Authors: Katey DG Osborne, MD (EM Attending Physician: Tacoma, WA) and Rachel Bridwell, MD (EM Attending Physician: Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital); Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX)
Welcome to emDOCs revamp! This series provides evidence-based updates to previous posts so you can stay current with what you need to know.
A 43-year-old male, with no significant medical history, presents to the ED for right eye pain. The patient notes his pain as constant and sharp (8/10); associated with light-sensitivity, tearing, and blurred vision. He reports onset of his symptoms while mowing his lawn just prior to arrival and reports that he was not wearing eye protection. The man does not use glasses or contact lenses. He denies known ocular trauma or ocular surgical history.
Triage VS: BP 136/86 mm Hg, HR 110 bpm, T 98.6 F oral, RR 14 bpm, SpO2 98% on room air.
OD: 20/30
OS: 20/20
OU: 20/20
Pertinent physical examination findings:
Eyes: PERRLA, 3 mm bilaterally; No consensual photophobia; EOM and visual fields intact bilaterally.
OD: Mild conjunctival injection, no FB on lid eversion. Examination under Wood’s lamp with fluorescein stain demonstrates and irregular defect at the 2 o’clock position (image below)
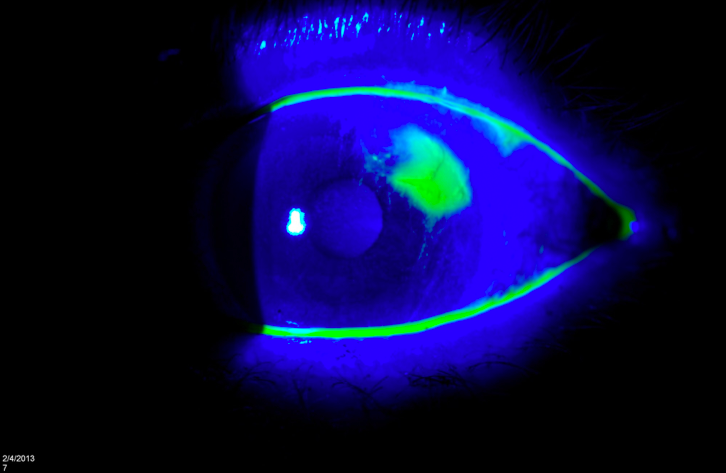
What is the diagnosis?
Answer: Corneal Abrasion1-12
Epidemiology
- Ocular diagnoses comprise 8% of total ER visits with 45% of those being corneal abrasions.1
- Corneal epithelium is easily damaged, however, regenerates quickly with a healing time of 24-48 hours.2
- Associated findings or complications include traumatic iritis, hypopyon, or a corneal ulcer.3
Risk Factors1
- History of trauma
- Contact lens wearer
- Male gender
- Lack of eye protection
- Construction or manufacturing job
Clinical Presentation
- Patients often report eye pain, red eye, foreign body sensation, eye watering/tearing, decreased visual acuity, and photophobia.
- Older children typically present like their adolescent/adult counterparts, however, infants and toddlers can present with inconsolability and a red eye.
Evaluation
- Ask specifically about patients’ work environment, materials involved, and if they are aware of the inciting event
- Manage pain and blepharospasm with topical anesthetic (e.g. tetracaine, proparacaine) to facilitate the exam.
- Pain relief with instillation is highly suggestive of corneal abrasion with appropriate clinical history.
- Conduct thorough ocular examination to include pupillary reactivity, visual acuity, extraocular motility, and lid eversion.
- Evidence of a misshapen or peaked pupil or large, non-reactive pupil are signs concerning for open globe or evidence of intra-ocular foreign body
- Visual acuities are likely to be normal unless the abrasion is over to visual axis or the abrasion is associated with iritis2
- Affected eye will likely show reactive miosis
- Patients’ conjunctiva will be injected and if presenting later will show signs of ciliary flush
-
- Examination with a slit lamp and fluorescein dye is ideal.
