Today on the emDOCs cast with Brit Long, MD (@long_brit), we look at malignant otitis externa.
Episode 72: Malignant Otitis Eterna
Introduction:
- Malignant otitis externa (MOE) is a severe and progressive infection of the external auditory canal.
- MOE has also been called necrotizing otitis externa and skull base osteomyelitis.
- First described as a case of progressive Pseudomonas osteomyelitis of the temporal bone in a diabetic patient in 1959.
- Pathophysiology includes osteomyelitis of the skull base osteomyelitis.
- MOE begins as an infection of the external ear canal and spreads to the temporal bone and skull base and can affect the jugular foramen and other intracranial structures. Water exposure is often implicated.
- Prior to the use of antibiotics, MOE had rates of death reported up to 50%. This disease still carries a high morbidity and mortality, with current rates of mortality estimated as high as 20%.
Risk factors:
- The most common risk factor for MOE is diabetes mellitus (DM), with an estimated 90% of patients with MOE having DM. DM is thought to predispose patients to MOE due to microangiopathy, impaired wound healing, increased pH in diabetic cerumen.
- Immunosuppression is another risk factor, including HIV or transplant recipient. MOE should be suspected when these patients present with symptoms of otitis externa.
- There are case series that report lower rates of DM and immunosuppression, with the only risk factor for MOE being age >65 years.
- An analysis of 8,300 patients who were hospitalized due to MOE found that elderly patients (>65 years of age) had greater in-hospital complications and greater mortality.
- A case series from 1984 reported several cases of MOE in patients with no underlying medical condition causing them to be immunocompromised, with the only major identified risk factor being advanced age.
- The disease is rare in children (< 20 reported cases).
Organisms:
- Pseudomonas aeruginosa is the most common causative agent of MOE, as it can grow in water and may colonizes the EAC in a moist environment or after trauma. Most common cause in DM and overall. Most studies suggest it is present in up to 95% of cases.
- In 1988, a literature review of 280 cases of MOE found that 99.2% of cases were due to Pseudomonas
- However, a study in 2010 by Chen et al. reported a 26.9% of Pseudomonas infection in their patient cohort of 26 patients. The next common pathogen identified was Klebsiella pneumoniae (19.2%), followed by fungal species (15.4%).
- Not all patients have just Pseudomonas; there are other bacterial causes.
- Another case series from 2010 evaluated a cohort of 51 patients with MOE; Pseudomonas accounted for 34% of isolated causative pathogens.
- Recent studies suggest 30% of infections grow Staphylococcus aureus, with 1/3 of these MRSA.
- In a 2014 retrospective case series of 29 patients, nine patients (45%) had cultures that grew Pseudomonas aeruginosa. Three patients (15%) had cultures that grew MRSA.
- Fungal causes of MOE have also been reported, especially in those with HIV/immunocompromise.
- The most common fungal organism is Aspergillus fumigatus. Others include Candida species.
- Pseudomonas infections in HIV patients occur with CD4 less than 100 and Aspergillus associated MOE with CD4 less than 50.
Clinical Manifestations
- Severe unremitting otalgia, aural fullness, otorrhea, and hearing loss. Otalgia is often worse at night and with chewing.
- Patients have often failed topical treatments for otitis externa.
- Fever and other systemic findings are not common.
- Pain out of proportion to exam is a red flag for MOE.
- Hallmarks on exam include purulent otorrhea with a swollen, tender external auditory canal.
- Granulation tissue or exposed bone is often present on the floor of the canal at the bony-cartilaginous junction.
- Patients with immunosuppression/HIV may lack typical granulation tissue along the floor of the external auditory canal.
- The TM is usually normal.
- As osteomyelitis affects the skull base and even TMJ, cranial nerve palsies may occur. The facial nerve is the most commonly involved cranial nerve. Less frequently involvement of the jugular foramen leads to CN IX, X, and XI deficits.
- Late conditions include dural sinus thrombosis, meningitis, and cerebral abscess (late findings that portend a poor prognosis).
- Consider MOE in patients who have severe OE, even if they do not possess the classic risk factors of DM and immunosuppression.
- Patients may have undiagnosed DM or even immunosuppression.
