
Author: Rachel Bridwell, MD (@rebridwell, EM Resident Physician, SAUSHEC / San Antonio, TX) // Reviewed by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 22-year old male presents to the ED after landing on his right thumb while playing football with some friends. The pain and swelling became progressively worse as he notes pain with any movement of his thumb. He is right hand dominant, a non-smoker, and works as an analyst at a large bank.
Triage vital signs (VS): BP 127/82, HR 91, T 98.2, RR 16, SpO2 99% on room air. On exam, the right MCP joint is edematous with point tenderness and ecchymosis, though the skin is closed. He has normal radial and median sensation and strength, with 2+ radial and ulnar pulses.
X-ray reveals the following:

What is your next step in evaluation and treatment?
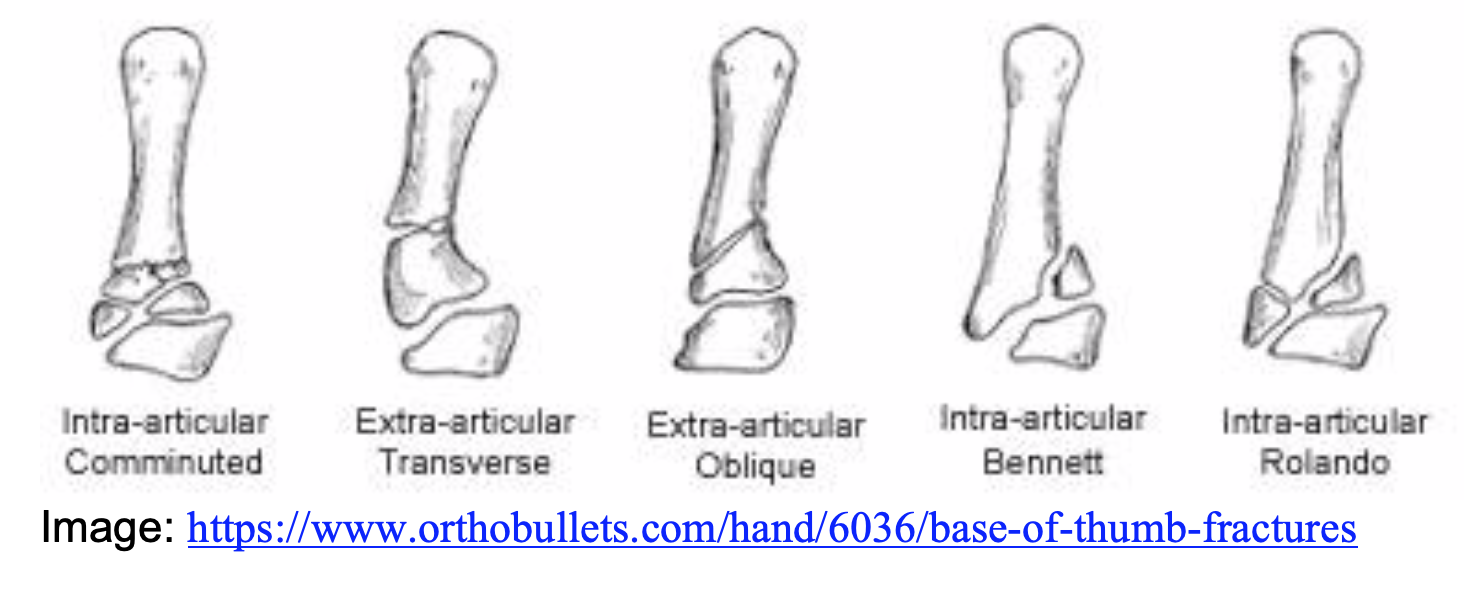
Answer: 1st Metacarpal Base Fracture1-15
Epidemiology:
- Bimodal distribution of thumb fractures in pediatric and elderly population
- Pediatric: 22% of tubular bone fractures occur in thumb1
- Elderly (>65): Of all hand fractures, 20% occur in the thumb1
- 17-40 years old: only 12% involve thumb1
- Relatively infrequent, making up 1.4-4% of hand fractures2,3
- Rolando fractures account for 15-20% of all 1st metacarpal (MCP) base fractures4
- Rolando and Bennett are caused by axial force to a thumb in flexion
- Falls, assault
- Greater disability when occurs in dominant hand5
Anatomy:
- Bennett: Partial intra-articular fracture of base of 1st metacarpal
- Occurs on ulnar side5
- At the side of locus minoris resistenziae (place of less resistance) which in the 1st MCP is the anteromedial margin6
- Not multifragmented5
- Occurs on ulnar side5
- Rolando: Complete intra articular fracture of base of 1st metacarpal
- Multi-fragmented
- Fracture lines in classic T- or Y-shaped pattern1
- Extra-articular fracture
- Most common pattern
Clinical Presentation:
- Acute pain at the base of the thumb
- Swelling, tenderness, ecchymosis at the base of the MCP
- Physical examination does not differentiate Rolando versus Bennett
- Range of motion limited by pain but unusual for deficits to be present
- Bennett: Trapezium holds intra-articular piece in place. With fracture, the 1st MCP subluxes because of retained Abductor Pollicis Longus et Brevis, Extensor Pollicis Longus et Brevis, moving the MCP dorsally, proximally, and radially7
- Rolando: Abductor Pollicis Longus moves dorsal fragment, metacarpals displaced by Adductor and Extensor Pollicis Longus8
Evaluation:
- Radiographs
- 3 view is standard
- Additional views:
- Robert’s view: true AP of 1st MCPJ1
- Bett’s view: true lateral of thumb1
- 30 degree pronated view
- Bennett’s
- Gedda Classification9
- Fracture with single ulnar fragment and subluxation of metacarpal base
- Impaction fracture without 1st MCP subluxation
- Ulnar avulsion with metacarpal dislocation
- Gedda Classification9


- CT: complex fracture patterns for assessment of detail and location of fragments, helpful for operative planning11
Treatment:
- Non-operative: thumb spica after closed reduction10
- Extra-articular fractures with < 30 degrees of angulation after closed reduction10
- Bennett fractures with < 1mm displacement10
- Bennett: Axial traction with palmar abduction with external pressure over the base of the 1st metacarpal1
- Avoid thumb extension as it displaces fractures and worsens outcomes12
- Rolando: Call Orthopedics for operative management as these are complex fractures and are intrinsically unstable13
- Open reduction and internal fixation versus external fixation with or without pinning14
Disposition:
- Follow up with orthopedics as the fracture reduction is crucial
- Definitive management is operative vs casting
- Fracture alignment crucial– Bennett
- Good anatomic alignment (<1mm step off), no residual symptoms15
