
Authors: Ernesto Hernandez, MD (EM Resident Physician, Advocate Christ Medical Center, Oak Lawn, IL); Jennifer Woodruff, MD (EM Attending Physician, Advocate Christ Medical Center, Oak Lawn, IL) // Reviewed by: Sophia Görgens, MD (EM Physician, Northwell, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 74-year-old female with a past medical history of hypertension, diabetes, recent basilar artery stent placement with a 20 pack-year smoking history presents to the ED via EMS for altered mental status and episodes of apnea.
Vital signs include BP 168/89, HR 96, T 98.3, RR 3, SpO2 95% on 15L non-rebreather mask. Symptoms started acutely about 15 minutes prior to arrival. On exam, the patient opens eyes to voice, has extraocular movements intact, is unable to speak, and has 0/5 strength in all extremities. The patient was intubated for acute hypercapnic and hypoxic respiratory failure and airway protection.
CT head without contrast1 is performed and reveals the following:
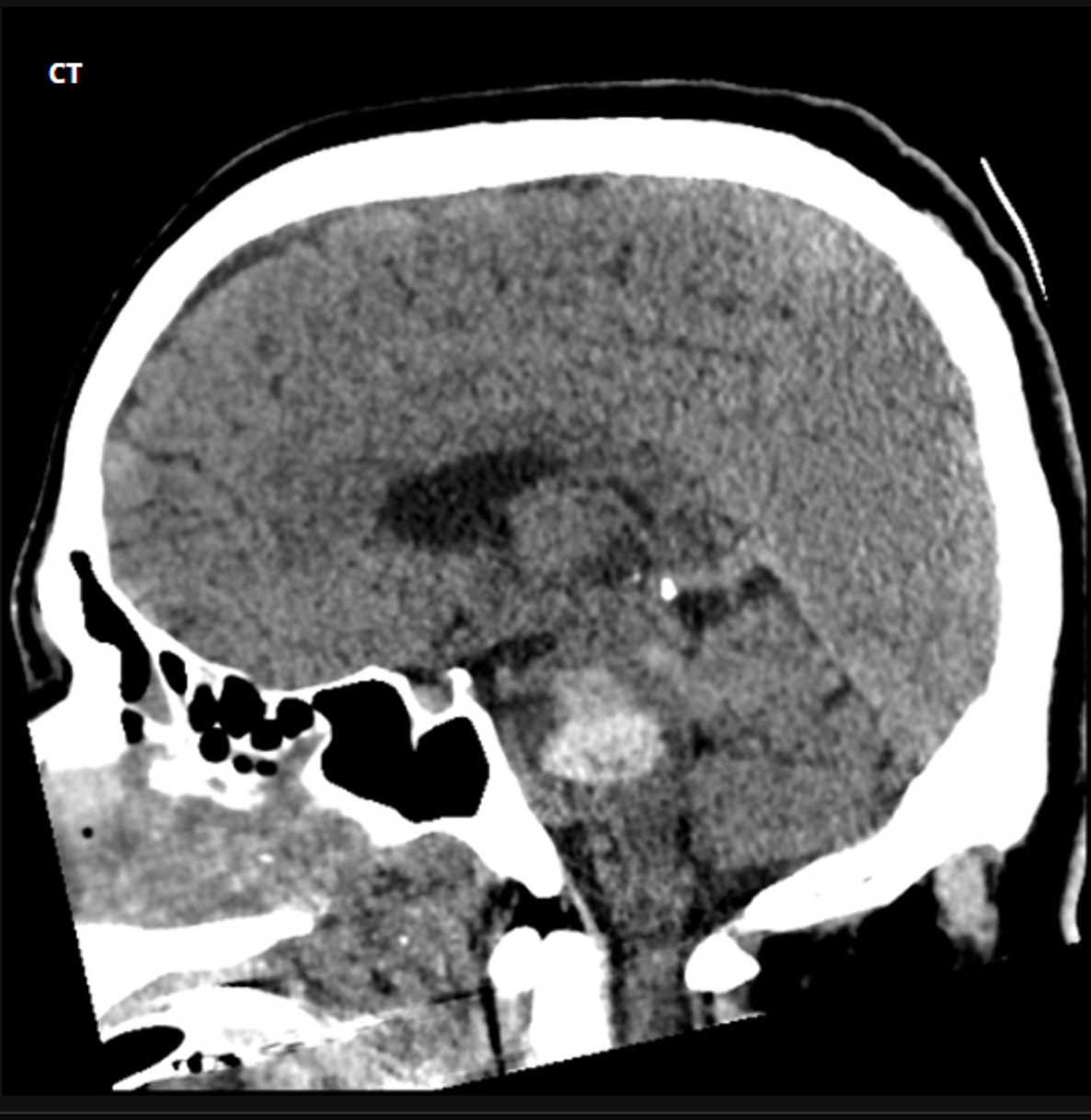
Question: What is the diagnosis?
