
Authors: Gillian Schmitz, MD (@GillianMD1, EM Attending Physician, San Antonio, TX) and Max Hockstein, MD (@MaxHockstein, Critical Care Fellow, Emory University) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Welcome back to emDocs Cases! Today we have case-based discussion on a core EM topic, with a look at some controversy and cutting-edge treatments.
Kidney stones result in an estimated 2.1 million annual visits to U.S. emergency departments (EDs) (1,2). Ureteric colic is defined as episodic, severe abdominal pain from sustained contraction of ureteric smooth muscle as a kidney stone passes down the ureter into the bladder (3). It is a common, but unfortunately, painful disorder, resulting in many patients seeking emergency health care. Although most patients can be safely discharged, some patients will suffer complications including urosepsis, perinephric abscess, and acute renal failure. The composition of calculi (including calcium, urate, struvite, etc.) are less germane in the emergency setting; the key to management lies solely in clinical presentation.
A 41-year old female with no prior history presents to the ED with sudden onset left flank pain and nausea with vomiting. She has no fevers but has some dysuria. She is not pregnant. She is leaving for vacation next week and wants to know if this could be a kidney infection or a kidney stone, or both. If it’s a stone, what is the likelihood of it passing?
Clinically, it can sometimes be challenging to differentiate renal colic from pyelonephritis from nephrolithiasis with an obstructed stone. Patients with these conditions may all present with back or flank pain, dysuria, hematuria, frequency, and CVA tenderness.
In general, the likelihood of spontaneous passage is inversely proportional to the size of the stone. If a stone is present, the likelihood that her stone will pass within 4 weeks ranges between 50% and 95%, depending on stone size and location in the ureter (4,5). The narrowest part of the ureter is at the ureterovesicular junction (UVJ) and is thus a common area for stones to become lodged.
Her CT scan shows a 5 mm stone in the proximal ureter.Let’s say her urine analysis shows some hematuria along with 8 WBCs. She has no fever. Does the absence of fever reassure us?
About 8% of patients presenting with acute nephrolithiasis will also have a urinary tract infection (UTI), defined as growth of a single uropathogen at greater than or equal to 103 colony-forming units/mL (11). The presence of fever was absent in 50% of patients with kidney stone and confirmed UTI. Let that sink in for a minute. Fever was absent in half the patients! Ok, so we can’t use absence of fever to rule out an infected stone.
How about physician gestalt after reviewing the vitals and urine results?
Not great. Of patients who were given empiric antibiotics for presumed UTI with stones, almost 70% were not infected according to the final urine culture. Conversely, 20% who were not treated with antibiotics actually had an infection based on urine culture (11).
How sensitive and specific is pyuria, leukocyte esterase, and nitrites for a concomitant UTI in the setting of nephrolithiasis? And how useful is hematuria in kidney stones in general?
The urinalysis is a common test in the ED and can provide a lot of useful information. As 8% of patients with acute nephrolithiasis have UTI’s and can result in all complications of sepsis, the UA has historically been an important test (11). As we’ve seen thus far, however, it’s an imperfect test.
