
Authors: Mounir Contreras Cejin, MD (EM Resident Physician, UT Southwestern – Dallas, TX); Felipe Gonzalez Gutierrez (Medical Student, UT Southwestern – Dallas, TX); Emmanuel Ohuabunwa, MD, MBA (Attending Physician, UT Southwestern – Dallas, TX) // Reviewed by: Sophia Görgens, MD (EM Physician, Northwell, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 58-year-old female with a history of diabetes, hypertension, and chronic back pain presents to the ED with severe headache and nausea. Her symptoms started shortly after leaving the office of her pain management doctor, where she had an epidural steroid injection to alleviate her chronic back pain approximately 30 minutes before she arrived in the ED. The patient denies any trauma to the head, fevers, nuchal rigidity, changes in vision, focal weakness, paresthesia, or anticoagulation use.
On arrival, she is awake and alert and in obvious distress. Her vitals signs include temperature of 98.8F, HR of 64, BP 133/78, and O2 saturation of 98% on room air with a respiratory rate of 18. Her exam, including a complete neurological exam, is grossly benign. Given her acute complaint and recent history, labs and CT of the head are obtained. The clinician orders analgesics. The patient remains hemodynamically stable and labs are unremarkable, but the CT scan showed the following:
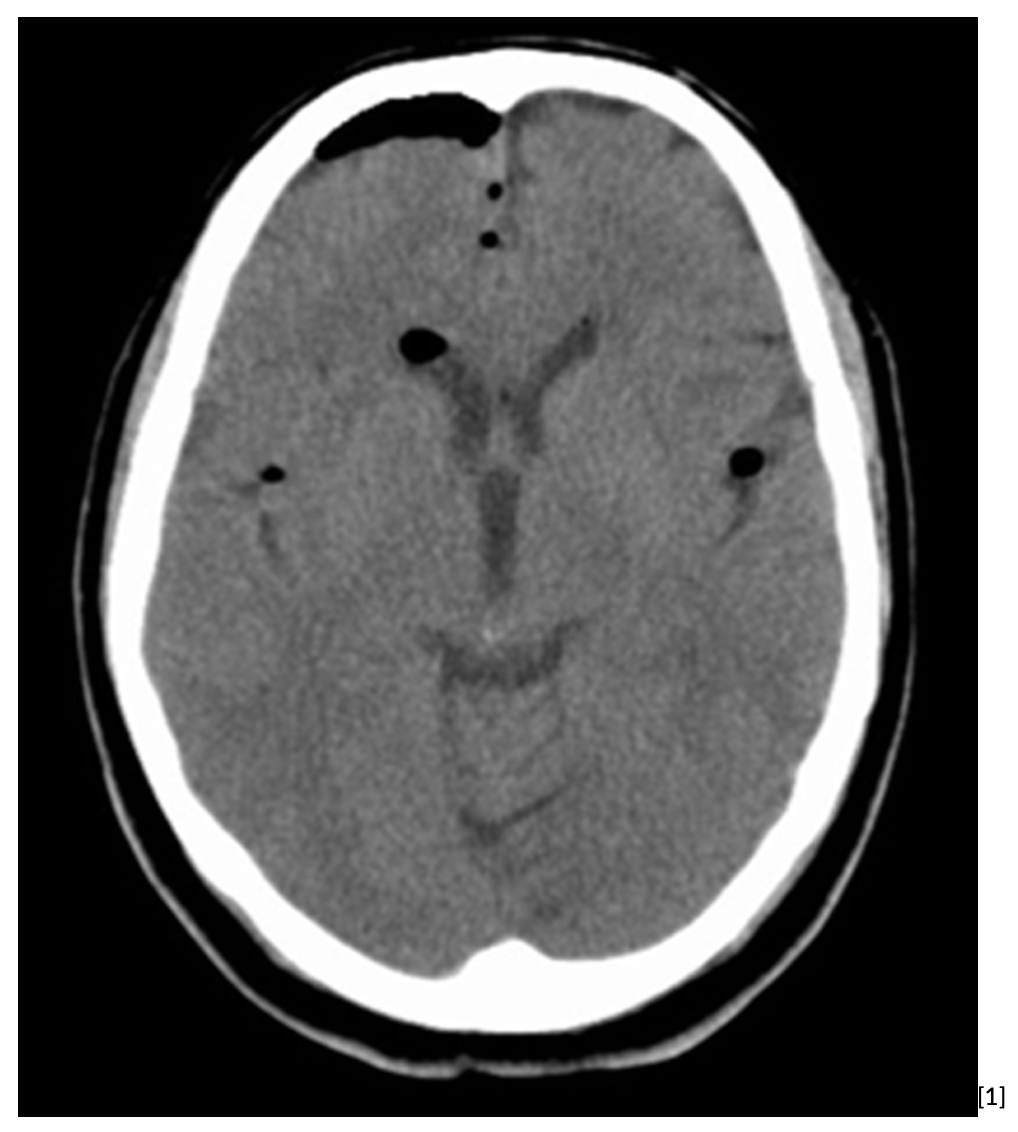
What is the diagnosis?