Answer: Brainstem stroke specifically in the pons resulting in locked in syndrome.
Risk factors:
- 10% of ischemic strokes occur in the brainstem2
- Risk factors for ischemic brainstem stroke3:
- Atherosclerosis
- Hypertension
- Diabetes
- Smoking
- Atrial fibrillation
- Hyperlipidemia
- Ischemic heart disease
- Embolism
- Dissection
- Risk variables for hemorrhagic brainstem strokes 3:
- Hypertension
- Anticoagulant use
- AV malformations
- Amyloid angiopathy
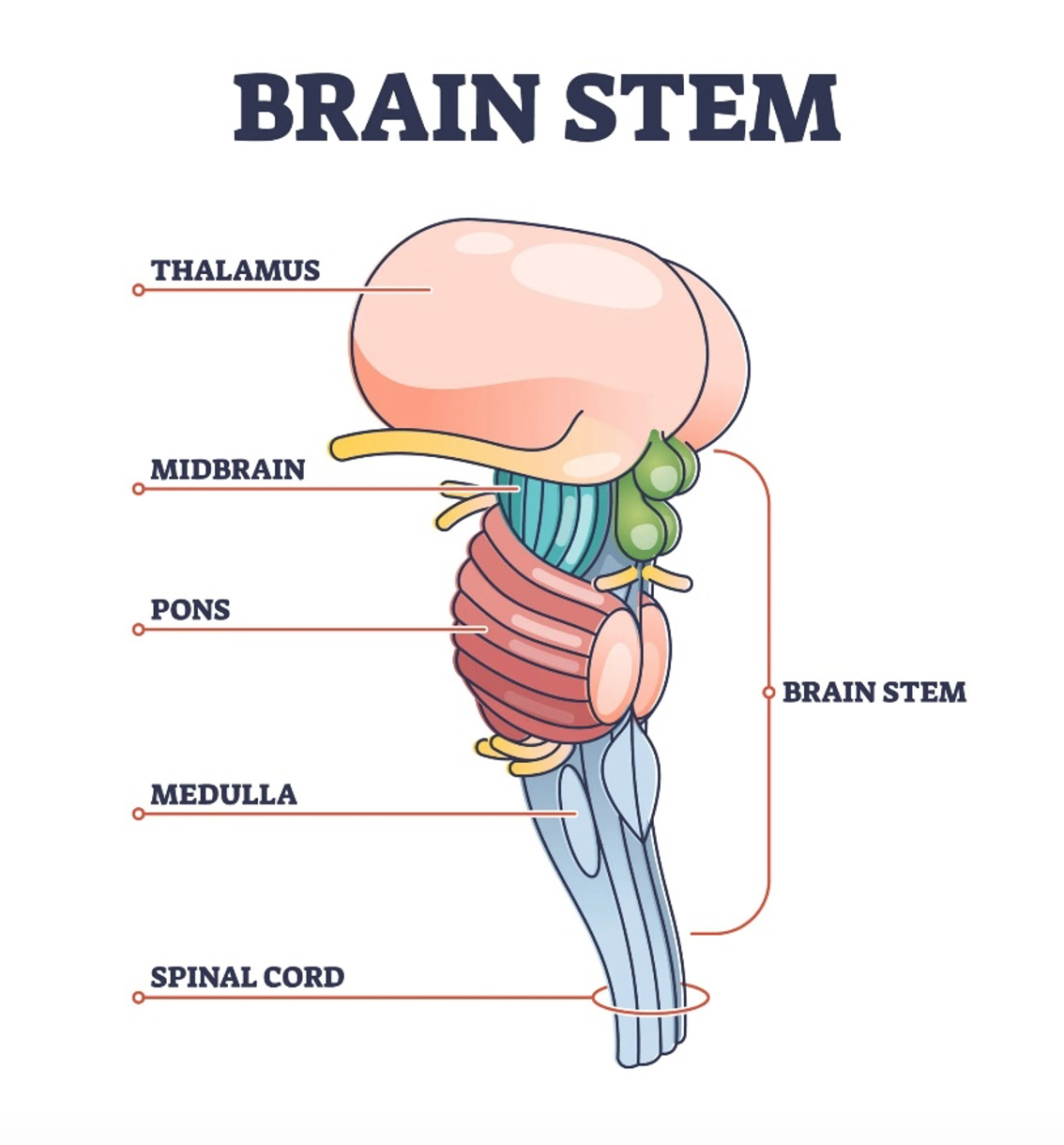
Anatomy:4
Clinical presentation:
- Deficits depend on region affected5
- Localization
- Step 1: Identify midbrain vs pons vs medulla involvement
- “Rule of 4’s”5
- Impaired CN I-IV = lesion above pons
- Impaired CN V-VIII = lesion from the pons
- Impaired IX-XII = lesion from the medulla
- Step 2: Identify medial vs lateral involvement
- 4 medial structures start with M5
- Motor tract (corticospinal tract)
- Deficit: contralateral weakness of limbs
- Medial lemniscus (extension of dorsal columns)
- Deficit: contralateral loss of vibration and proprioception of limbs
- Medial longitudinal fasciculus
- Deficit: ipsilateral internuclear ophthalmoplegia
- Motor nuclei of CN III, IV, VI, XII
- All divisible equally into 12
- Deficit: respective CN motor dysfunction
- Motor tract (corticospinal tract)
- 4 lateral structures start with S – s for side5
- Spinocerebellar tract
- Deficit: ipsilateral ataxia of the limbs
- Spinothalamic tract
- Deficit: contralateral loss of pain and temperature affecting the limbs
- Sensory nucleus of CN V
- Deficit: ipsilateral loss of pain and temperature affecting trigeminal distribution of face
- Sympathetic tract
- Deficit: ipsilateral Horner syndrome (classic triad- ptosis, miosis, anhidrosis)
- Spinocerebellar tract
- 4 medial structures start with M5
- “Rule of 4’s”5
- Step 1: Identify midbrain vs pons vs medulla involvement
Evaluation:
- Point-of-care glucose
- Hypoglycemia can present with stroke-like symptoms
- NIHSS – National Institute of Health Stroke Scale used by Nebraska Mission: Lifeline Stroke6


- Non-contrast CT head, CTA head and neck or MRI7
- CT preferred for speed and availability
- Determines if there is hemorrhagic etiology
- CTA head and neck is useful for identifying large-vessel occlusions (LVOs) which can be targets for mechanical thrombectomy
