
Authors: Amelia Campbell, MD (EM Resident Physician, Carl R. Darnall Army Medical Center) and Alec Pawlukiewicz, MD (EM Attending Physician, Carl R. Darnall Army Medical Center) // Reviewed by: Joshua Lowe, MD (EM Attending Physician, USAF); Marina Boushra, MD (EM-CCM, Cleveland Clinic Foundation); Brit Long, MD (@long_brit); Alex Koyfman, MD (@EMHighAK)
Disclaimer: The views expressed in this post are those of the authors and do not reflect the official policy or position of the Department of the Army, DoD, or the US Government.
Case:
A 45-year-old woman presents to the emergency department (ED) with itching to bilateral palms. She endorses some fatigue, which she attributes to a stressful job transition, but has otherwise been in her usual state of health. Her triage vitals are within normal limits. Her examination is notable only for mild erythema to the palms of her hands and the soles of her feet with no discrete lesions. Her medical history is significant for hypertension, hyperlipidemia, and hypothyroidism. She takes lisinopril/hydrochlorothiazide, atorvastatin, and levothyroxine. She denies any history of allergies and does not use alcohol, drugs, or tobacco. She works as a gardener and wonders whether her pruritus could be due to a new pair of gloves she started wearing around the time of symptom onset. With that historical clue, contact dermatitis is high on the differential. However, a review of labs obtained from triage is notable for some abnormalities, an alkaline phosphatase (ALP) level of 403 with alanine aminotransferase (ALT) mildly elevated at 82.
What is the physiologic basis of her pattern of lab derangements?
What is the differential diagnosis for this clinical picture?
What further testing is indicated?
What is cholestasis?
Cholestasis describes obstruction of bile flow anywhere along its course from its production in hepatocytes to its delivery into the duodenum. Obstruction of bile flow is categorized by the anatomic location where it occurs, either extrahepatic or intrahepatic. A wide variety of conditions can result in either type of cholestasis (Figure 1).1 Extrahepatic obstruction is due to mechanical obstruction occurring downstream of the hepatic ducts such as pancreatic disease, gallstone obstruction of the common bile duct, and cancer. Intrahepatic cholestasis occurs due to a wide variety of inflammatory, autoimmune, infiltrative, space-occupying, toxicological, and systemic conditions affecting the synthesis and flow of bile through intrahepatic ducts. Several of these conditions are primarily injurious to hepatocytes but may present with cholestatic labs because a higher concentration of bile salts within hepatocytes stimulates the translation of alkaline phosphatase.2

What happens when bile flow is obstructed?
Obstruction of bile flow causes retrograde reflux of bile through the biliary system and back across the hepatocyte membrane, where it incorporates into hepatocyte membranes and causes cellular dysfunction and death.3 This process can lead to portal hypertension, hepatic cirrhosis, and increased risk of hepatocellular carcinoma.4 Failure of bile to reach the duodenum also results in malabsorption of fat-soluble vitamins, hyperlipidemia, and osteopenia/osteoporosis.5 Identification of obstructive physiology in the emergency department (ED) and referral for definitive management can spare patients from these damaging downstream consequences.
How does cholestasis present?
Cholestatic labs are often discovered incidentally as part of the workup of an unrelated ED complaint, although sometimes patients will present with cholestasis such as pruritis and jaundice. Pruritis is induced by bile acid accumulation, is typically worse in the evenings, and is most prominent in the palms and soles. 6 Jaundice and dark urine may occur but are not universal.6
History and physical exam are powerful tools in the initial evaluation of a patient with cholestatic labs. Past history should include an assessment of risk factors for hepatobiliary disease, including sexual history, history of intravenous drug use, recent abdominal or biliary surgery, family history of hepatobiliary disease, and medication history. Many common medications are known to cause drug-induced cholestasis.7 Antibiotics, particularly amoxicillin-clavulanate, are common offenders. Chlorpromazine, azathioprine, and oral contraceptives have also been implicated.8 The history of present illnesses can also reveal important clues to the etiology of cholestasis. A prospective study of 220 patients found that fever within the past 3 months and a longer duration of jaundice are independent predictors of intrahepatic cholestasis.9
How are cholestatic labs defined?