Answer: Pneumocephalus1-21
Background:
- Pneumocephalus is defined by the presence of air within the cranial cavity.
- The condition is classified as simple or tension pneumocephalus and can also be acute (less than 72 hours) or delayed (greater than 72 hours).
- The most common causes include trauma and cranial surgeries, but there are other etiological factors, and in rare cases, it can also be spontaneous. [1-3]
- The most common location is the frontal region, followed by the occipital and temporal regions. [4]
Epidemiology:
- Pneumocephalus is seen in almost all post-craniotomy cases, whereas the incidence of pneumocephalus seen in trauma involving head injury varies between 3.9% to 9.7% [6]
Pathophysiology:
- Pneumocephalus most commonly occurs when a traumatic event disrupts the integrity of the skull, allowing air to enter the cranial cavity [6]
- Ball valve theory of Dandy: unidirectional movement of air from the outside environment to the cranial cavity (e.g., following positive pressure ventilation) [6]
- This mechanism explains how the dura plugs the fistula tract allowing input but not output
- Inverted-soda-bottle effect of Horowitz and Lunsford: Excessive drainage of cerebral spinal fluid leads to low intracranial pressure and air trapping inside the cranium (e.g., lumbar drain) [7]
- Similar to drinking or pouring from a bottle, as CSF escapes from the cranium air must enter to allow more CSF to exit
- Rarely, production of gas is due to infection by gas-forming organisms [8, 9]
History: Difficult diagnosis, but the following are clues that suggest the presence of pneumocephalus
- Head trauma with or without CSF leak from the nose or ear
- Post-operative meningitis (with gas-forming organisms) [8, 9]
- Headaches or seizures following cranial or spinal surgery [10, 11]
- Oculomotor nerve palsy and tinnitus