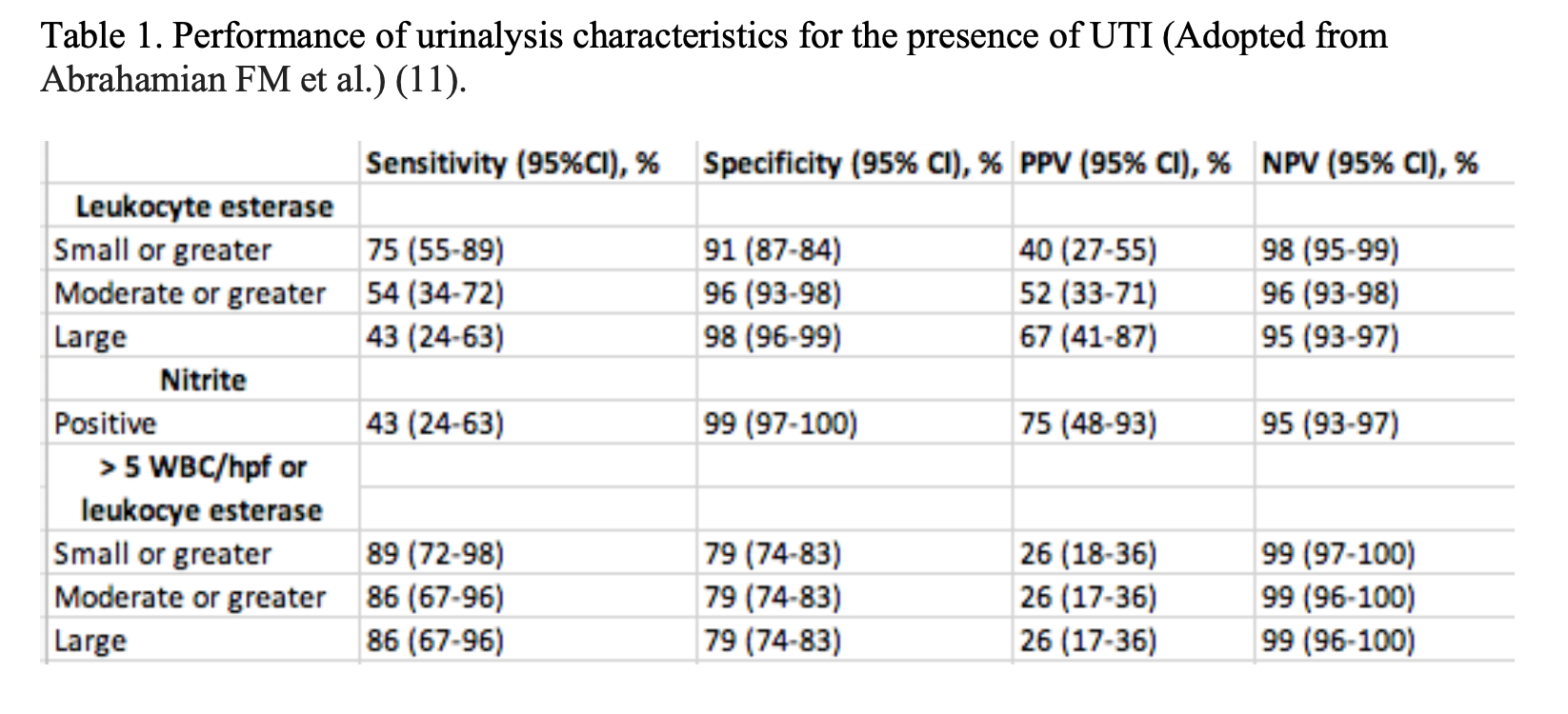
Pyuria has only a moderate accuracy in identifying UTI in this setting. The table below lists the performance characteristics of the urinalysis in patients with acute nephrolithiasis (11). The sensitivity and specificity of pyuria for the culture confirmed diagnosis of UTI without a stone has been reported to be 47% to 90% and 47% to 89%, respectively, depending on the extent of pyuria and bacterial concentration used to define UTI (4-10).
It is important to diagnose UTI’s in patients with nephrolithiasis because they are at higher risk for urosepsis, abscess, or pyonephrosis as a result of “pus behind pressure” (11). A UTI in the setting of an obstructed stone is a urologic emergency (12,13).
The absence of hematuria has also been canonically taught as a reliable way to rule out acute renal calculi. The accuracy of hematuria as an indicator for acute renal calculi has been cited at 60.9%, and thus its absence cannot exclude calculi (14). The presence of hematuria, however, is most common during the first day of disease, and 80% of patients experience either micro- or macroscopic hematuria at some point during their disease course (11).
Does perinephric stranding or hydronephrosis on imaging accurately predict UTIs in the presence of a kidney stone?
Perinephric stranding was present in approximately half of patients with and without UTI. Hydronephrosis was present in 46% of patients with UTI and 63% of patients without UTI (11). Based on these findings, neither finding can rule out UTI in the setting of urolithiasis.
So how do we know if she has an obstructed stone with a UTI?
Patients with kidney stones should have both a UA and urine culture sent. Because the UA is not always diagnostic and patients may not have symptoms of UTI, a culture is needed to determine infection and antibiotic sensitivities. Clinical features of UTI, a greater degree of pyuria, and female sex increases the likelihood of infection (11).
Do all patients with ureteral stones and UTI require admission?
Patients with obstructing kidney stones and UTI’s are considered urologic emergencies, and many texts and references recommend admission (15).
