Management of Patients on Novel Oral Anticoagulants with Bleeding
By Christie Sun MD
(EM Resident Physician, Georgetown University School of Medicine/Medstar Washington Hospital Center),
Maryann Mazer-Amirshahi PharmD MD/MPH
(Assistant Professor of Emergency Medicine, Georgetown University School of Medicine/Medstar Washginton Hospital Center)
Edited by Alex Koyfman MD (@EMHighAK) and Stephen Alerhand MD (@SAlerhand)
Introduction
In recent years, novel oral anticoagulants (NOAC’s) have been introduced as therapeutic alternatives to warfarin, the gold standard for anticoagulation. These agents offer significant advantages over warfarin, including less drug and dietary interactions as well as no need for frequent therapeutic monitoring.1-4 There is also evidence that NOAC’s are as effective or even superior to warfarin in reducing the number of strokes and systemic embolic events in patients with atrial fibrillation.2-4 The major drawback to NOAC’s is that their anticoagulant effects are not easily reversed, which complicates the management of patients who present with bleeding, overdose, or with the need for urgent procedures.
Pharmacology and Physiology
NOAC’s currently approved in the U.S. fall into two categories: direct thrombin inhibitors (DTIs) and Factor Xa inhibitors. Dabigatran (Pradaxa®) is a DTI that is FDA-approved for the treatment of venous thromboembolism (VTE) and stroke prevention in the setting of non-valvular atrial fibrillation.5,6 It is a univalent DTI that binds to the active site of thrombin, preventing the conversion of fibrinogen to fibrin.5 Factor Xa inhibitors including rivaroxaban (Xarelto®) and apixaban (Eliquis®) are also approved for the prevention and treatment of VTE as well as stroke prevention. In January 2015, the FDA approved a third agent, edoxaban (Savaysa®). Factor Xa is made up of a prothrombinase complex and these agents bind to the active site of free Factor Xa as well as complex-bound forms to prevent the generation of thrombin.7
Clinical Presentation
The most significant adverse effect of these agents is the development of bleeding complications. Bleeding may present in a variety of clinical contexts, and may range from minor ecchymosis to life-threatening hemorrhage. The more common scenario is the patient who presents with spontaneous bleeding often in the setting of renal insufficiency, although intentional and unintentional overdoses do occur. Reported bleeding events include intracranial bleeding, epistaxis, hemoptysis, gastrointestinal bleeding, and hematuria.8
Diagnostic Testing
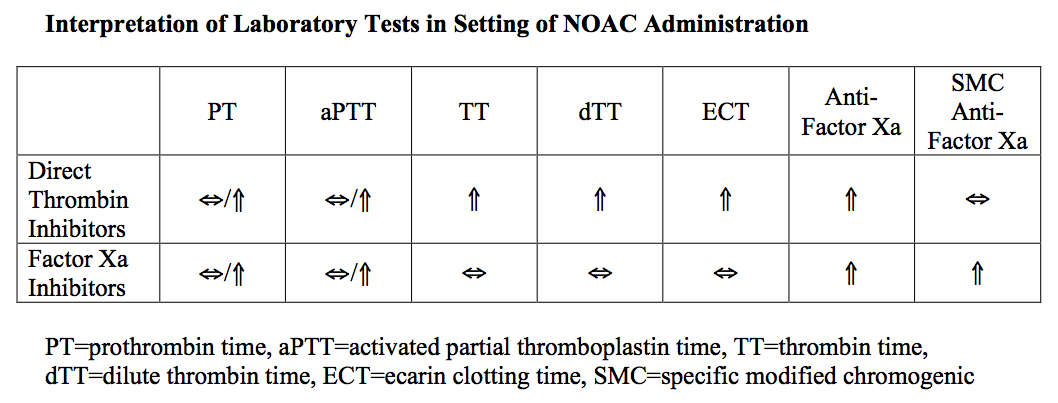
Diagnostic testing for patients presenting with bleeding who are currently taking a NOAC include a basic metabolic panel to determine renal function, baseline and serial complete blood counts, coagulation studies (PT/INR, aPTT), and a type and cross. Interpretation of routine coagulation studies can be difficult in these patients. DTI’s cause an increase in aPTT, but this relationship is not linear and there is a plateau effect at higher drug concentrations. PT can also be elevated in patients taking dabigatran, but measurements do not correlate with toxicity. More sensitive tests for DTI’s include the ecarin clotting time (ECT) and the dilute thrombin time (dTT); however, these tests are not routinely available in most institutions.9 Like DTI’s, factor Xa inhibitors can prolong PT and aPTT, but this does not correlate with clinical toxicity. Anti-factor Xa concentrations will be elevated in these patients. Specific modified anti-factor Xa concentrations correlate well with anticoagulation, but this assay is not routinely available.10 (Table)
Additional diagnostic testing is based on the clinical presentation. For patients with head trauma or altered mental status, a non-contrast head CT should be obtained. The patient should also be assessed for gastrointestinal bleeding and hematuria and other sources of bleeding as guided by history and physical examination. In the setting of an intentional overdose, diagnostic testing should also include evaluation for co-ingestions as indicated.