Signs and Symptoms: [7]
- Headaches
- Nausea
- Vomiting
- Irritability
- Dizziness
- Seizures
- Syncope
Physical Exam:
- Bruit hydro-aerique (cranial succussion splash) is present in only 7% of patients and is pathognomonic for pneumocephalus [12, 13]
- Patients describe a “splashing” sound when moving their head
- It is heard by auscultating the head during head movement
- Irregularities in breathing patterns or cardiac arrest (i.e., brainstem signs) as seen with tension pneumocephalus [5]
- Changes in sensorium, papilledema, para- and hemiplegia have all been reported with tension pneumocephalus [5]
- Cushing reflex, colloquially called “Cushing’s triad”, is a physiological nervous system response to acute elevation of intracranial pressure (ICP), resulting in a triad that is characterized by widen pulse pressure, bradycardia and irregular respirations [14]
Imaging studies:
Head CT [7]
- Gold standard
- Able to detect as low as 0.55 ml of intracranial air, while a skull radiograph requires at least 2 ml for detection [15]
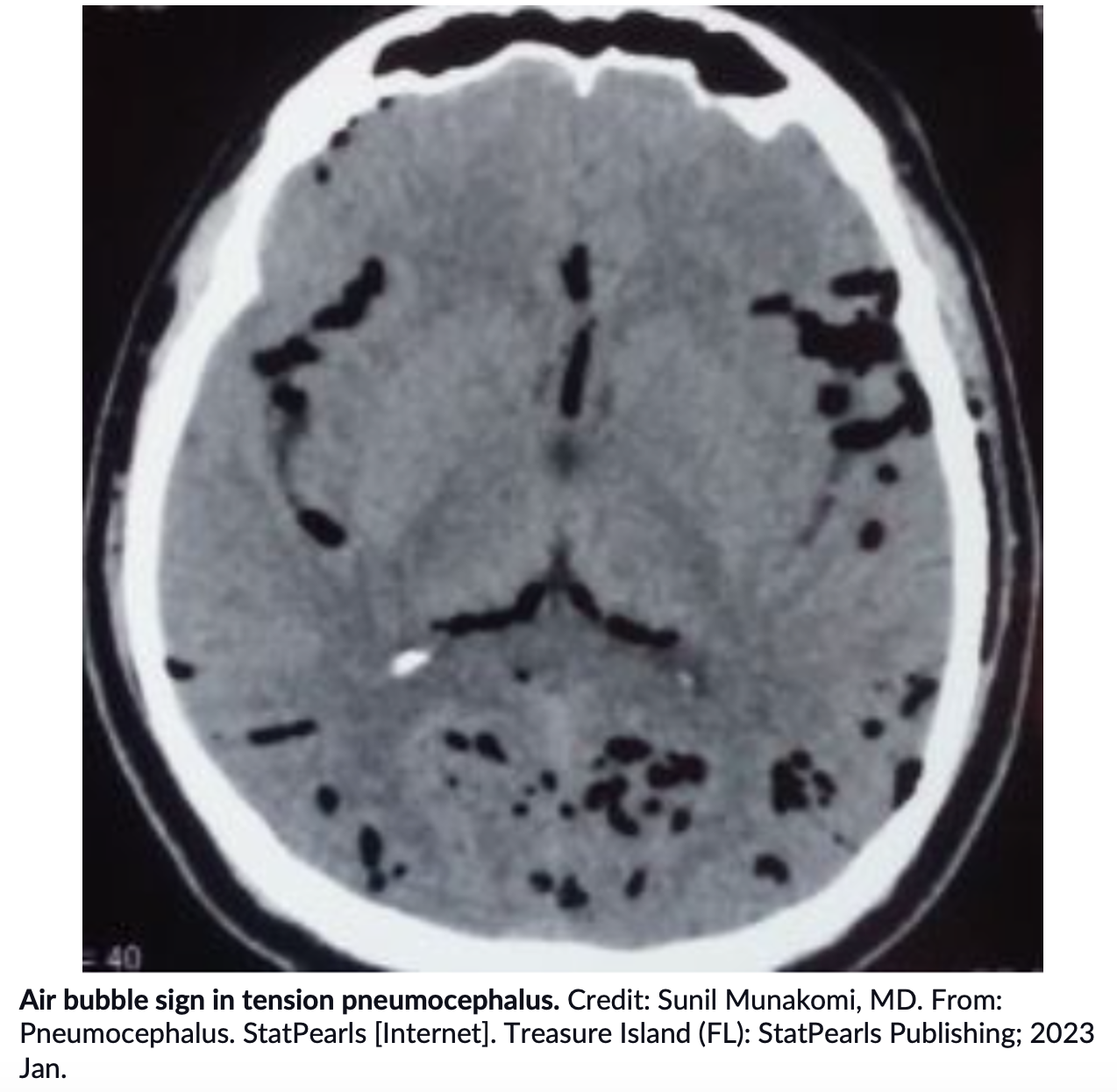
- Two signs on a CT scan are considered characteristic of tension pneumocephalus [16]
- Mount Fuji Sign – a collection of air in the frontal region with partitioning of the frontal lobes
- Air bubble sign – air bubbles scattered in several cisterns
- Consideration: Intracranial fat can appear hypodense on a CT scan and be mistaken for pneumocephalus [17]

MRI [17]
- Useful but not as sensitive as a CT scan
- Consideration: Flow voids or blood products appear dark in all sequences and may be mistaken for air
Management:
Treatment is usually conservative, with 85% of reported cases showing spontaneous reabsorption after 2-3 weeks with the following measures [7, 15]
- Bed-rest, placing the patient in a sitting position at 30 degrees.
