
Author: Devin Morris, MD (EM Resident Physician, UTSW / Parkland Memorial Hospital); Colin Danko, MD (EM Attending Physician, UTSW / Parkland Memorial Hospital) // Reviewed by: Sophia Görgens, MD (EM Resident Physician, Zucker-Northwell NS/LIJ, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. He has been having “issues with [his] eyes” today and “not feeling quite right.” Vital signs include BP 165/83, HR 81, RR 18, SpO2 96%. On exam, you notice he has dysarthric speech, limb ataxia, and vertical gaze palsy, which he reports is new. You perform a NIHSS which scores a 3 for mild dysarthria and ataxia in two limbs. You pursue further work-up given his risk factors and presenting symptoms and obtain a CT head non-contrast with the following image:

What is the most likely diagnosis?
Answer: Basilar Artery Occlusion
Epidemiology:
- Basilar artery occlusion (BAO) is a subset of the posterior circulation strokes.
- Posterior circulation strokes are estimated to account for 20% of all strokes, with BAO accounting for ~1% of all strokes.2
- BAO has an estimated incidence of 4/100,000 people per year.3
Anatomy:
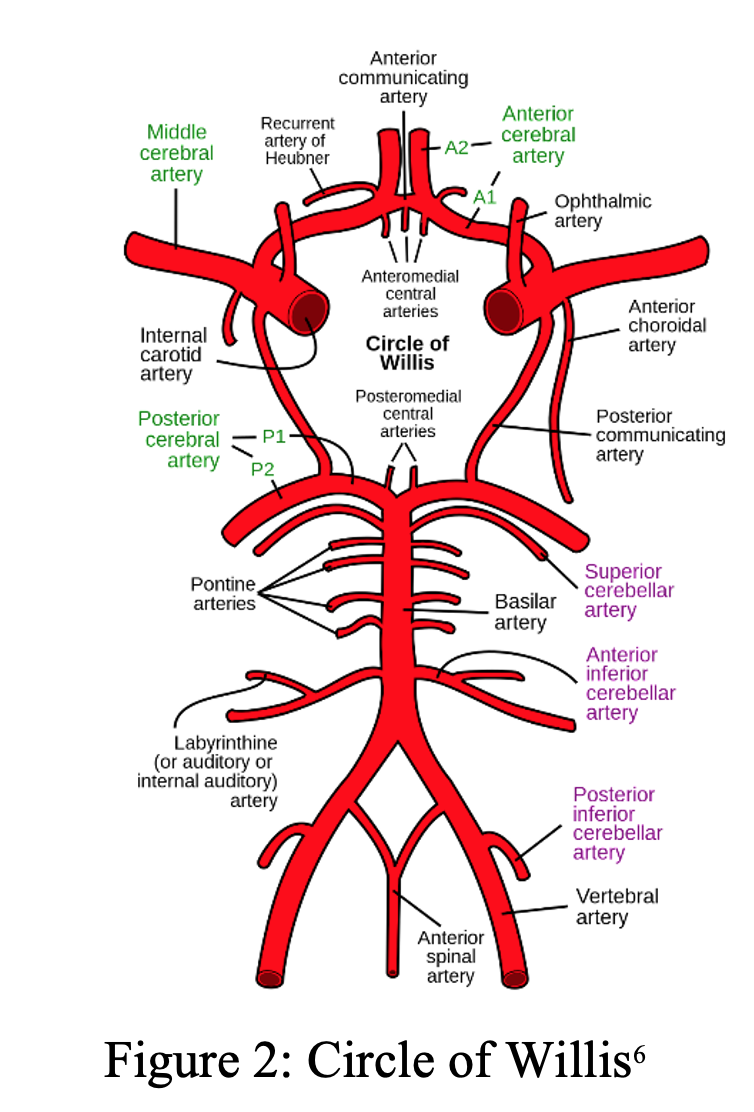
- The posterior circulation accounts for 20% of blood supply to the brain and originates from the vertebral arteries which merge to form the basilar artery which supplies the brainstem, thalami, cerebellum, and occipital lobes.4
- The basilar artery (BA) lies on the ventral surface of the pons and forms many perforating branches to supply a collateral network to the pons and midbrain.5
- The basilar artery can be subdivided into three segments:
- Proximal segment: from vertebral artery junction to anterior inferior cerebellar arteries (AICA)
- Middle segment: from AICA to the origin of superior cerebellar arteries (SCA)
- Distal segment: from SCA to the terminal posterior cerebral arteries (PCA)
- The area of arterial occlusion closely relates to symptoms at presentation.
- The posterior circulation has many collaterals; variability in these collaterals leads to diverse clinical manifestations of basilar artery occlusion.