- Instill fluorescein by moistening the strip with a drop of saline or topical anesthetic. Pull down the patient’s lower lid and gently swipe against the bulbar conjunctiva.
- Application of the strip directly to the eye can be challenging, especially in children and there are multiple methods for instilling fluorescein into a flush for easy application.4
- After staining, the abrasion will be apparent to the naked eye and will be enhanced with the use of a Wood’s lamp or cobalt blue filter (ophthalmoscope / slit lamp).5
- Assess for open globe with Seidel’s test: fluorescein streaming away from a noted defect/abrasion.
- An abrasion will present as a superficial, irregular defect2
- If presenting more than 24 hours after onset of symptoms, there may be evidence of cell and flare in the anterior chamber due to concomitant iritis.2
- Instill fluorescein by moistening the strip with a drop of saline or topical anesthetic. Pull down the patient’s lower lid and gently swipe against the bulbar conjunctiva.
- Evert the upper lid to assess for foreign body (FB):
- Maintain high suspicion in a patient whose cornea is marred by numerous vertical, linear, abrasions.2
- If found, or still high suspicion, remove by using a clean cotton tip applicator and gently sweep the palpebral conjunctiva.6
- Examination with a slit lamp and fluorescein dye is ideal.
Treatment:
- Prescribe a topical antibiotic
- Non-contact lens wearers
- Erythromycin ointment four times daily – ointment preferred to help provide comfort & lubrication
- Avoid ointments containing neomycin due to hypersensitivity reactions7
- Contact lens wearers
- Cover for Pseudomonas with topical tobramycin or fluoroquinolones four times daily (e.g. ofloxacin or moxifloxacin)
- Fluoroquinolone drops are acceptable in children due to limited systemic absorption7
- Non-contact lens wearers
- Provide outpatient analgesia
- Topical NSAIDs (diclofenac, ketorolac) offer little advantage for pain relief to oral NSAIDs and cost more8
-
- Topical anesthetics are not recommended for home use9–12:
- There has been advocation for the use of topical anesthetics in the short-term management of corneal abrasions, however, there is limited data showing pain control compared to that of placebo or NSAIDs.
- Additionally, there is concern posed by ophthalmologists for development of keratopathy, delayed healing, worsening of injury, or delayed follow-up; this remains a debated topic between emergency medicine physicians and ophthalmologists.
- Topical anesthetics are not recommended for home use9–12:
- Cycloplegic use showed minimal reduction in pain scores compared to placebo.2
- Patching does not promote healing but can help with comfort for large abrasions 2
- Contraindicated in contact lens wearers, abrasions caused by organic materials or fingernails as this can increase risk for infection
- Not indicated for small abrasions
Consult Ophthalmology5:
- Findings concerning for open globe (positive Seidel test).
- Evidence of corneal infiltrate or opacity concerning for corneal ulceration
- Inability to remove retained FB
- Presence of hypopyon or hyphema
Disposition:2,6,7
- Most small corneal abrasions heal within 24-48 hours and follow-up may not be necessary in the reliable patient with resolution of symptoms.
- Urgent Ophthalmology follow-up in 24-48 hours:
- Large abrasions (< 50%) of corneal epithelium or those in the central visual axis
- A drop in vision of > 1 line on the Snellen Chart
- Continued symptoms after 3-4 days as this could suggest infection, FB, or progression.
- Recent surgery to affected eye
- Involvement of only functional eye
- Ophthalmology Referral:
- Recurrent corneal abrasions
- Dry eyes
Pearls:
- In the inconsolable toddler or infant, consider a corneal abrasion
- Keep high suspicion for open globe in the setting of high-speed mechanism of injury
- Topical anesthetics (e.g. tetracaine) not advised for home use at this time due to safety risks
- Topical NSAIDs offer minimal benefit compared to oral NSAIDs
- Antibiotic recommendations include erythromycin QID for non-contact lens wearers and tobramycin or fluoroquinolone ophthalmic gtts for contact lens wearers
For Additional Reading:
Taming of the SRU: https://www.tamingthesru.com/blog/bread-butter-em/corneal-abrasions
REBEL EM: https://rebelem.com/corneal-abrasions-and-short-term-topical-tetracaine/
Ophthalmologic Medications: Pearls & Pitfalls in the ED:
References:
- Ahmed F, House RJ, Feldman BH. Corneal Abrasions and Corneal Foreign Bodies. Prim Care Clin Off Pract. 2015;42(3):363-375.