- Pain control and antipyretics
- Strict avoidance of Valsalva maneuvers (i.e., coughing, sneezing, nose-blowing)
- High-flow oxygen therapy (i.e., 5 L per minute for five days via non-rebreather mask)
- Oxygen therapy increases the rate of nitrogen absorption
- Strict avoidance of positive pressure
- Osmotic diuresis, if indicated (i.e., traumatic brain injury)
- Mannitol – IV boluses of 0.25 to 1 g/kg every 4 to 5 hours[18]
- This should be done in consultation with neurosurgery as there is a theoretical risk of mannitol leakage into brain tissue when the blood brain barrier is compromised, consequently reversing the osmolar gradient and worsening the edema
- Hyperbaric oxygen therapy [19]
- Although there is a case report describing a posttraumatic pneumocephalus aggravated by hyperbaric chamber treatment [20]
Neurosurgical consultation [17]
- Consult neurosurgery in all cases
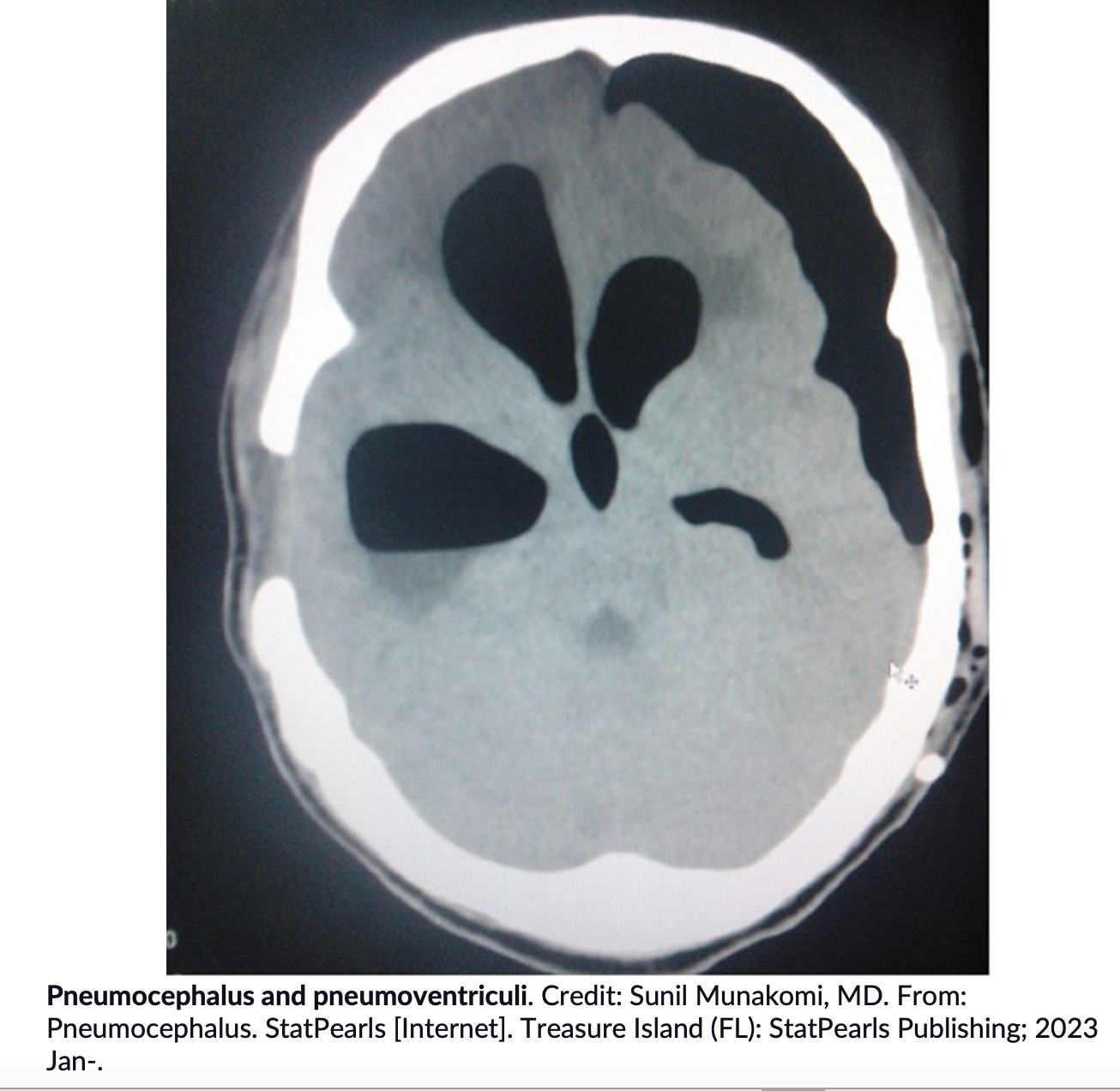
- Indications for possible intervention include: symptomatic or recurrent pneumocephalus, tension pneumocephalus or pneumoventricle, persistent traumatic pneumocephalus (longer than one week)
- Decompression options
- Emergency decompression via burr hole
- Needle aspiration through a burr hole or craniotomy
- Ventriculostomy (for pneumoventricle)
- Decompressive craniectomy
- Insertion of a subdural evacuating port system (SEPS)
- Medical guidelines recommend a wait time of at least seven days following transcranial or spinal surgery prior to air travel [21]
- As height increases, atmospheric pressures decrease, and gases expand. As a result, a previously stable pneumocephalus could turn into intracranial hypertension
- Air travel is not advised for patients with an intracranial air volume greater than 30 ml