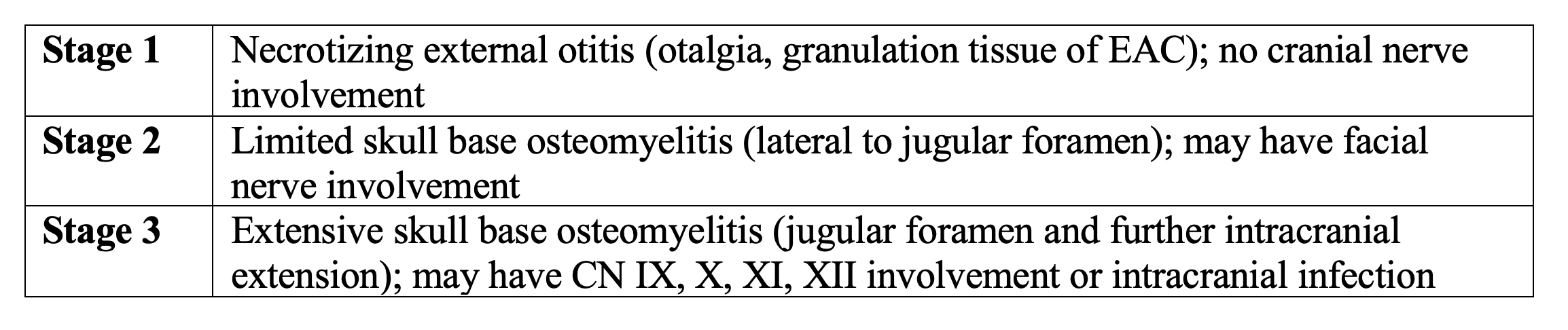
- There is a system for staging severity, ranging from stage 1 to 3.
Severe MOE:
- Factors associated with poor outcomes include CN VII palsy, fungal etiology of MOE, relapse of MOE, need for surgery, and major radiographic findings were associated with a poor prognosis.
- Severe with radiographic criteria: findings of bone erosion, intracranial involvement, or nasopharyngeal involvement.
- Higher mortality risk in patients with severe radiographic criteria (42% mortality) compared to non-severe cases (0%).
Diagnosis:
- Diagnosis in the ED should be based on combination of history and exam; labs can be obtained but cannot exclude diagnosis.
- Labs: CBC, inflammatory markers, culture of otorrhea.
- WBC is usually normal.
- ESR and CRP may be elevated in MOE.
- Culture (bacterial and fungal) of otorrhea is recommended.
- Imaging
- First line is CT of the temporal bones
- Useful in detecting bony erosion and decreased skull-based density, abscess formation.
- Bone erosion and decreased skull base density may not be present in early MOE.
- Controversial if useful for determining prognosis/resolution.
- MRI
- Better than CT for soft tissue changes, especially early in the disease or with involvement of the medial skull based and medullary bone spaces.
- Involvement of the retrocondylar fat pad on MRI may be an early diagnostic finding.
- MRI is better for determining disease extent and monitoring response to therapy.
- Others: Gallium and bone scanning are other options but not available in the ED. They may be more specific.
- First line is CT of the temporal bones
Treatment:
- Consult ENT specialist.
- Antibiotic therapy is the mainstay, primarily covering There is no clearly recommended single regimen.
- Antibiotics regimen should be based on disease severity. Treatment for 6-8 weeks is generally needed.
- Immunocompetent patients with more mild, uncomplicated, disease => Fluoroquinolone such as ciprofloxacin can be utilized.
- Fluoroquinolones cover Pseudomonas and have excellent bone penetration.
- Ciprofloxacin is the most commonly studied.
- Long-term monotherapy with oral ciprofloxacin (750mg PO BID) has been proposed as the initial antibiotic regimen. If admitted, start with IV ciprofloxacin and transition to PO as patient improves.
- However, ciprofloxacin has poor gram-positive coverage and does not cover MRSA. If concern for MRSA is present, provide gram positive coverage.
- Resistance of pseudomonas to therapy with ciprofloxacin may vary greatly across different settings, with resistance up to 30-33% reported.
- For patients with toxic appearance/sepsis, significant bony erosion, cranial neuropathies, immunocompromise, administer a fluoroquinolone with an antipseudomonal beta-lactam and admit the patient.
- Piperacillin/tazobactam, cefepime, OR meropenem PLUS a fluoroquinolone.
- Add MRSA coverage if concern for MRSA present.
- If immunocompromise/HIV, culture positive for fungal species speak with ID and admit. Antifungal therapy is often necessary.
- Options include voriconazole or liposomal amphotericin B. RCT data suggests voriconazole may be more effective. Isavuconazole is a newer antifungal that may be used.
- Interventions with limited role:
- No role for topical antibiotics – these decrease culture yield.
- Surgical excision usually plays no role; debridement and/or biopsy to exclude cancer may be performed.
- Hyperbaric oxygen may be an adjuvant therapy for refractory cases, but a Cochrane review found no clear evidence demonstrating efficacy.
- Disposition depends on patient appearance, disease severity (bony erosion/cranial nerve palsies), patient hemodynamic status, pain status, and consultation.
- Patients with adequate pain control, no immunocompromise, no cranial nerve involvement, and ENT follow up may be appropriate for discharge with oral antibiotics.
References:
- Long DA, Koyfman A, Long B. An emergency medicine-focused review of malignant otitis externa. Am J Emerg Med. 2020 Aug;38(8):1671-1678.
- Treviño González JL, Reyes Suárez LL, Hernández de León JE. Malignant otitis externa: An updated review. Am J Otolaryngol. 2021 Mar-Apr;42(2):102894.