Interpretation of Laboratory Tests in Setting of NOAC Administration
Management
Patients taking NOAC’s that present with bleeding should be rapidly assessed and stabilized based on the degree of hemorrhage. For patients who present with significant blood loss and hemodynamic instability, packed red blood cell transfusion is indicated. Fresh frozen plasma (FFP) can be used as part of a balanced transfusion strategy but will not reverse coagulopathy. There are limited data evaluating the optimal reversal strategies for NOAC’s. Early consultation with specific subspecialties (gastroenterology, neurosurgery) may be indicated based on patient presentation. Although these medications are bound by activated charcoal, it is of little utility in overdose once bleeding has manifested and may impede endoscopy when indicated.9,11
There are limited options for the reversal of clinically significant bleeding in patients taking dabigatran. Prothrombin complex concentrates (PCC’s), which contain high doses of vitamin K dependent clotting factors as well as Protein C and S, may be effective for dabigatran reversal.11 Hemodialysis has also been shown to be effective in removal of dabigatran in patients with end-stage renal disease, but the benefit of dialysis in patients with normal renal function is controversial.12 There are also logistical concerns surrounding the risks of placing a large bore catheter in patients who are coagulopathic as well as the fact that patients with significant bleeding are often hypotensive and cannot tolerate hemodialysis. Recombinant activated factor VII (rVIIa), typically used in patients with hemophilia, has been raised as an option for non-hemophiliac patients with severe bleeding, but there are limited data supporting its use. Activated PCC (aPCC) also developed for hemophiliac patients, contains activated factors II, VII, IX and X, and has shown complete reversal of lab abnormalities.13 While there are dagibatran-specific reversal agents, they are currently being evaluated in clinical trials and are not yet available outside of study centers.14
In bleeding secondary to Factor Xa inhibitors, the mainstay of reversal is PCC’s. In one study, a single high dose of four factor PCC (factors II, VII, IX, X) reversed the PT prolongation caused by rivaroxaban.15 However, it is unclear if this reversal corresponds to a clinically significant reduction in hemorrhage. The half-lives of these agents may require repeat administration of PCC’s. Both three and four factor PCC’s are available in the U.S. and current data suggests four factor PCC’s may be more reliable in reversing coagulopathy; however, this data is primarily for warfarin reversal.16 There are limited, but promising data examining rVIIa in the reversal of lab abnormalities specifically due to rivaroxaban.17 While there are also specific antidotes currently being researched, none are currently available for commercial use in the U.S.
Conclusions
NOAC’s have significant therapeutic advantages over traditional warfarin therapy. However, these agents may cause life-threatening bleeding complications that are less easily reversed. When bleeding does occur, rapid stabilization, supportive care, and reversal of coagulopathy are the current mainstays of treatment.
References / Further Reading
- Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med 2007; 167:1414-19.
- Bruins Slot KM, Berge E. Factor Xa inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in patients with atrial fibrillation. Cochrane Database Syst Rev 2013; 8:1-84.
- Mousa SA. Oral direct factor Xa inhibitors, with special emphasis on rivaroxaban. Anticoagulants, Antiplatelets, and Thrombolytics. Springer Science + Business Media 2010:181–201.
- Eikelboom JW, Weitz JI. New anticoagulants. Circulation 2010; 121:1523–32.
- Nisio MD, Middeldorp S, Buller HR. Direct thrombin inhibitors. N Engl J Med 2005; 353:1028-40.
- Cheng JW, Vu H. Dabigitran etexilate: an oral direct thrombin inhibitor for the management of thromboembolic disorders. Clin Ther 2012; 34:766-87.
- Samama MM. The mechanism of action of rivaroxaban — an oral, direct Factor Xa inhibitor — compared with other anticoagulants. Thromb Res 2011; 127:497-504.
- Haprer P, Young L, Merriman E. Bleeding risk with dabigatran in the frail elderly. N Eng J Med 2012; 366:864-66.
- van Ryn J, Stangier J, Haertter S. et al. Dabigatran exetilate-a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Throb Haemost 2010; 103:1116-27.
- Samama MM, Contant G, Spiro TE, et al. Laboratory assessment of rivaroxaban: a review. Throm J 2013; 11:11.
- Siegal DM, Crowther MA. Acute management of bleeding in patients on novel oral anticoagulants. Eur Heart J 2013; 34:489-498b.
- Stangier J, Rathgen K, Stahle H, et al. Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open-label, parallel-group, single-centre study. Clin Pharmacokinet 2010; 49:259-268.
- Khoo TL, Weatherburn C, Kershaw G, et al. The use of FEIBA in the correction of coagulation abnormalities induced by dabigatran. Int J Lab Hematol 2013; 35:222-4
- Gomez-Outes A, Suarex-Gea ML, Lecumberri R, et al. Specific antidotes in development for reversal of novel anticoagulants: a review. Recent Pat Cardiovasc Drug Discov 2014; 9:2-10.
- Eerenberg ES, Kamphuisen PW, Sijpkens MK, et al. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation 2011; 124:1573-79.
- Voils SA, Baird B. Systematic review: 3-factor versus 4-factor prothrombin complex concentrate for warfarin reversal: does it matter? Thromb Res 2012; 130:833-40.
- Korber MK, Langer E, Ziemer S, et al. Measurement and reversal of prophylactic and therapeutic peak levels of rivaroxaban: an in vitro study. Clin Appl Thromb Hemost 2014; 20:735-40.
- http://www.ncbi.nlm.nih.gov/pubmed/24466599
- http://www.ncbi.nlm.nih.gov/pubmed/24908445
- http://www.ncbi.nlm.nih.gov/pubmed/24512886
- http://www.ncbi.nlm.nih.gov/pubmed/23786779





1 thought on “Management of Patients on Novel Oral Anticoagulants with Bleeding”
Pingback: emDOCs.net – Emergency Medicine EducationEM in 5: NOACs - Novel Oral Anticoagulants - emDOCs.net - Emergency Medicine Education