Complication and prognosis: [7, 17]
- Complications include: meningitis, brain abscess, seizures, brain herniation
- The condition usually carries a good prognosis as it resolves by itself with conservative measures and even when there is tension pneumocephalus when treatment is given in a timely manner
- In patients with traumatic pneumocephalus, prophylactic ceftriaxone has not shown adequate evidence to prevent meningitis [21]
Pearls:
- Pneumocephalus is a rare occurrence in the non-traumatic patient
- Most cases of pneumocephalus resolve spontaneously with conservative measures
- Avoid positive pressure ventilation in patients with pneumocephalus
- Recognize the emergent nature of tension pneumocephalus to get the right consultants on board
- In traumatic pneumocephalus, prophylactic ceftriaxone has not been shown to be beneficial in preventing meningitis

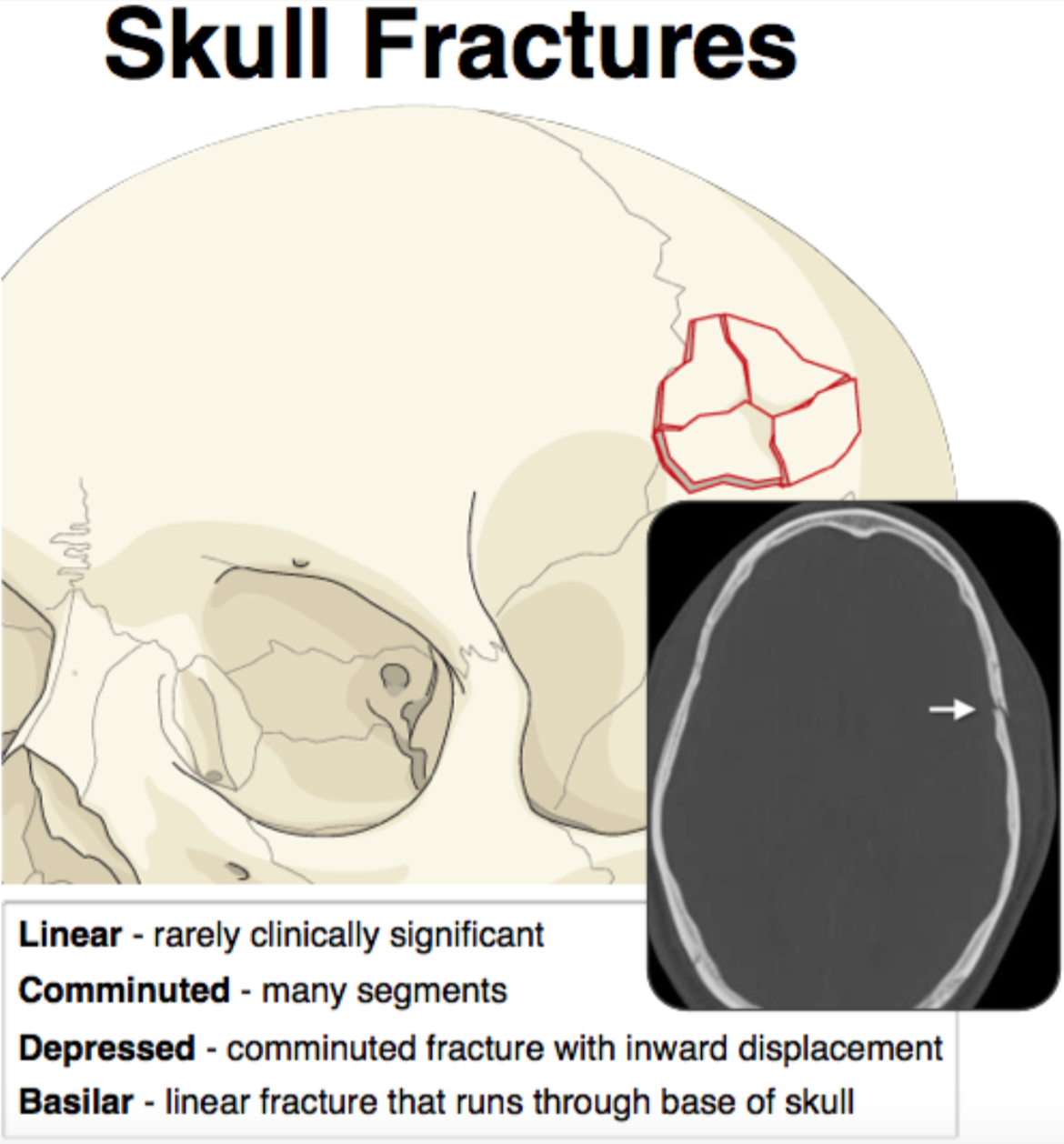
A 34-year-old man is struck in the head with a brick. He is awake and alert with a normal mental status. A 3 cm scalp laceration is noted, and a CT scan of the head shows a linear nondepressed skull fracture in the area of the laceration without evidence of intracranial hemorrhage. In addition to laceration repair, what is the appropriate treatment for this patient?
A) Administration of mannitol
B) Admission for observation
C) Discharge home
D) Discharge home with oral steroids
Answer: B
The patient has a skull fracture with an overlying laceration. This is considered an open fracture. Patients with open skull fractures should be evaluated by neurosurgery and admitted for observation. Skull fractures can be a marker for serious underlying pathology such as intracranial bleeding, so all patients with suspected skull