- CT perfusion scan can also be used to help determine a penumbra
- MRI is more sensitive for ischemic strokes
- CT preferred for speed and availability
- Additional stroke workup: CBC, BMP, lipid panel, PT, PTT, hemoglobin A1C, EKG, hcg (if applicable)
Treatment:
- Stabilization of patient’s ABCs
- Normoglycemia
- Ischemic:
- Thrombolytics if no contraindications
- Contraindications for thrombolytics8
- Thrombolytics if no contraindications

-
-
- ACEP 2015 Clinical Policy with B and C level recommendations for thrombolytics (tPA)9
- Only ECASS-III (1995) and NINDS-II (2008) were RCTs that showed disability benefit, however some showed concern regarding imbalances in stroke severity and were re-analyzed10
- NINDS: very small improvement in NIHSS – limited by small scale. No significant benefits were found
- ECASS-III: No significant benefits were found
- Permissive hypertension
- Like cerebrovascular ischemic strokes, patients should be treated with dual anti-platelet therapy
- If embolism at main vertebral or basilar artery, thrombectomy by a Neurointerventionalist may recommended
- Small study in 2019 and 2020 showed no difference between thrombectomy vs medical treatment alone11,12
- More studies are needed to assess significance of thrombectomy in this patient population
- Small study in 2019 and 2020 showed no difference between thrombectomy vs medical treatment alone11,12
-
- Hemorrhagic:
- Reversal of anticoagulation
- See link13 for more information
- Control blood pressure14
- Can use IV labetalol or nicardipine/clevidipine infusion
- Blood pressure goals:
- If ischemic and receiving thrombolysis
- Prior to thrombolytics: <185/110
- After thrombolytics: <180/105 for first 24 hours
- If ischemic and NOT receiving thrombolysis allow permissive hypertension unless:
- Systolic >220
- Diastolic >120
- Evidence of end organ damage
- If hemorrhagic: systolic goal 140-180
- AVOID hypotension and >10% decreases in blood pressure
- If ischemic and receiving thrombolysis
- Blood pressure goals:
- Can use IV labetalol or nicardipine/clevidipine infusion
- Surgery is controversial and NOT recommended. However, there is current trial underway to assess surgical management15