Not all patients with kidney stones and UTI develop severe sepsis, however, and obtaining a urine culture and ensuring short term follow up of clinical status and culture results may be sufficient for some patients. Caution is emphasized for patients with fever, hypotension, signs of systemic illness, medical co-morbidities, and high grade ureteral obstruction who appear to be at greatest risk of severe infection (11). These patients likely require admission.
Disposition for a patient with UTI with a smaller stone and without sepsis should be discussed with a urologist.
Most patients with kidney stones can be discharged. Which other patients need to be admitted?
It is important to obtain a good history to predict which patients are at risk for poor outcomes with a stone. Consideration for admission should be considered in patients who have renal function at risk (AKI from diabetes or HTN, single, horseshoe, or transplanted kidney), patients with a history of difficult stone passage (extractions, stents, ureterostomy tubes, and lithotripsy), and signs of infection (fever, hypotension, systemic illness, and UTI).
During acute obstruction, most patients will not have a rise in their serum creatinine because the other kidney is able to compensate. A rise in serum creatinine in acute obstruction suggests a solitary kidney or pre-existing renal disease. Patients with urosepsis, acute renal failure, intractable pain or vomiting, or single or transplanted kidney with obstruction should be admitted (15).
A 36-year old male is found to have a 4 mm stone in the left UVJ with some associated hydronephrosis of the left kidney. His urine is normal, and he has no fevers or signs of toxicity. The radiologist read indicated a partially obstructing stone. It’s 3 AM. Does the presence of hydronephrosis indicate an emergency requiring immediate urologic consultation?
The presence of hydronephrosis and hydroureter do not necessarily indicate an obstruction, and many urologists do not consider the presence of hydronephrosis or hydroureter to be a urologic emergency. In one study based on ultrasound, up to 22% of hydronephrosis was not caused by obstruction, but rather normal anatomic variants, full bladders, and renal cysts (16). Rapid infusion of crystalloid can also result in false positives of hydroureter or hydronephrosis.
Most patients have incomplete ureteral obstruction and can be safely discharged with outpatient follow up. Even with complete obstruction, it is unlikely to change the disposition of the patient until his or her symptoms are not controlled or the patient manifests signs of an infection. Irreversible renal damage from an obstructive kidney stone is rare unless obstruction has been present for over one month (17).
OK, so we’ve talked a lot about ureteral stones. We know stones in the actual renal pelvis generally do not cause pain unless they are temporarily blocking urinary outflow at the entrance of the ureter. When do stones in the renal pelvis become an emergency?
Struvite (magnesium-ammonium phosphate) stones make up 10-15% of kidney stones. These stones often cause staghorn calculi, forming a cast in the renal pelvis, and are associated with infection from urea-splitting bacteria. Proteus, Klebsiella, Staphylococcal species, Providencia,and Corynebacteriumcan raise the pH of the urine > 7.2. Because antibiotic penetration in staghorn calculi is poor, the potential for urosepsis is increased until the stone is removed. Surgical treatment is generally required for staghorn calculi (15).
A 49-year old male presents with flank pain that feels identical to his prior episodes of renal colic. He is concerned about the number of CT scans he has had over the course of his lifetime as his urologist has mentioned the radiation risk. He wants to know if you can order an ultrasound and what the limitations of that test are.
Ultrasonography has the potential to aid in the diagnosis of symptomatic stones by visualization of the stones directly or through secondary signs of obstruction, i.e. hydronephrosis, without exposing patients to ionizing radiation (2). Studies of emergency physician–performed ultrasonography have reported sensitivities ranging from 72% to 97% and specificities ranging from 69% to 83% (18-22).
CT scanning has rapidly become the first-line imaging modality for renal colic in U.S. ED’s (23-25). Although 70% of patients diagnosed with ureterolithiasis receive a CT, there has not been a significant change in patient centered-outcomes (26-28). Given the radiation risk with repeated CT use, it would be helpful to determine safe and alternative means of imaging and identifying lower and high-risk patients.
A multicenter, randomized trial evaluating patients with suspected renal colic in the ED demonstrated the noninferiority of ultrasonography compared with CT with respect to diagnosis of symptomatic stones and identification of significant alternative diagnoses (29). The study concluded that ultrasonography can be used as the initial diagnostic imaging test, with further imaging performed at the discretion of the physician based on clinical judgment. Clinical prediction tools have been used to risk stratify patients to help identify patients who are more likely to have uncomplicated ureteral stones or need for urologic intervention (2).