- Walker RA, Adhikari S. Eye Emergencies. In: Tintinalli JE, Ma OJ, Yealy DM, et al., eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 9th ed. McGraw-Hill Education; 2020. Accessed October 2, 2023.
- Knoop KJ, Palma JK. Corneal Abrasion. In: Knoop KJ, Stack LB, Storrow AB, Thurman RJ, eds. The Atlas of Emergency Medicine. 5th ed. McGraw-Hill; 2021. Accessed October 2, 2023.
- DO SS. Tricks of the Trade: Fluorescein application techniques for the eye. ALiEM. Published June 11, 2015. Accessed October 22, 2023. https://www.aliem.com/tricks-of-the-trade-fluorescein-eye/
- Corneal abrasions and corneal foreign bodies: Clinical manifestations and diagnosis – UpToDate. Accessed October 22, 2023. https://www.uptodate.com/contents/corneal-abrasions-and-corneal-foreign-bodies-clinical-manifestations-and-diagnosis?search=corneal%20abrasion&source=search_result&selectedTitle=1~93&usage_type=default&display_rank=1#H6
- Shahid SM, Harrison N. Corneal abrasion: assessment and management. InnovAiT. 2013;6(9):551-554.
- Kircher J, Dixon A. Eye Emergencies in Infants and Children. In: Tintinalli JE, Ma OJ, Yealy DM, et al., eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 9th ed. McGraw-Hill Education; 2020. Accessed October 21, 2023.
- Wakai A, Lawrenson JG, Lawrenson AL, et al. Topical non-steroidal anti-inflammatory drugs for analgesia in traumatic corneal abrasions. Cochrane Database Syst Rev. 2017;5(5):CD009781.
- Puls HA, Cabrera D, Murad MH, Erwin PJ, Bellolio MF. Safety and Effectiveness of Topical Anesthetics in Corneal Abrasions: Systematic Review and Meta-Analysis. J Emerg Med. 2015;49(5):816-824.
- Sulewski M, Leslie L, Liu SH, Ifantides C, Cho K, Kuo IC. Topical ophthalmic anesthetics for corneal abrasions. Cochrane Database Syst Rev. 2023;2023(8).
- Swaminathan A, Otterness K, Milne K, Rezaie S. The Safety of Topical Anesthetics in the Treatment of Corneal Abrasions: A Review. J Emerg Med. 2015;49(5):810-815.
- Waldman N, Winrow B, Densie I, et al. An Observational Study to Determine Whether Routinely Sending Patients Home With a 24-Hour Supply of Topical Tetracaine From the Emergency Department for Simple Corneal Abrasion Pain Is Potentially Safe. Ann Emerg Med. 2018;71(6):767-778.





1 thought on “emDOCs Revamp – Corneal Abrasion”
You missed a good opportunity to discuss ACEP’s new guidelines giving Level B recommendation to discharge these patients home with a short course of a topical anesthetic-
“ Our key observation is that for only simple corneal abrasions, as diagnosed and treated in accordance with the full protocol described herein, it appears safe to prescribe or otherwise provide a commercial topical anesthetic (ie, proparacaine, tetracaine, oxybuprocaine) for use up to every 30 minutes as needed during the first 24 hours after presentation, as long as no more than 1.5 to 2 mL total (an expected 24-hour supply) is dispensed and any remainder is discarded after 24 hours. ”
From:
https://www.annemergmed.com/article/S0196-0644(24)00004-0/abstract