fractures should undergo CT scanning to rule out intracranial injury. The presence of pneumocephalus on the CT scan is a clue that suggests an open skull fracture. A basilar skull fracture is a variant of skull fracture occurring at the base of the skull that can be missed on a CT scan. Physical findings suggestive of a basilar skull fracture include hemotympanum, ecchymosis in the mastoid area (Battle sign), and periorbital ecchymoses (raccoon eyes). The decision to start prophylactic antibiotics in open nondepressed skull fractures is somewhat controversial, and initiation of antibiotics should be discussed with the neurosurgeon who will be caring for the patient. Patients with open, depressed skull fractures should receive prophylactic antibiotics.
Administration of mannitol (A) is indicated for patients with elevated intracranial pressure. By promoting an osmotic diuresis, mannitol reduces intracranial pressure in patients with an expanding brain hematoma or edema and impending herniation. This patient has a normal mental status and no signs of intracranial hemorrhage, so it is very unlikely he has elevated intracranial pressure.
Discharging home (C) is incorrect because admission for observation is required for patients with open skull fractures.
There is no evidence that steroids (D) are beneficial in head injury.
Further Reading
References:
- İnce I, Ahiskalioglu A, Aksoy M, Dostbil A, Celik M. Pneumocephalus after lumbar epidural catheter: a case report. Anaesth Pain & Intensive Care 2014;18(2):186-188
- Pillai P, Sharma R, MacKenzie L, Reilly EF, Beery PR, Papadimos TJ, Stawicki SP. Traumatic tension pneumocephalus – Two cases and comprehensive review of literature. Int J Crit Illn Inj Sci. 2017 Jan-Mar;7(1):58-64.