- Reversal of anticoagulation
Disposition:
- Patients require close monitoring in intensive care with ischemic or hemorrhagic brainstem strokes
- It is important to watch for worsening hemorrhage in closed space or if ischemic, the possibility of hemorrhagic conversion
- Risk factors for hemorrhagic transformation (HT): advanced age, stroke severity (NIHSS), hypertension, hyperglycemia, poor collaterals, early infarction on brain imaging, low platelet count, use of antithrombotic drugs, and reperfusion therapy16
- Alteplase and Tenecteplase have a similar 1% risk of symptomatic intracerebral hemorrhage and 5-6% of HT which includes >30% of infarcted tissue with marked mass effect17,18
- It is important to watch for worsening hemorrhage in closed space or if ischemic, the possibility of hemorrhagic conversion
Pearls:
- Deficit depends on area affected:
- Generally, if ipsilateral cranial nerve deficit with contralateral motor/sensory deficit – consider brainstem stroke syndrome
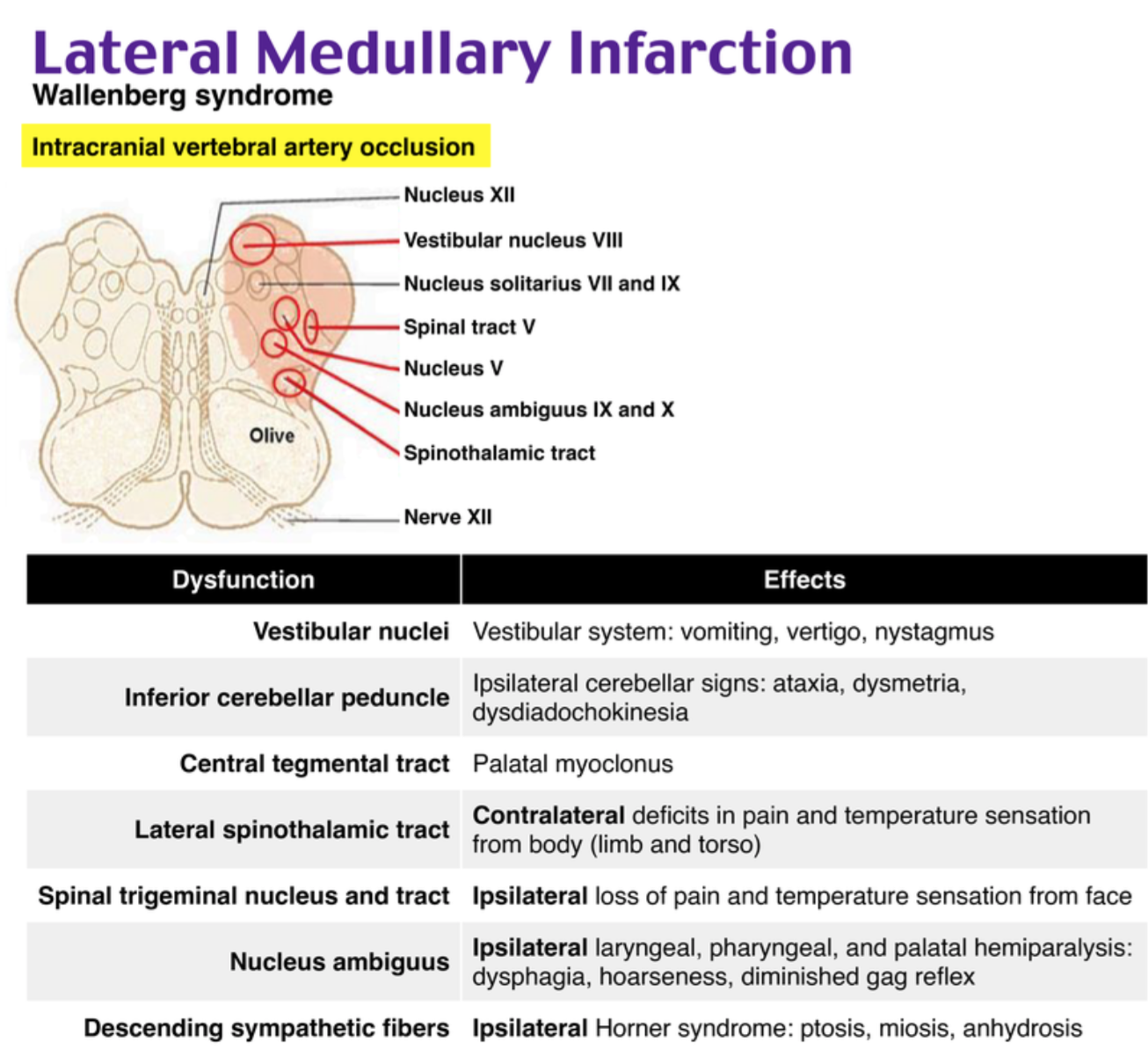
- Most common affected is:
- Lateral medullary syndrome (Wallenburg syndrome) with vertigo, ipsilateral ataxia, ipsilateral sensory loss in face, dysphagia, dysphonia and dysarthria19
- Medical treatment is similar to cerebral cortex ischemic strokes – thrombolytics, dual anti-platelet therapy
- No significant outcome improvement in thrombectomy vs medical management alone
- If hemorrhagic – reversal of anticoagulation, surgical management NOT usually recommended
- Control blood pressure if receiving therapeutics, otherwise will tolerate permissive hypertension

A 45-year-old man presents to the ED with vertigo. Symptoms began approximately 4 hours prior to arrival. He has a history of hypertension and hyperlipidemia and smokes one pack of cigarettes daily. His vital signs are T 98.6°F (37ºC), BP 180/90 mm Hg, HR 78 bpm, RR 14/minute, and SpO2 100% on room air. He has right-sided ptosis, miosis, decreased facial sensation, and loss of the corneal reflex. Upon further inspection, the right side of his palate does not elevate with phonation, and he has loss of pain and temperature sensation on the left arm and leg. Which one of the following is the most likely diagnosis?
A) Basilar artery stroke
B) Cavernous sinus syndrome