- >1mm step off, 54% of patients had residual symptoms with increase osteoarthritis15
Pearls:
- Bennett and Rolando fractures are both considered unstable fractures
- Rolando fractures require operative fixation
- Avoid thumb extension as it worsens fracture displacement
- Refer to hand surgeon to mitigate complications

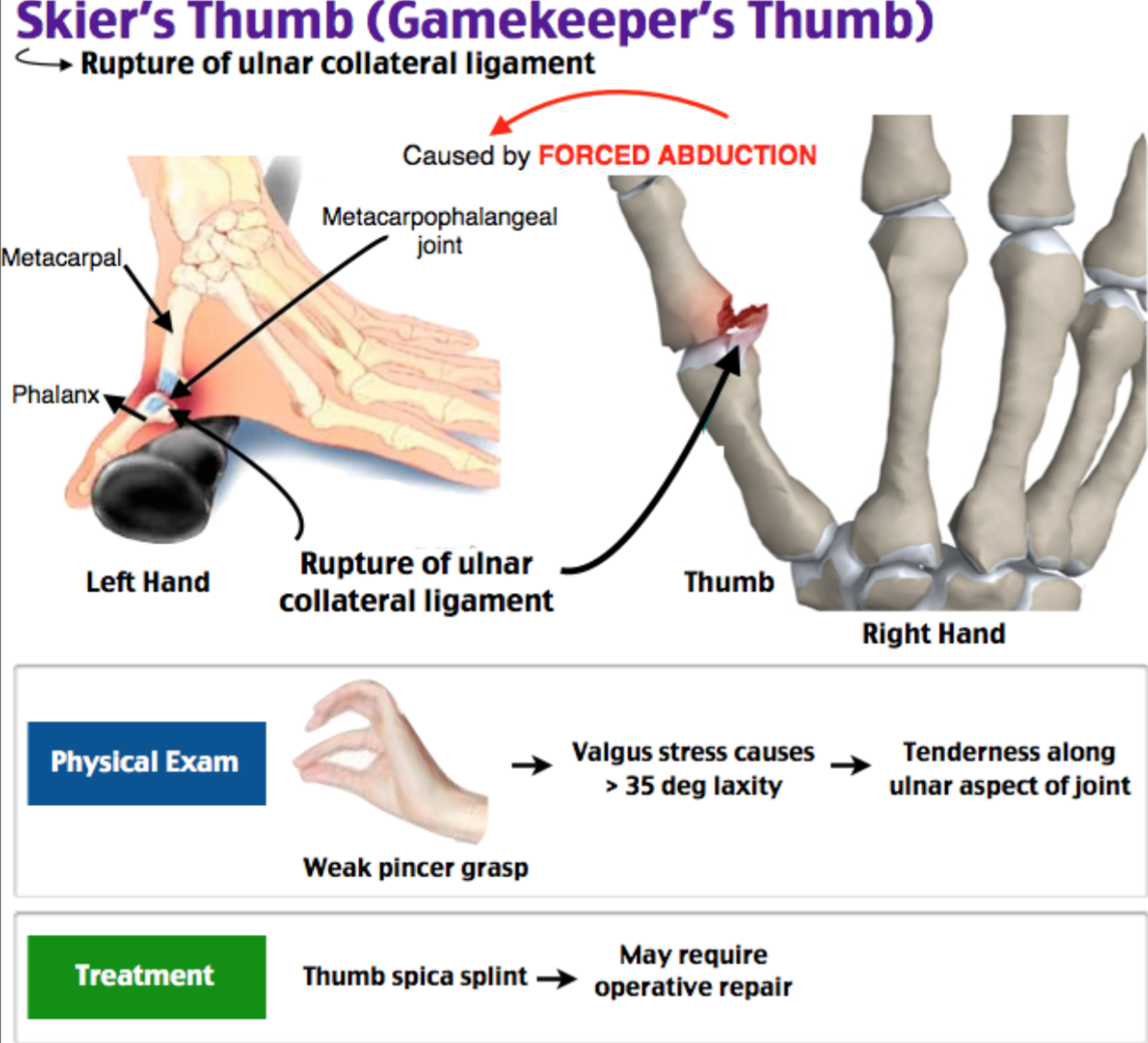
A 24-year-old woman presents with right thumb pain. She recently fell while skiing. On examination, she has swelling and tenderness over the base of the thumb on the ulnar side. She has weakness when pinching an object between her thumb and index finger. Which of the following structures is most likely to be injured?
A) Extensor pollicis brevis
B) Extensor pollicis longus
C) Radial collateral ligament
D) Ulnar collateral ligament
Answer: D
The patient has an injury to the ulnar collateral ligament, also known as “gamekeeper’s thumb” named after Scottish gamekeepers who developed this injury pattern from repeatedly twisting the necks of hares. It is also known as “skier’s thumb” since skiing is now the most common cause of this injury. The injury occurs when the thumb gets stuck in the pole straps during a fall. The mechanism of injury is a forceful radial abduction of the thumb with a subsequent partial or complete tear in the ulnar collateral ligament at the insertion into the proximal phalanx of the thumb. Patients present with pain, swelling, and tenderness on the ulnar side of the metacarpophalangeal joint of the thumb and a weak pincer grasp. Greater than 35 degrees of laxity of thumb abduction or additional 15 degrees of laxity beyond the uninjured side suggests a complete rupture. Radiographs may show a small associated avulsion fracture. Patients should be immobilized in a thumb spica splint and referred to orthopedics. A partial ulnar collateral ligament rupture will often heal well with immobilization alone, but a complete rupture often requires surgical repair.