Mechanism:

- Like other stroke syndromes, the common causes of BAO include embolism, large artery atherosclerosis, small-artery disease, and arterial dissection.7
- A cause of BAO more commonly seen in young patients is traumatic vertebral artery dissection.
- Suspect dissection in a patient with cervical pain and neurologic deterioration.7
Clinical Presentation:
- Prodromal symptoms are a hallmark of BAO.
- More common in the setting of atherosclerotic lesions than emboli, which typically occur with sudden onset of symptoms.
- Symptoms may range from days to months prior to stroke onset.
- As many as two-thirds of patients with BAO experience prodromal symptoms, including TIAs, minor strokes, or other symptoms.2
- The most common prodromal symptoms are headache, neck pain, vision loss, dysarthria, dizziness, and ataxia amongst others.
- “Herald Hemiparesis” is a known finding in BAO that involves a transient hemiparesis that may precede permanent unilateral weakness.8
- Reduced consciousness is another key finding in BAO.
- The reticular activating system (RAS) is in the paramedian tegmental grey matter near the fourth ventricle and is supplied by penetrating branches from the basilar artery.
- The RAS is essential for consciousness, and this area can be compromised in BAO, especially when the middle or distal segments become occluded.
- The pons is the region of the brain most often affected by BAO.8
- Symptoms are predominantly motor and oculomotor given involvement of the paramedian pontine base (descending long motor tract) and the paramedian tegmentum (oculomotor fibers).
- “Locked In Syndrome”: the most devastating form of BAO, which results from mid-basilar occlusion with bilateral pontine ischemia.
- Characterized by full body paralysis with limited vertical eye movements.
- Patient may appear comatose but be fully conscious.
- High mortality rate in acute phase at approximately 75%.
- Proximal and middle segment occlusion often result in large pontine strokes.
- May manifest with either hemi or quadriplegia.
- Additional findings include reduced consciousness, dysarthria, dysphagia, horizontal gaze paresis, and other cranial nerve palsies.2
- Distal segment occlusion can cause strokes in the mesencephalon and thalamus.
- Symptoms include decreased consciousness, quadriparesis, and oculomotor and pupillomotor dysfunctions.2
- “Top of the basilar syndrome” is a presentation most often caused by embolic occlusion of the distal basilar artery.2
- Characterized primarily by visual, oculomotor, and behavioral changes, and can occur without significant motor dysfunction.
- May present with somnolence, vivid hallucinations, or dream-like behavior.
Evaluation:

- Early BAO may present with nonspecific symptoms such as dizziness and vertigo.
- A patient presenting with vertigo plus at least one other neurologic symptom has a higher chance of vertebrobasilar ischemia.9
- Most common signs include oculomotor palsies, dysarthria, dysphagia, truncal/appendicular ataxia, and limb weakness.
- Vertical or alternating horizontal nystagmus in primary gaze is of central etiology until proven otherwise.7
- The head impulse, nystagmus type, and test of skew (HINTS) is a sensitive clinical decision tool that is useful to distinguish between central and peripheral vertigo.
- An additional tool that can be used to risk stratify patients presenting with dizziness who may be experiencing posterior circulation stroke is an ABCD2 score.
- 1% of patients with a score of 3 or less had a diagnosis of stroke, whereas those with a score of 6-7 had stroke in 27% of cases.10

- Standardized scales such as NIHSS may be beneficial to determine severity of symptoms, guide treatment, and are useful when speaking with other physicians regarding the case.
- NIHSS does have limitations when applied to posterior circulation (PC) strokes.
- The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions.12
- NIHSS underestimates clinical severity in PC strokes as it does not investigate many symptoms present in PC stroke including diplopia, dysphagia, gait instability, hearing, nystagmus.12
Imaging:
- The diagnosis of BAO requires dedicated imaging studies that demonstrate occlusion or ischemia in the basilar artery distribution.
- CT non-contrast of the head can be done to rule out hemorrhagic stroke and can sometimes demonstrate “hyperdense artery sign” (HAS).
- HAS has high specificity (95%) for angiographically demonstrated arterial obstruction, but low sensitivity (52%).13
- HAS is more likely to be identified in proximal than distal arteries, likely due to larger caliber of proximal arteries.
- In a case with high pretest probability for BAO, a hyperdense basilar artery (as demonstrated in Figure 1) is a specific predictor for BAO and can help expedite care and interventions if seen early.
- HAS is seen in up to 50% of BAO cases.14
- CT angiography of head and neck with contrast may demonstrate filling defects within the basilar artery.