Ultrasound is not sensitive for imaging mid-ureteral stones, but it has 98% sensitivity in detecting hydronephrosis. Although hydronephrosis is not specific for obstruction, as we discussed earlier, the absenceof hydronephrosis may help risk stratify those with smaller non-obstructing stones. This must be used in patients with a high pre-test probability of having a kidney stone, as ultrasound is less diagnostic at identifying other emergent causes of flank pain. CT should still be used in patients with unclear diagnosis or high risk for other emergency conditions, i.e. AAA or aortic dissection.
In a patient with a history of uncomplicated stones and classic features of renal colic, shared decision making can be used. In this subgroup, a negative ultrasound (no evidence of hydronephrosis) may obviate the need for CT, as the likelihood of spontaneous stone passage without urologic intervention is high.
The same 49-year-old male recalls that he was given a medicine that started with either an “f” or a “t” last time he had a kidney stone – he wants to know if he’s going to receive the same medication today.
The usage of medical expulsive therapy (MET) has been long-debated in the outpatient treatment of kidney stones. Two large classes of medications have been evaluated in literature: alpha-1 blockers and calcium channel blockers; however, the most popular drug used in this setting is tamsulosin. The ureter has varying concentrations of alpha receptors which, when blocked, theoretically augment stone passage. It should be noted that use of MET should only be considered in the patient population that does not require urgent surgical attention.
A Cochrane review of α-blockers reported a significant improvement in stone passage (30). However, most trials included in this review were not placebo controlled and blinded and were considered at moderate to high risk of bias; only 7 of 32 trials were double blinded. Two subsequent multicenter randomized placebo-controlled trials did not show a significant benefit of tamsulosin, except in a recent randomized trial, which suggested a benefit in a subgroup with larger stones (5 to 10 mm) (5,31). Other studies have suggested that alpha-1 blockers may only be useful in the setting of large stones (> 5 mm) (32).
The most recent study, a randomized trial, noted that there was no benefit to the administration of tamsulosin for stones < 9 mm (33). It is possible that there could be benefit for stones > 9 mm, but more study is needed for this subset. These conflicting results have led to considerable uncertainty in regard to the efficacy of tamsulosin for increasing the passage of ureteral stones (34).
Key Points:
– The combination of an obstructed stone with a UTI is a urologic emergency. About 8% of patients presenting with acute nephrolithiasis will also have a UTI.
-Patients with decreased renal function, previous urologic interventions, and symptoms of infection are historical features for poor outcome in patients with stones.
-The presence of pyuria has only moderate sensitivity in patients with positive urine cultures.
–Fever was absent in 50% of patients with stone and confirmed UTI.
– Hydronephrosis and hydroureter may be secondary signs of ureteral obstruction. However, this finding is not specific and can be caused by other things including rapid administration of IV fluids.
-In a subset of low risk patients, renal ultrasound may be an alternative to CT imaging without exposing patients to ionizing radiation. The absence of hydronephrosis in these patients may predict the spontaneous passage of stone without urologic intervention.
–Antibiotic penetration in staghorn calculi is poor, the potential for urosepsis is increased until the stone is removed. Surgical treatment is generally required for staghorn calculi.
– Patients with acute flank pain have many etiologies, including cardiovascular and pulmonary catastrophes. Isolated kidney stones should not cause shock.
References/Further Reading:
- Hyams ES, Korley FK, Pham JC, et al. Trends in imaging use during the emergency department evaluation of flank pain. J Urol. 2011;186:2270-2274.
- Daniels B, Gross CP, Molinaro A, Singh D, Luty S, Jessey R, Moore CL. STONE PLUS: Evaluation of Emergency Department Patients With Suspected Renal Colic, Using a Clinical Prediction Tool Combined With Point-of-Care Limited Ultrasonography. Ann Emerg Med. 2016 Apr;67(4):439-48.
- Bultitude M, Rees J. Management of renal colic. BMJ 2012; 345: e5499.
- Miller OF, Kane CJ. Time to stone passage for observed ureteral calculi: a guide for patient education. J Urol 1999; 162: 688–91.
- Pickard R, Starr K, MacLennan G et al. Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial. Lancet2015; 386: 341–49.
- Bailey BL. Urinalysis predictive of urine culture results. J Fam Pract. 1995;40:45-50.
- Lammers RL, Gibson S, Kovacs D, et al. Comparison of test characteristics of urine dipstick and urinalysis at various test cutoff points. Ann Emerg Med. 2001;38:505-512.