Blood tests for cholestasis include alanine aminotransferase (ALT), aspartate aminotransferase (AST), direct and indirect bilirubin, alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT), international normalized ratio (INR), and albumin. Of these, the only tests that provide information on the actual function of the liver itself are the INR, bilirubin, and albumin. All others are indirect indicators of damage to hepatic and biliary cells.10 Patterns of liver blood test derangements are typically divided into hepatocellular and cholestatic etiologies. A hepatocellular pattern primarily features elevated aminotransferases. ALP may also be elevated in hepatocellular disease but typically less than twice the upper limit of normal.1 In cholestatic injury, increased reflux of bile salts into hepatocytes causes increased translation of ALP. This increased translation results in ALP levels in the blood at three or more times the upper limit of normal. Aminotransferases will be normal or only slightly elevated (Table 1).3

A quantitative method of establishing a cholestatic versus. hepatocellular pattern is by using the R factor. The R factor is a ratio of the patient’s ALT and ALP compared to normal values and estimates the likelihood of hepatocellular vs. cholestatic injury (patient’s ALT ÷ upper limit of normal ALT)/(patient’s ALP ÷ upper limit of normal ALP). The American College of Gastroenterology recognizes a value of >5 as hepatocellular and <2 as cholestatic.1
Elevations in ALP, although suggestive of biliary injury, are not specific to the biliary tract. ALP is also found in bone, intestine, kidney, and placenta. It can be elevated in conditions that increase bone turnover, including accelerated growth during puberty and Paget’s disease.2 Therefore, the first step after identifying liver blood tests concerning for cholestatic injury is to confirm the ALP is from a biliary source. If ALP is elevated in conjunction with aminotransferases, the source may be assumed to be biliary, and further confirmation of the source is not required. If alkaline phosphatase is elevated in isolation, a GGT level should be obtained.1 GGT is an enzyme located on the plasma membrane of hepatocytes that is involved in the regeneration of glutathione. This enzyme is not expressed in significant concentrations in bone, so elevated GGT levels indicate a biliary rather than osseous source. Although more specific than ALP, GGT can also be elevated in extra-hepatic conditions including chronic alcohol use, pancreatic disease, myocardial infarction, renal failure, emphysema, and diabetes, and in patients taking certain medications such as phenytoin and barbiturates.11
Approach to Initial Imaging
After diagnosing cholestasis based on bloodwork, the next step is imaging to identify the anatomic location and potential etiology of the obstruction. This begins with localizing intrahepatic vs. extrahepatic obstruction. Extrahepatic disease is evidenced by dilation of the common bile duct (CBD). A normal CBD measures <5 mm in those <50 years old. The upper limit of normal increases by 1 mm with each decade above 50 years of age. Additionally, patients with prior cholecystectomy may have CBD dilation up to 10 mm without identifiable obstruction. Chronic opioid use can also cause incidental asymptomatic CBD dilation, up to 8 mm, without obstruction.12 Ultrasound and computed tomography (CT) can both identify CBD and are available in most emergency departments. Ultrasound is cost-effective and radiation-sparing. When available, it is an ideal starting point for most cases. Ultrasound has approximately 90% sensitivity for detecting common bile duct dilation. However, intestinal air can obscure the distal common bile duct in 40-50% of patients.7 It is also limited in its ability to delineate the anatomic level and specific etiology of obstruction. Estimates vary, but its sensitivity in identifying the level of obstruction ranges from 27-95%, and the etiology of obstruction from 23-81%.13
CT is 96% sensitive in identifying CBD dilation. It is superior to ultrasound for identifying both the level (88-97% sensitive) and the etiology (70-95% sensitive) of obstruction. However, 20-25% of biliary stones are iso-attenuating with bile and are thus difficult to identify on CT.7 Although unenhanced scans better highlight calcification associated with stones, IV contrast is generally required to visualize the bile ducts.13 CT is also superior to ultrasound in its ability to detect malignancy. If the patient complains of unexplained weight loss, night sweats, painless jaundice, and has concerning social and family history risk factors, CT would be the more prudent first test. A scan with biphasic pancreatic and portal venous phase contrast should be considered if feasible and suspicion for cancer is high since this protocol is used for staging malignancy.7
Subsequent imaging
If ultrasound and/or CT are nondiagnostic but clinical suspicion remains high for obstructive biliary pathology, the next step in evaluation is typically endoscopic retrograde cholangiopancreatography (ERCP) or magnetic resonance pancreatography (MRCP). A suggested algorithm for initial and subsequent imaging is provided below (Figure 2).