- If CT imaging does not provide evidence of basilar artery stroke and suspicion remains high, MRI/MRA should be pursued as it is more sensitive for identifying early ischemia and vascular occlusion.
- While MRI is more resource and time intensive, studies have shown that a 6-minute protocol can give sufficient information to dictate treatment in the right setting.15
- DWI MRI sequence can show an acute brainstem or cerebellar infarct within seconds of the arterial occlusion.4
Differential Diagnoses:
- Meningitis, mass in posterior fossa, metastasis, supratentorial lesion with mass effect, herniation basilar migraine, Miller Fisher Syndrome, nonconvulsive status epilepticus, cerebellar hemorrhage, cerebellar infarct, subarachnoid hemorrhage, hypoglycemia, Todd paralysis, conversion disorder, metabolic coma
Diagnosis:
- Diagnosis is made by imaging demonstrating occlusion within the basilar artery.
- Basilar artery occlusion remains a challenging diagnosis to make, and the delays in reaching the diagnosis can have considerable impact on health outcomes.
- Median time from ED arrival to diagnosis was 8 hours 24 min in one study, with only 19% being diagnosed within the 4.5-hour IV thrombolytic window.15
Treatment:
- Several treatment modalities have been described for BAO, including intravenous thrombolysis (IVT) which involves systemic administration of agents such as TNK or tPA, intra-arterial thrombolysis (IAT) via microcatheter at thrombus site, or mechanical endovascular thrombectomy (EVT).
- As BAO is rare, there are limited randomized clinical trials (RCTs) describing outcomes based on modality of treatment.
- A 2023 Systematic review and meta-analysis of 4 major RCTs for BAO treatment described higher odds of modified Rankin score (a 6-point disability score for post-stroke patients) 0-3 at 90 days in patients who underwent EVT vs. medical management (MM) alone.17
- EVT was associated with decreased mortality and better outcomes in BAO up to 24 hours from stroke symptoms compared to MM.
- Mechanical thrombectomy should be considered for any patient who presents <6 hours since time LKW, and in any patient <24 hours with salvageable brain tissue demonstrated on structural neuroimaging studies.18
- All patients with BAO who arrive within the 3-4.5-hour time window since LKW should be given thrombolytic therapy if there are no contraindications.
- Those who are eligible for mechanical thrombectomy should be taken to angiography for EVT.
- Making at least three mechanical thrombectomy passes before stopping the procedure had significant advantage of recanalization in BAO patients.19
- Those who are ineligible for thrombolytics can be put on acute anticoagulation or antiplatelet regimen.
- All patients who receive thrombolytics for ischemic stroke should be admitted to a neurosurgical, neurologic, or medical ICU for management and monitoring, as this is shown to decrease mortality and length of stay.20
Prognosis:
- Despite advances in imaging and treatment options, BAO is associated with high morbidity and mortality.
- In hospital mortality estimated at 30-40%.17
- 65-78% of survivors have significant disability one month after hospital discharge.
- Mortality in absence of reperfusion reach as high as 83-96%.21
Pearls:
- Up to ⅔ of patients with BAO will experience prodromal symptoms such as vertigo, nausea, headache, neck pain, dysarthria, or ataxia.
- Clinicians should consider BAO in a patient with dizziness plus any other neurological deficit, particularly fluctuating level of consciousness, diplopia, or unsteady gait.
- HINTS exam and ABCD2 score can be used as adjuncts in risk stratifying patients presenting with vertigo and dizziness who you assess for posterior circulation stroke.
- Hyperdense artery sign of the basilar artery is highly specific for BAO. MRI/MRA should be pursued when there is high suspicion for posterior circulation stroke.
- Mechanical thrombectomy has become the preferred treatment modality for BAO as it has mortality and functionality benefits over medical management alone.
References:
- Gaillard F, Glick Y, Tatco V, et al. Top of the basilar syndrome. Reference article, Radiopaedia.org (Accessed on 15 Apr 2023) https://doi.org/10.53347/rID-6257
- Mattle HP, Arnold M, Lindsberg PJ, Schonewille WJ, Schroth G: Basilar artery occlusion. Lancet Neurol. 2011, 10:1002-1014. 1016/S1474-4422(11)70229-0
- Rai AT, Seldon AE, Boo S, Link PS, Domico JR, Tarabishy AR, Lucke-Wold N, Carpenter JS. A population-based incidence of acute large vessel occlusions and thrombectomy eligible patients indicates significant potential for growth of endovascular stroke therapy in the USA. J Neurointerv Surg. 2017 Aug;9(8):722-726. doi: 10.1136/neurintsurg-2016-012515. Epub 2016 Jul 15. PMID: 27422968; PMCID: PMC5583675.