- Weinberg AG, Gan VN. Urine screen for bacteriuria in symptomatic pediatric outpatients. Pediatr Infect Dis J. 1991;10:651-654.
- Goldsmith BM, Campos JM. Comparison of urine dipstick, microscopy, and culture for the detection of bacteriuria in children. Clin Pediatr. 1990;29:214-218.
- Lohr JA, Portilla MG, Geuder TG, et al. Making a presumptive diagnosis of UTI by using a urinalysis performed in an on-site laboratory. J Pediatr. 1993;122:22-25.
- Abrahamian FM, Krishnadasan A, Mower W. et al. Association of Pyuria and Clinical Characteristics with the Presence of UTI Among Patients with Acute Nephrolithiasis. Ann Emerg Med. 2003;62 (5):526-533.
- Neal DE. Complicated UTIs. Urol Clin North Am. 2008;35:13-22.
- Ohkawa M, Tokunaga S, Nakashima JT, et al. Composition of urinary calculi related to UTI. J Urol. 1992;148:995-997.
- Safriel Y, Malhotra A, Sclafani SJ. Hematuria as an indicator for the presence or absence of urinary calculi. Am J Emerg Med. 2003;21(6):492-493.
- Tintinalli’s Emergency Medicine. 7thedition.
- Koelliker SL, Cronan JJ: Acute urinary tract obstruction: imaging update. Urol Clin North Am 24:571,1997.
- Teichman JM: Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 350: 684,2004.
- Dalziel PJ, Noble VE. Bedside ultrasound and the assessment of renal colic: a review. Emerg Med J. 2012;30:3-8.
- Goertz JK, Lotterman S. Can the degree of hydronephrosis on ultrasound predict kidney stone size? Am J Emerg Med. 2010;28:813-816.
- Erwin B, Carroll B, Sommer F. Renal colic: the role of ultrasound in initial evaluation. Radiology. 1984;152:147-150.
- Gaspari RJ, Horst K. Emergency ultrasound and urinalysis in the evaluation of flank pain. Acad Emerg Med. 2005;12:1180-1184.
- Gleyzer A, Sinert R. Emergency ultrasound in the evaluation of flank pain: limited data. Acad Emerg Med. 2006;13:704-705.
- Moore CL, Scoutt L. Sonography first for acute flank pain? J Ultrasound Med. 2012;31:1703-1711.
- Noble VE, Brown DF. Renal ultrasound. Emerg Med Clin North Am. 2004:651-659.
- Kartal M, Eray O, Erdogru T, et al. Prospective validation of a current algorithm including bedside US performed by emergency physicians for patients with acute flank pain suspected for renal colic. Emerg Med J. 2006;23:341-344.
- Westphalen AC, Hsia RY, Maselli JH, et al. Radiological imaging of patients with suspected urinary tract stones: national trends, diagnoses, and predictors. Acad Emerg Med. 2011;18:699-707.
- Cupisti A, Pasquali E, Lusso S, et al. Renal colic in Pisa emergency department: epidemiology, diagnostics and treatment patterns. Intern Emerg Med. 2008;3:241-244.
- Türk C, Knoll T, Petrik A, et al. Guidelines on urolithiasis. Eur Assoc Urol. 2011.
- Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N Engl J Med. 2014;371:1100-1110.
- Campschroer, T., Zhu, Y., and Duijvesz, D. Alpha-blockers as medical expulsive therapy for ureteral stones. (CD008509)Cochrane Database Syst Rev. 2014; 4
- Furyk JS, Chu K, Banks C, et al. Distal Ureteric Stones and Tamsulosin: A Double-Blind, Placebo-Controlled, Randomized, Multicenter Trial. Ann Emerg Med. 2016;67(1):86-95.e2
- Hollingsworth JM, Canales BK, Rogers MAM, et al. Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ. 2016;355:i6112
- Meltzer AC, Burrows PK, Wolfson AB, et al. Effect of Tamsulosin on Passage of Symptomatic Ureteral Stones: A Randomized Clinical Trial. JAMA Intern Med. June 2018. doi:10.1001/jamainternmed.2018.2259
- Wang RC, Smith-Bidman R, Whitaker E. Effect of Tamsulosinon Stone Passage for Ureteral Stones: A Systematic Review and Meta-analysis. Ann Emerg Med. 2017 Mar;69(3):353-361