Extensor pollicis brevis (A) and extensor pollicis longus (B) are incorrect. Injury to these structures would cause weakness of thumb extension, not pincer grasp. Radial collateral ligament (C) injuries are less common than ulnar collateral ligament injuries.
Further Reading:
FOAM Reading:
References:
- Carlsen BT, Moran SL. Thumb Trauma: Bennett Fractures, Rolando Fractures, and Ulnar Collateral Ligament Injuries. J Hand Surg Am. 2009;34(5):945-952. doi:10.1016/j.jhsa.2009.03.017
- Van Onselen EBH, Karim RB, Hage J, Ritt MJPF. Prevalence and distribution of hand fractures. J Hand Surg Am. 2003;28 B(5):491-495. doi:10.1016/S0266-7681(03)00103-7
- Stanton JS, Dias JJ, Burke FD. Fractures of the Tubular Bones of the Hand. J Hand Surg Eur Vol. 2007;32(6):626-636. doi:10.1016/j.jhse.2007.06.017
- Mumtaz M, Ahmad F, Kawoosa A, Hussain I, Wani I. Treatment of Rolando Fractures by Open Reduction and Internal Fixation using Mini T-Plate and Screws. J Hand Microsurg. 2016;08(02):080-085. doi:10.1055/s-0036-1583300
- Windsor TA, Blosser KM, Richardson AC. Rolando fracture. Clin Case Reports. 2019;7(12):2603-2604. doi:10.1002/ccr3.2544
- Liverneaux PA, Ichihara S, Hendriks S, Facca S, Bodin F. Fractures and dislocation of the base of the thumb metacarpal. J Hand Surg Eur Vol. 2015;40(1):42-50. doi:10.1177/1753193414554357
- Rivlin M, Fei W, Mudgal CS. Bennett Fracture. Vol 40. W.B. Saunders; 2015. doi:10.1016/j.jhsa.2015.05.017
- Feletti F, Varacallo M. Rolando Fractures. StatPearls Publishing; 2020. http://www.ncbi.nlm.nih.gov/pubmed/31194364. Accessed July 23, 2020.
- Gedda KO. Studies on Bennett’s fracture; anatomy, roentgenology, and therapy. Acta Chir Scand Suppl. 1954;193:1-114. doi:10.3109/00016925209177031
- Base of Thumb Fractures – Hand – Orthobullets. https://www.orthobullets.com/hand/6036/base-of-thumb-fractures. Accessed July 23, 2020.
- Peterson JJ, Bancroft LW. Injuries of the Fingers and Thumb in the Athlete. Clin Sports Med. 2006;25(3):527-542. doi:10.1016/j.csm.2006.02.001
- Edmunds JO. Traumatic Dislocations and Instability of the Trapeziometacarpal Joint of the Thumb. Hand Clin. 2006;22(3):365-392. doi:10.1016/j.hcl.2006.05.001
- Marsland D, Sanghrajka AP, Goldie B. Static monolateral external fixation for the Rolando fracture: A simple solution for a complex fracture. Ann R Coll Surg Engl. 2012;94(2):112-115. doi:10.1308/003588412X13171221501140
- Mahoney M, Marsland D, Garagnani L, Sauvé P. Rolando and his fracture. Trauma. 2015;17(1):24-28. doi:10.1177/1460408614532046
- Kjær-Petersen K, Langhoff O, Andersen K. Bennett’s fracture. J Hand Surg Am. 1990;15(1):58-61. doi:10.1016/0266-7681(90)90049-A