- Reinemeyer NE, Tadi P, Lui F. Basilar Artery Thrombosis. [Updated 2022 Dec 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532241/
- Ikram A, Zafar A. Basilar Artery Infarct. [Updated 2022 Oct 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551854/
- Circle of Willis. Wikipedia. https://en.wikipedia.org/wiki/Circle_of_Willis Published January 24, 2007. Accessed April 13, 2023.
- Demel SL, Broderick JP. Basilar Occlusion Syndromes: An Update. Neurohospitalist. 2015 Jul;5(3):142-50. doi: 10.1177/1941874415583847. PMID: 26288672; PMCID: PMC4530423.)
- Caplan L. Posterior circulation cerebrovascular syndromes. Post TW, ed. UpToDate. Waltham, MA: UpToDate, Inc. http://www.uptodate.com. (Accessed on April 5, 2023.)
- Voetsch B, DeWitt LD, Pessin MS, Caplan LR. Basilar Artery Occlusive Disease in the New England Medical Center Posterior Circulation Registry. Arch Neurol. 2004;61(4):496–504. doi:10.1001/archneur.61.4.496
- Navi BB, Kamel H, Shah MP, et al. Application of the ABCD2 score to identify cerebrovascular causes of dizziness in the emergency department. Stroke. 2012;43(6):1484-1489. doi:10.1161/STROKEAHA.111.646414
- ABCD2 Score criteria. ResearchGate. https://www.researchgate.net/figure/ABCD2-score-to-assess-the-risk-of-stroke-after-TIA_tbl2_259529729. Published January 2014. Accessed April 20, 2023.
- Siniscalchi A, Sztajzel R, Malferrari G, Gallelli L. The National Institutes of Health Stroke Scale: Its Role in Patients with Posterior Circulation Stroke. Hosp Top. 2017;95(4):79-81. doi:10.1080/00185868.2017.1322888
- Mair G, Boyd EV, Chappell FM, von Kummer R, Lindley RI, Sandercock P, Wardlaw JM; IST-3 Collaborative Group. Sensitivity and specificity of the hyperdense artery sign for arterial obstruction in acute ischemic stroke. Stroke. 2015 Jan;46(1):102-7. doi: 10.1161/STROKEAHA.114.007036. Epub 2014 Dec 4. PMID: 25477225; PMCID: PMC4338528.
- Goldmakher GV, Camargo EC, Furie KL, Singhal AB, Roccatagliata L, Halpern EF, et al. Hyperdense basilar artery sign on unenhanced CT predicts thrombus and outcome in acute posterior circulation stroke. Stroke. 2009;40(1):134–9. https://doi-org.foyer.swmed.edu/10.1161/STROKEAHA.108.516690.
- Nael K, Khan R, Choudhary G, Meshksar A, Villablanca P, Tay J, et al. Six-minute magnetic resonance imaging protocol for evaluation of acute ischemic stroke: pushing the boundaries. Stroke. 2014;45(7):1985–91. https://doi-org.foyer.swmed.edu/10.1161/STROKEAHA.114.005305.
- Burns JD, Rindler RS, Carr C, et al. Delay in Diagnosis of Basilar Artery Stroke. Neurocrit Care 24, 172–179 (2016). https://doi-org.foyer.swmed.edu/10.1007/s12028-015-0211-0
- Abdalkader M, Finitsis S, Li C, et al. Endovascular versus Medical Management of Acute Basilar Artery Occlusion: A Systematic Review and Meta-Analysis of the Randomized Controlled Trials. J Stroke. 2023;25(1):81-91. doi:10.5853/jos.2022.03755
- Kazmi JS, Chulpayev B, Jung RS et al. An Update on the Treatment of Basilar Artery Occlusion. Curr Treat Options Neurol 25, 55–69 (2023). https://doi-org.foyer.swmed.edu/10.1007/s11940-023-00748-5
- de Havenon A, Elhorany M, Boulouis G, et al. Thrombectomy in basilar artery occlusions: impact of number of passes and futile reperfusion. J Neurointerv Surg. 2023;15(5):422-427. doi:10.1136/neurintsurg-2022-018715
- Jorgensen H, Nakayama H, Raaschou H, Larsen K, Hubbe P, Olsen T. (1995). The Effect of a Stroke Unit. Stroke A Journal of Cerebral Circulation, 26 (7), 1178-1182.
- Schonewille WJ, Wijman CA, Michel P, Rueckert CM, Weimar C, Mattle HP, et al. Treatment and outcomes of acute basilar artery occlusion in the basilar artery international cooperation study (BASICS): a prospective registry study. Lancet Neurol 2009; 8:724-730.