Endoscopic retrograde cholangiopancreatography (ERCP)
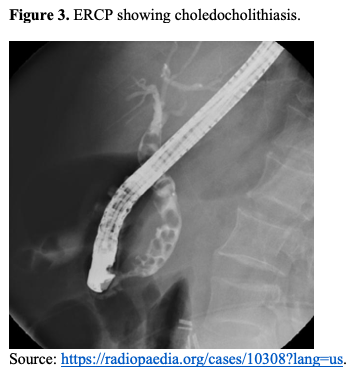
ERCP is the gold standard for the evaluation of the bile duct. It consists of the advancement of an endoscope through the mouth, into the descending duodenum, and into the ampulla of Vater, where contrast is injected to outline the biliary tree. Obstruction of bile flow is evidenced by a lack of contrast enhancement, as demonstrated by the large number of stones within the common bile duct in the image below (Figure 3). It is highly accurate, with the level of obstruction able to be determined in 87% to 98% of cases. In addition to its diagnostic capabilities, its advantages include the ability to perform therapeutic procedures such as stone retrieval and biliary stenting.13 ERCP has a complication rate of as high as 6.8% with the incidence of post-ERCP pancreatitis at 3.5%. Other complications include bleeding and perforation.13 Due to its relatively high risk of complications and advancements in less invasive imaging modalities, purely diagnostic indications for ERCP have decreased. Now it is typically only employed if therapeutic procedures are anticipated, such as in patients with sepsis due to ascending cholangitis requiring biliary intervention for source control. For patients unable to undergo ERCP or who fail initial attempts, cholangiography and biliary interventions may be performed percutaneously.14
Magnetic resonance cholangiopancreatography (MRCP)
MRCP is an imaging technique that exploits the physical properties of bile to selectively image the biliary system. Bile is easily distinguished using a heavily T2-weighted MRI sequence such that no exogenous contrast or radiotracer is required for visualization.15 MRCP is unique in that it visualizes the biliary tree above and below obstruction, as demonstrated by contrast enhancement above and below a common bile duct stone in the image below (Figure 4). Its sensitivity for detecting choledocholithiasis is 92% and its specificity is 97%. The sensitivity for malignancy is 88%, and the specificity is 95%.13 Its use is limited in patients with severe claustrophobia and implanted metallic devices. MRCP has no therapeutic capabilities but spares the patient from radiation and is an alternative diagnostic approach for patients unable to undergo ERCP.7 However, in a patient whose condition necessitates intervention, such as a patient with ascending cholangitis, ERCP, or percutaneous transhepatic biliary drainage will likely be required.