C) Lateral medullary infarction
D) Multiple sclerosis
Answer: C
Vertigo, or the internal sensation of motion when no motion exists, is often classified as either peripheral or central depending on the origin of the pathology. Central causes of vertigo include ischemic stroke, demyelinating conditions, cerebellar hemorrhage, vertebrobasilar insufficiency, vertebral artery dissection, multiple sclerosis, malignancy, and vestibular migraine. Causes of peripheral vertigo include paroxysmal peripheral vertigo, Ménière syndrome, vestibular neuronitis, endolymphatic fistula, vestibular ganglionitis, labyrinthitis, ototoxicity from medications (e.g., antibiotics, antimalarials, anticonvulsants, antineoplastics), cerebellopontine angle tumors, and trauma. The vascular territory of the lateral medulla oblongata is supplied by the posterior inferior cerebellar artery. Lateral medullary infarction (Wallenberg syndrome) may present with a constellation of symptoms, including vertigo. Some refer to an ischemic event in this territory with clinical findings as posterior inferior cerebellar artery syndrome. The classic features of this syndrome include ipsilateral cranial nerve deficits (e.g., Horner syndrome, soft palate paralysis) and contralateral deficits in the trunk and extremities (e.g., loss of pain and temperature sensation). This crossed pattern of deficits is a hallmark of the diagnosis. Dysphagia or dysphonia may be present, along with deficits of the sixth, seventh, and eighth cranial nerves. Emergent MRI and neurology consultation are required for diagnosis and management.
Basilar artery stroke (A) involves the middle posterior circulation and may present with unilateral limb weakness, headache, dizziness, dysphagia, dysarthria, cranial nerve VIl deficits, or diplopia.
Cavernous sinus syndrome (B) usually presents with cranial nerve deficits, diplopia, periorbital cellulitis, and facial swelling that may progress to meningitis or sepsis.
Multiple sclerosis (D) is a chronic, progressive demyelination disorder that classically presents with neurologic deficits separated by time and space (i.e., anatomic region). Symptoms are often relapsing and remitting, and typically include visual manifestations (e.g., optic neuritis).






{kind=link}
{kind=link}