survey of college wrestlers, the incidence of auricular hematoma was found to be 52% for those who do not wear headgear versus 26% who wore ear protection.[2]
Anatomy:
- The auricle is composed of skin, subcutaneous tissue, musculature, and the perichondrium which supplies blood to underlying cartilage.[3]
- An auricular hematoma is a collection of blood between the perichondrium and underlying cartilage.[3]
- Areas of cartilage in the ear include:[3]
- tragus
- helix
- antihelix
- triangular fossa
- cymba concha
- concha cavum
- Main blood vessels that supply the ear consist of the superficial temporal and posterior auricular artery.[1]
- Trauma to the ear can cause the perichondrium and vasculature to be damaged, causing separation from the underlying cartilage and resulting in a potential space for blood to accumulate. This results in ischemia of the adjacent cartilage and venous congestion that can result in histologic changes and cartilage deformity.[3]

Clinical Presentation:
- Typically caused by trauma (earring placement to ear, but more commonly by direct blow to the ear).[3]
- Symptoms include mild to moderate pain, paresthesia, and overlying erythema or ecchymosis.[4]
- Exam demonstrates contour irregularity of ear with swelling and fluctuant area overlying the ear’s cartilaginous portions.[4]
- May occur on posterior aspect of the ear.[4,5]
- Risk of necrosis is higher if it’s present on anterior and posterior aspects.[5]
- 24 hours post-trauma, the blood will clot and the swelling may become firmer.[4]
- It’s important to rule out other serious processes including serious head/neck injuries, loss of consciousness, amnesia, tympanic membrane rupture, hemotympanum.[6]
Management/Treatment:
- If the hematoma is more than 7 days old organization and formation of granulation tissue is likely and patient warrants referral to ENT
- Recommended management depends on the size of the hematoma
- < 2 cm in size and < 48 hours old: needle aspiration with 18 gauge.[1,4]
- > 2 cm in size, > 48 hours old, difficulty with aspiration of hematoma: incision and drainage.[1,4]
Supplies should consist of an 11 blade or 15 blade scalpel and/or an 18-gauge needle with a 10 cc syringe, suction canister, tubing and suctioning instrument (Frasier), a hemostat, toothed forceps, suture supplies with scissors, bolster material, local anesthetic, and local skin cleansing material.[3]
- The patient’s head should be turned so that the unaffected ear is facing towards the stretcher and the affected ear is towards the ceiling.
- The ear is cleaned with a local cleansing agent such as povidone-iodine.
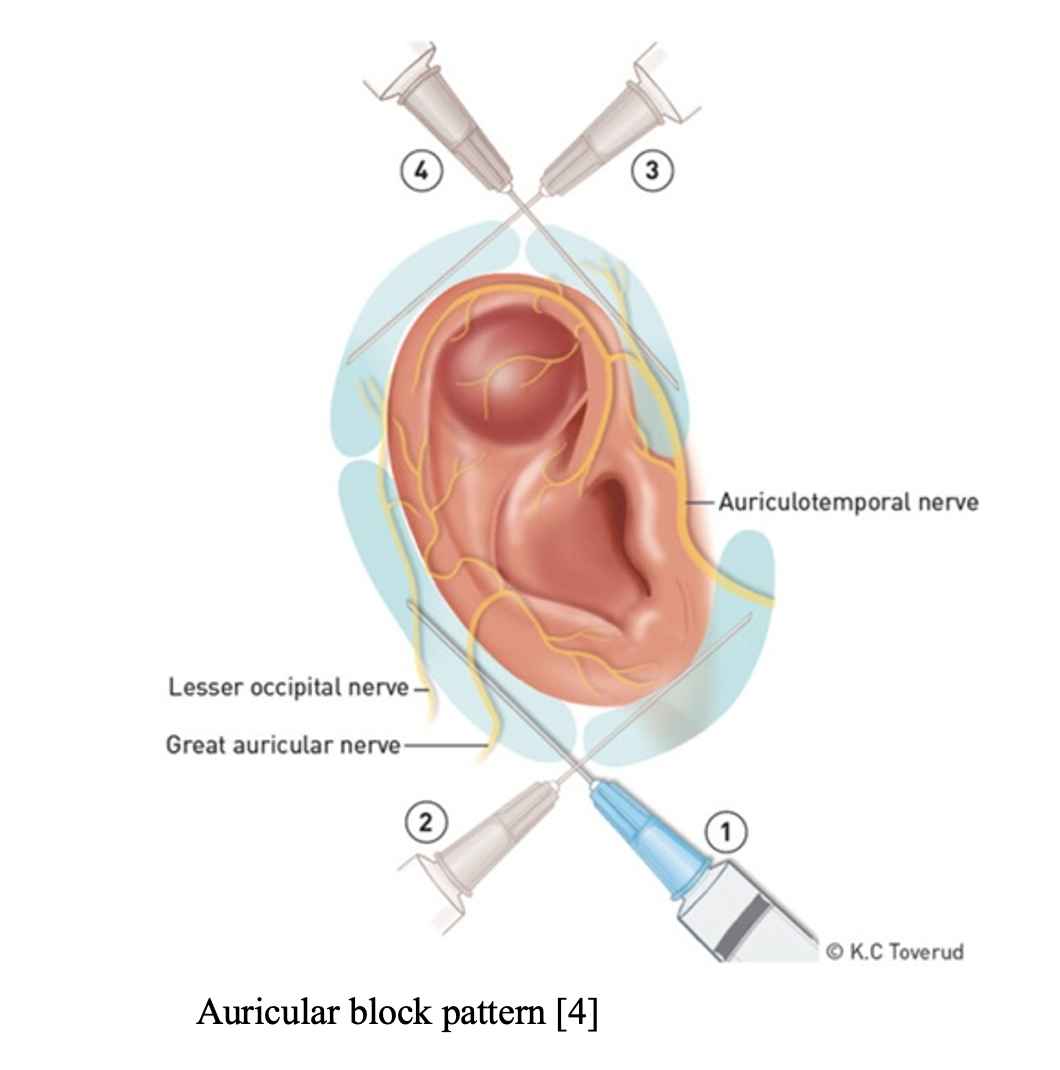
- Local anesthesia should then be injected or applied topically to the site where the incision or aspiration will be performed.
- The anesthetic can be injected in an auricular block pattern or directly into the site of the auricular hematoma.[1,4]
Incision and Drainage
- Next make a linear incision overlying the swelling or hematoma.[3] The goal of the incision is to drain the fluid collection. Incision in areas of concavity will heal with a more aesthetically pleasing results compared to areas of convexity.
- Use hemostats and suction to evacuate the hematoma.
- Irrigate with normal saline.
- Apply bolster dressing. It closes the dead space or potential space where the hematoma formed. When using dental rolls as a bolster, two rolls should be used. Place each roll so it to runs parallel with the incision line on either side of the ear. Place two vertical mattress sutures through dental rolls.[3] A permanent suture material such as nylon is appropriate. Adequate bolster is applied when there is no potential space for accumulation of hematoma
- Apply bacitracin to incision site post procedure.[1,4]
Aspiration
- Insert an 18-gauge needle at the base of the hematoma into or through the cartilage.[4]
- Aspirate the most fluctuant part while milking the hematoma
- If aspiration is difficult, then blood is likely fully or partly coagulated. I&D should then be considered.[4]
- Apply pressure for 5 to 10 minutes, then place a pressure dressing
- Pressure dressing: place sterile gauze posterior to the ear, mold sterile petrolatum-impregnated gauze or saline-soaked cotton balls within the contours of the auricle, place sterile gauze over entire ear, and then wrap the entire head with sterile rolled gauze.[3,10,12]
- There are several variances of bolster and pressure dressings used, but the goal is the same: eliminate the potential space for fluid accumulation.[1]
Disposition:

- A 7-10 day course of prophylactic antibiotics is recommended due to limited vascular supply.[7]
- Referral to ENT in case additional drainage of the hematoma is needed.[1]
- All patients should refrain from activity that places their ear at risk for additional trauma until the ear is healed.[9] Return to sports can occur as early as seven days after the initial injury if the hematoma does not reaccumulate.[10,11]
- Strongly advise athletes to wear protective headgear to prevent reinjury
- Patients warrant daily follow-up for three to five days to evaluate for reaccumulation of the hematoma or infection.[7]
- The bolster dressing and sutures can be removed after 5 to 7 days.[1]
Pearls:
- An auricular hematoma is a collection of blood in the cartilaginous portion of the ear usually secondary to trauma.
- If the hematoma is not drained it can cause disruption of blood supply to the cartilage and subsequent necrosis, as well as an increase in risk of infection.
- Hematomas over 7 days old warrant referral to plastic surgery or ENT.
- Incision and drainage is recommended for hematomas over 48 hours old and/or > 2 cm in size.
- Prophylactic antibiotics are recommended.


A 21-year-old man presents to the emergency department for pain and swelling in his ear beginning 3 days ago. He is a collegiate wrestler and participated in several matches at a regional wrestling meet the day before his symptoms began. He did not notice any specific injury during the matches but woke up the following morning to find his right ear swollen and painful. His symptoms have worsened since that time. He has no medical or surgical history and drinks alcohol socially on the weekends. Vital signs show no abnormalities. Physical examination shows the findings in the photo above. Which of the following is the most appropriate next step in management?
A) Bedside incision and drainage
B) Emergent consult to otolaryngology
C) Intra-auricular phenylephrine injection
D) Needle aspiration
E) Warm compresses and an oral antibiotic prescription
Answer: A
Auricular hematoma is a complication of trauma that occurs due to shearing forces to the ear. It is most common in wrestlers, boxers, and rugby players and presents as tender, anterior auricular swelling in the setting of trauma, such as this patient’s wrestling matches. It can occur in patients on anticoagulants with incidental trauma, but this is less common. Drainage of an auricular hematoma is necessary due to the relatively avascular nature of the ear, which makes it susceptible to necrosis, infection, and neocartilage formation. The latter may result in deformities (e.g.,cauliflower ear) as the new cartilage develops. There is debate surrounding the best form of procedural drainage of an auricular hematoma, though both needle aspiration and incision and drainage may be used. However, many authorities formally recommend incision and drainage over needle aspiration due to a reduced risk of re-expansion of the hematoma after the procedure. In this patient, incision and drainage is specifically indicated because of the time course (> 48 hours of symptoms) and size (> 2 cm). Needle aspiration is indicated for small hematomas (< 2 cm) that are < 24–48 hours old. More recently, the use of an angiocatheter has been introduced to the procedural management of larger auricular hematomas. This involves an initial needle aspiration but leaves an angiocatheter in place for 5 days to allow continued drainage of the hematoma. Prophylactic antibiotics with antipseudomonal and antistaphylococcal coverage are generally recommended. Complications of auricular hematoma include reaccumulation, infection, and deformity due to scarring.
Specialist involvement (B) (i.e., otolaryngology or plastic surgery) is reserved for auricular hematomas > 7 days old and generally occurs outpatient rather than as an emergency consult.
Intra-auricular injections (C) of any kind are not indicated in the management of auricular hematomas.
Needle aspiration (D) has historically been used and is still appropriate in cases of auricular hematomas < 2 cm and < 48 hours old.
Many cutaneous infections can be treated with antibiotics and warm compresses (E), but this regimen does not treat an auricular hematoma.