Endoscopic ultrasound (EUS)
Endoscopic ultrasound is another imaging modality used to evaluate the biliary system. Although it is most commonly used to evaluate for cholestasis due to malignancy (Figure 5), its sensitivity for choledocholithiasis is 94%. This is on par with ERCP, which is 83% sensitive for detecting CBD stones.16,17 EUS is a technique of accessing and imaging the upper GI tract in which an echoendoscope is guided through the mouth and advanced through the upper GI tract, where trans-gastric or trans-duodenal imaging of the biliary system can be obtained. Following diagnostic EUS, ERCP can be performed for biliary drainage, stenting, and tissue sampling. More recently, advances in device technology have allowed interventions to be performed solely via the ultrasound transducer without the requirement for ERCP. This provides an option for when conventional ERCP fails to achieve adequate biliary drainage or is not feasible for various reasons, including surgically altered abdominal anatomy.18

Next steps if cholestasis is present but common bile duct diameter is normal
Patients with cholestatic labs but imaging reassuring against extrahepatic cholestasis are likely to have intrahepatic cholestasis. These patients should be referred to gastroenterology on an outpatient basis unless their presentation otherwise warrants admission. During their outpatient evaluation, these patients will undergo further testing of liver function, evaluation for autoimmune disease, and consideration of liver biopsy.19
Approach to the unexpected imaging finding of common bile duct dilation
Sometimes, incidental dilation of the CBD is identified on imaging obtained for other reasons. In these cases, if there are associated abnormal imaging findings such as pancreatic duct dilation, intrahepatic duct dilation, biliary stones, excessive duct dilation (>10mm), an abrupt cutoff in duct dilation, or findings that are progressive compared to prior imaging, the patient should be referred for further evaluation. If the patient has no clinical signs or symptoms of obstruction (jaundice, pruritis, acholic stools, dark urine, weight loss, fever) and has no lab abnormalities suggestive of obstruction, then no further workup is warranted.20
Case Conclusion
A hepatic panel is ordered to further investigate her cholestatic labs, and due to her strongly suggestive clinical picture and autoimmune history, a right upper quadrant ultrasound is ordered to evaluate for extrahepatic cholestasis. Her GGT is elevated and her common bile duct diameter is normal on ultrasound. Due to concern for intrahepatic cholestasis, the patient is referred to a gastroenterologist, where she undergoes autoimmune testing that is positive for anti-mitochondrial antibodies. She is diagnosed with primary biliary cholangitis. She begins ursodeoxycholic acid treatment and receives close hepatic monitoring .
Pearls and Pitfalls
- Elevated ALP at three or more times the upper limit of normal should raise suspicion for cholestasis.
- Elevated ALP is a nonspecific lab finding that can originate from extrabiliary sources including bone, intestine, kidney, and placenta. If the elevation is isolated, obtain a GGT level to confirm the biliary source.
- The differential diagnosis for cholestasis is broad. ED assessment should focus on determining whether biliary obstruction is extrahepatic or intrahepatic. Once localized, further evaluation and treatment is usually guided by gastroenterology.
- CT and ultrasound are commonly obtained imaging modalities in the ED but both have their limitations in evaluating cholestasis. Consider consultation or referral to gastroenterology if the patient’s labs and clinical picture suggest cholestasis but their initial imaging is unrevealing.
- ERCP is the gold standard for common bile duct evaluation but other options including endoscopic ultrasound and percutaneous biliary drainage exist for patients unable to undergo ERCP.