- Álvarez-Holzapfel MJ, Aibar Durán JÁ, Brió Sanagustin S, de Quintana-Schmidt C. [Diffuse pneumocephalus after lumbar stab wound]. An Pediatr (Engl Ed). 2019 Jan;90(1):63-64.
- Solomiichuk VO, Lebed VO, Drizhdov KI. Posttraumatic delayed subdural tension pneumocephalus. Surg Neurol Int. 2013;4:37.
- Kankane VK, Jaiswal G, Gupta TK. Posttraumatic delayed tension pneumocephalus: Rare case with review of literature. Asian J Neurosurg. 2016 Oct-Dec;11(4):343-347.
- Moon HS, Lee SK, Chung SH, Chung JH, Chang IB. Recurred pneumocephalus in a head trauma patient following positive pressure mask ventilation during induction of anesthesia -A case report-. Korean J Anesthesiol. 2010 Dec;59 Suppl(Suppl):S183-6.
- Dabdoub CB, Salas G, Silveira Edo N, Dabdoub CF. Review of the management of pneumocephalus. Surg Neurol Int. 2015 Sep 29;6:155. doi: 10.4103/2152-7806.166195. PMID: 26500801; PMCID: PMC4596054.
- Penrose-Stevens A, Ibrahim A, Redfern RM. Localized pneumocephalus caused by Clostridium perfringens Br J Neurosurg. 1999;13:85–6.
- Lee EJ, Kim RO, Lee M, Joo BE. Concurrent Spontaneous Pneumocephalus and Subarachnoid Hemorrhage Due to Klebsiella Pneumoniae J Clin Neurol. 2022 Mar;18(2):253-255.
- Palacios-García JM, Vazquez-Becerra E, Ropero-Romero F. Seizure as Early Presentation of a Pneumocephalus after Cochlear Implant: A Case Report. J Int Adv Otol. 2020 Dec;16(3):470-472.
- Kim TK, Yoon JR, Kim YS, Choi Y, Han S, Jung J, Park IS. Pneumocephalus and headache following craniotomy during the immediate postoperative period. BMC Surg. 2022 Jun 29;22(1):252.
- Bernstein AL, Cassidy J, Duchynski R, Eisenberg SS. Atypical headache after prolonged treatment with nasal continuous positive airway pressure. 2005;45:609–11.
- Zasler ND, Katz DI, Zafonte RD. Brain Injury Medicine, Principles And Practice. Demos Medical Publishing. (2007 ) ISBN:1888799935.
- Dinallo S, Waseem M. Cushing Reflex. In: StatPearls. Treasure Island (FL): StatPearls Publishing; March 20, 2023.
- Karavelioglu E, Eser O, Haktanir A. Pneumocephalus and pneumorrhachis after spinal surgery: case report and review of the literature. Neurol Med Chir (Tokyo). 2014;54(5):405-7.
- Ishiwata Y, Fujitsu K, Sekino T, Fujino H, Kubokura T, Tsubone K, Kuwabara T. Subdural tension pneumocephalus following surgery for chronic subdural hematoma. J Neurosurg. 1988 Jan;68(1):58-61.
- Das, J. M., & Bajaj., J. (2023, January). Pneumocephalus – StatPearls – NCBI Bookshelf. Pneumocephalus. https://www.ncbi.nlm.nih.gov/books/NBK535412/
- Rajajee, V. (n.d.). Management of acute moderate and severe traumatic brain injury. UpToDate. https://www.uptodate.com/contents/management-of-acute-moderate-and-severe-traumatic-brain-injury#H17
- Castedo J, Ferreira AP, Camacho Ó. Hyperbaric oxygen therapy in the treatment of pneumocephalus associated with epidural block: case report. Braz J Anesthesiol. 2021 May-Jun;71(3):295-298
- González Tortosa J, Mendoza Roca A, Poza Poza M. Post-traumatic pneumocephalus, aggravated by hyperbaric chamber treatment.(article in Spanish) Neurocirugía. 1996;7:126–8
- Lim E, Lan BL, Ooi EH, Low HL. Pneumocephalus and air travel: an experimental investigation on the effects of aircraft cabin pressure on intracranial pressure. Sci Rep. 2020 Aug 12;10(1):13626.