References:
- Kwo PY, Cohen SM, Lim JK. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. American Journal of Gastroenterology. 2017;112(1):18-35. doi:10.1038/ajg.2016.517
- Lowe D, Sanvictores T, Zubair M, Savio ;, Affiliations J. Alkaline Phosphatase. https://www.ncbi.nlm.nih.gov/books/NBK459201/?report=printable
- Asensio M, Ortiz-Rivero S, Morente-Carrasco A, Marin JJG. Etiopathogenesis and pathophysiology of cholestasis. Exploration of Digestive Diseases. Published online October 31, 2022:97-117. doi:10.37349/edd.2022.00008
- Onofrio FQ, Hirschfield GM. The Pathophysiology of Cholestasis and Its Relevance to Clinical Practice. Clin Liver Dis (Hoboken). 2020;15(3):110-114. doi:10.1002/cld.894
- Hilscher MB, Kamath PS, Eaton JE. Cholestatic Liver Diseases: A Primer for Generalists and Subspecialists. Mayo Clin Proc. 2020;95(10):2263-2279. doi:10.1016/j.mayocp.2020.01.015
- Das KK, Kochman ML. Dilated Bile Duct and Pneumobilia.; 2018. doi:10.1016/B978-0-323-48109-0.00036-5
- Todd Taylor A, Wheatley M, Chung AS, et al. Jaundice in the Emergency Department: Meeting the Challenges of Diagnosis and Treatment. Hamad General Hospital. 2018;20. www.ebmedicine.net/topics
- Sundaram V, Björnsson ES. Drug-induced cholestasis. Hepatol Commun. 2017;1(8):726-735. doi:10.1002/hep4.1088
- Pasanen PA, Pikkarainen P, Alhava E, Partanen K, Janatuinen E. Evaluation of a computer-based diagnostic score system in the diagnosis of jaundice and cholestasis. Scand J Gastroenterol. 1993;28(8):732-736. doi:10.3109/00365529309098282
- Newsome PN, Cramb R, Davison SM, et al. Guidelines on the management of abnormal liver blood tests. Gut. 2018;67(1):6-19. doi:10.1136/gutjnl-2017-314924
- Kunutsor SK. Gamma-glutamyltransferase—friend or foe within? Liver International. 2016;36(12):1723-1734. doi:10.1111/liv.13221
- Vardar BU, Dupuis CS, Goldstein AJ, Vardar Z, Kim YH. Ultrasonographic evaluation of patients with abnormal liver function tests in the emergency department. Ultrasonography. 2022;41(2):243-262. doi:10.14366/usg.21152
- Das KK, Kochman ML. Dilated Bile Duct and Pneumobilia. In: ERCP, Third Edition. ; 2018:346-353.e2. doi:10.1016/B978-0-323-48109-0.00036-5
- Mishra A, Tyberg A. Endoscopic ultrasound guided biliary drainage: A comprehensive review. Transl Gastroenterol Hepatol. 2019;4(Febuary). doi:10.21037/tgh.2019.01.03
- Mudgal P, Chieng R, Murphy A. Magnetic resonance cholangiopancreatography. Radiopedia. Published 2023. https://radiopaedia.org/articles/magnetic-resonance-cholangiopancreatography-mrcp-2?lang=us
- Chen CC. The efficacy of endoscopic ultrasound for the diagnosis of common bile duct stones as compared to CT, MRCP, and ERCP. Journal of the Chinese Medical Association. 2012;75(7):301-302. doi:10.1016/j.jcma.2012.05.002
- Gurusamy KS, Giljaca V, Takwoingi Y, et al. Endoscopic retrograde cholangiopancreatography versus intraoperative cholangiography for diagnosis of common bile duct stones. Cochrane Database of Systematic Reviews. 2015;2015(2). doi:10.1002/14651858.CD010339.pub2
- DeWitt JM, Arain M, Chang KJ, et al. Interventional Endoscopic Ultrasound: Current Status and Future Directions. Clinical Gastroenterology and Hepatology. 2021;19(1):24-40. doi:10.1016/j.cgh.2020.09.029
- Yeh MJ, Kim SY, Jhaveri KS, Behr SC, Seo N, Yeh BM. Imaging of autoimmune biliary disease. Abdominal Radiology. 2017;42(1):3-18. doi:10.1007/s00261-016-0903-8
- Rizvi A, Poneros J, Sethi A, Visrodia KH. Q: Does incidentally detected common bile duct dilation need evaluation? Cleve Clin J Med. 2022;89(6):315-319. doi:10.3949/ccjm.89a.21029




